
Abstract
The traditional sonographic characteristic used to distinguish polyorchidism (PO) has been its homogeneous echotexture, which is similar or identical to the normal testicle. PO is most commonly found in the left hemi-scrotum but can also be identified in the right hemi-scrotum, inguinal canal, or abdominal cavity. The mediastinum of a testicle represents where the tunica vaginalis and tunica albuginea that encases a testicle folded back in on itself. The identification of a mediastinum in a scrotal lesion implies that testicular tissue is present. This series review presents three cases where PO was identified in the left hemi-scrotum. In addition to the classic homogeneous echotexture that is typically identified in an accessory testicle, a mediastinum was also appreciated in two of the cases, which helped to solidify the diagnosis of polyorchidism.
Polyorchidism (PO), also known as supernumerary testicle (SNT), is a congenital anomaly in which three or more testicles are present. A study by Bergholz and Wenke 1 identified 140 confirmed cases of PO. 1 Although a search through the literature since this time populated several documented cases of PO, it is still considered a rare congenital malformation. 2 The most common site to find an accessory testicle is in the left hemi-scrotum, but a variety of locations, such as the right hemi-scrotum, inguinal canal, or abdominal cavity, are also possibilities.1,3,4 The classic sonographic characteristic used to define an accessory testicle is its homogeneous echotexture, which will be similar to the normal testicles. 3 This is reinforced by all three of the cases in this article. This series review was developed in particular to highlight the possibility that a mediastinum may be identified in an accessory testicle, which was appreciated in two of the three cases presented. This additional sonographic feature often seen in normal testicles may help solidify the diagnosis of PO. 6
Case Report 1
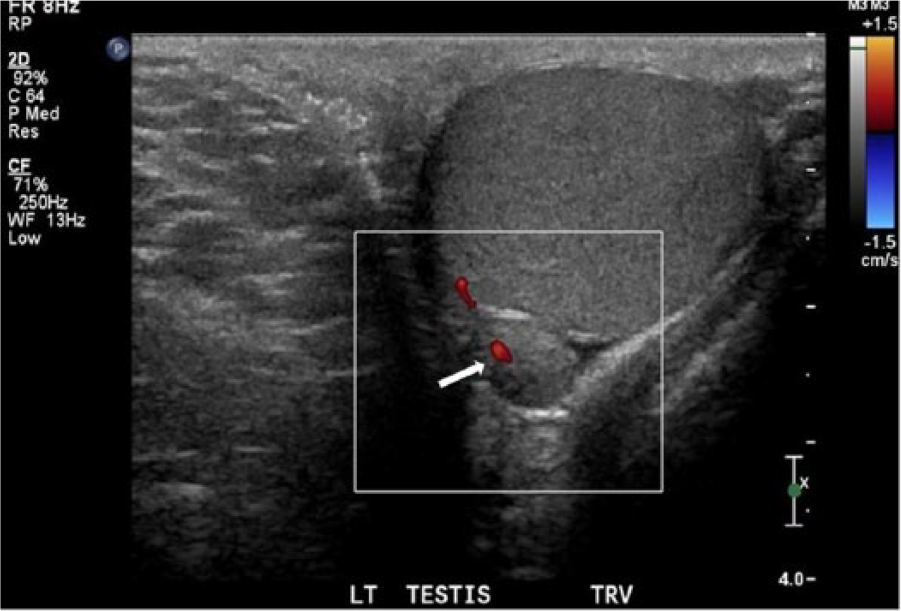
A 38-year-old male was sent for a sonogram by his primary care physician (PCP) to assess the source of right-sided testicular pain. A solid-appearing left epididymal head mass was identified during this initial scan. After meeting with his PCP to discuss the results, the patient was referred to another outpatient imaging clinic for a second opinion regarding the mass. A sonographic examination was performed using a Philips iU-22 ultrasound system (Philips Medical, Bothell, WA) with a 12-5 MHz linear transducer. Sonography confirmed a normal appearing right testicle measuring 5 × 3.6 × 1.9 cm. The left testicle measured 2.7 × 2.2 × 1.9 cm, with the rete testes being noted. Normal low-resistant blood flow was also present in both testicles. Both the right and left epididymis were present and normal. The lesion of interest was identified within the left hemi-scrotum at the level of the epididymal head measuring 1 × 1.1 × 0.9 cm. The mass was of similar echotexture and homogeneity in respect to the normal testicles (Figure 1). Of note, there was a linear band of slightly increased echogenicity within the mass that was suggestive of a mediastinum (Figure 2). Additionally, an arterial waveform was obtained within the mass that showed low-resistant blood flow similar to the Doppler waveforms obtained from the testicles (Figure 3). The radiologist indicated that the left scrotal mass had imaging features suggestive of an SNT.
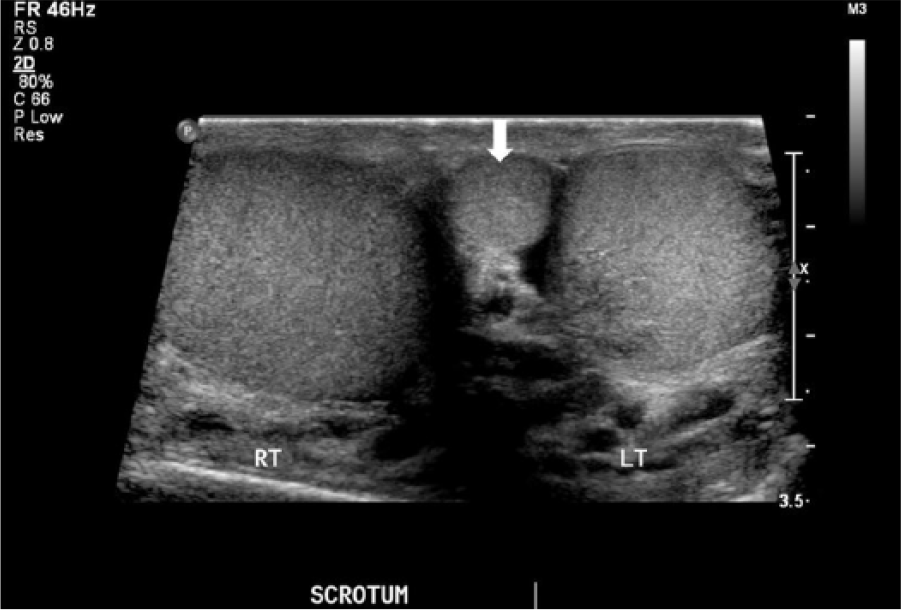
Transverse image of the scrotum demonstrates normal testes with the supernumerary testicle (SNT) medial to the left testicle (arrow). Note the similar echotexture of the SNT compared to the testes.
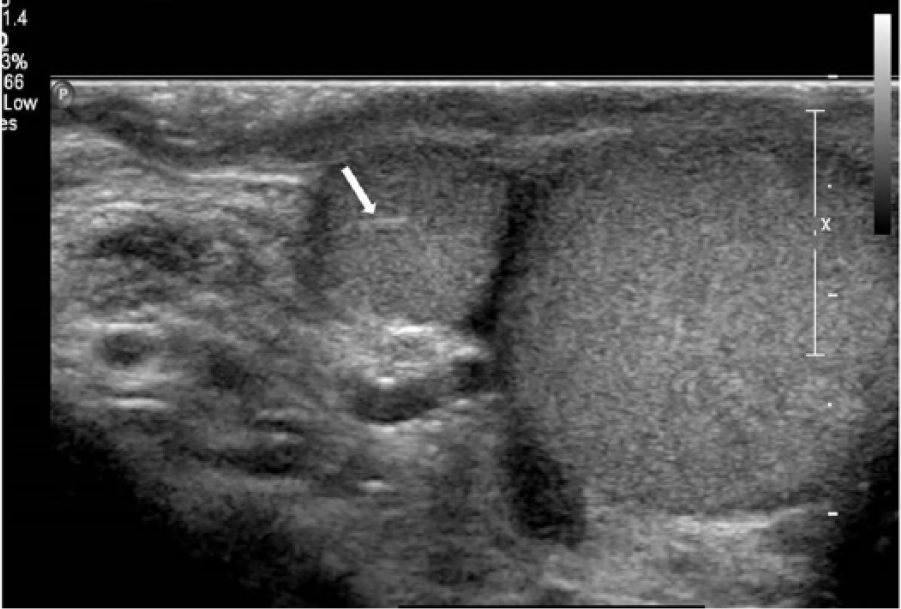
Longitudinal image of the supernumerary testicle showing the slightly echogenic mediastinum (arrow).
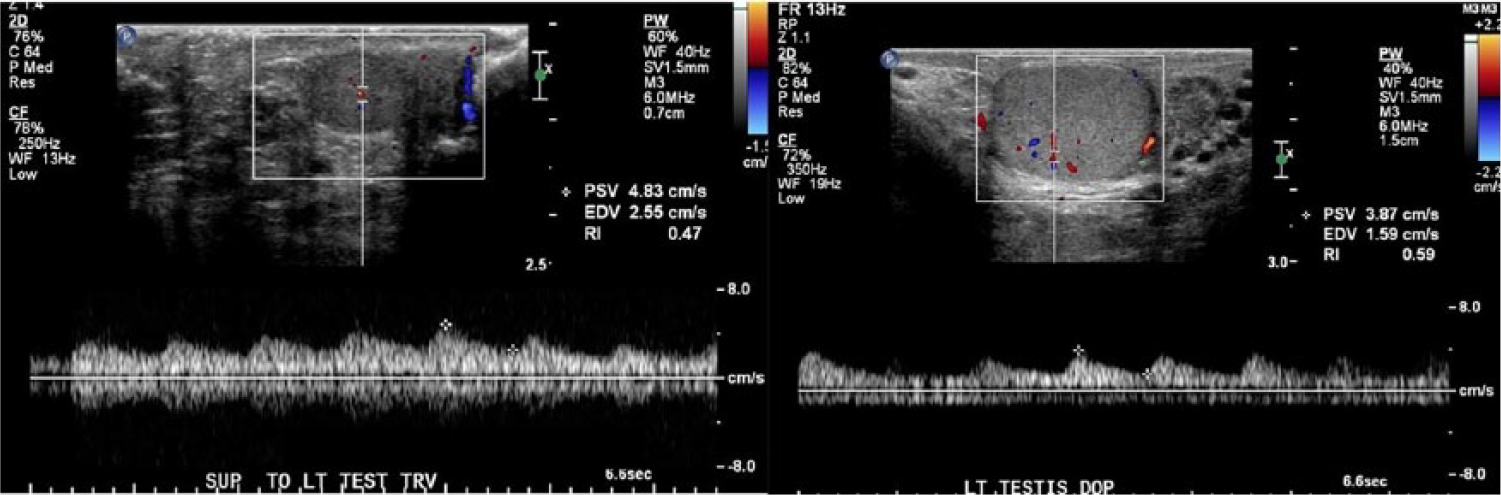
(Left) Doppler flow within the supernumerary testicle (SNT). (Right) Doppler flow within the left testicle. Note the low velocity, low resistant flow in both the left testicle and the SNT.
Following the study, the patient was seen by his provider in the urology clinic where it was decided to repeat the sonogram in 3 months to evaluate for changes and draw tumor markers. The tumor markers came back negative. The follow-up sonogram was performed using a Philips Epiq ultrasound system (Philips Medical) with a 12-5 MHz Linear transducer, which reinforced the findings of PO, where it was again noted that the morphology of the mass resembled the normal testes with a small echogenic mediastinum present. On this exam, it was also documented that a separate epididymis was not visualized and that the SNT was again seen just adjacent to the left epididymal head, suggesting that the SNT and left testicle possibly shared an epididymis (Figure 4).
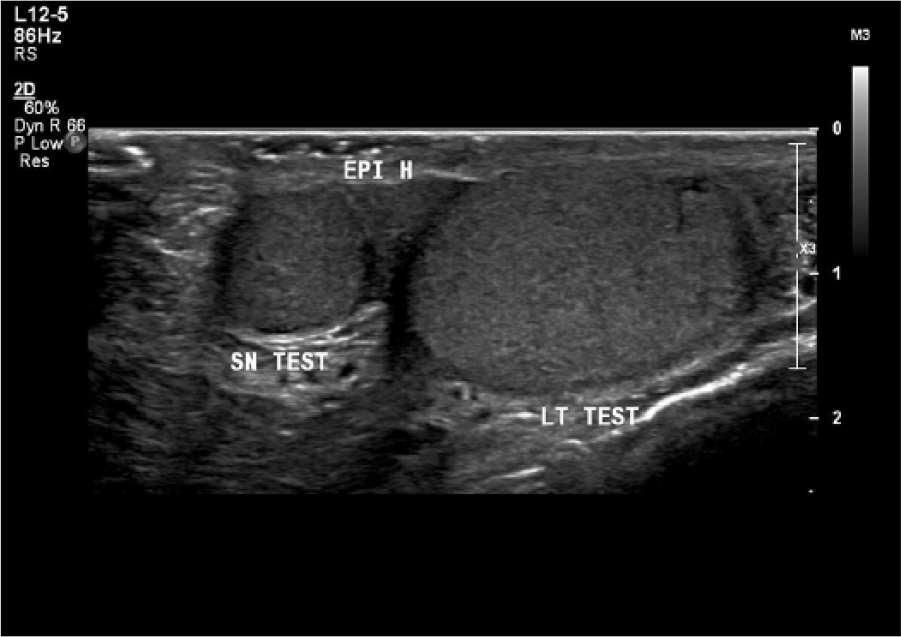
Longitudinal image showing the relationship of the supernumerary testicle (SNT) and left testicle to the epididymis. A separate epididymis was not identified with the SNT, possibly implying a shared epididymis with the left testicle.
Conservative management rather than surgical intervention was decided on as the appropriate course of action after the last sonogram since no concerning sonographic findings were present within the SNT.
Case Report 2
A 46-year-old male with a nontender left testicular lump was referred by his PCP to an outpatient imaging clinic. A scrotal sonogram was ordered to assess the mass. The exam was performed using a Philips iU-22 ultrasound system (Philips Medical) with a 12-5 MHz linear transducer. The right testicle measured 4.1 × 2.5 × 2 cm. The left testicle measured 4.1 × 2.2 × 2.5 cm. Both testicles appeared normal sonographically and had the expected low-resistant arterial waveform pattern. The right epididymis had a normal appearance. An appendix epididymis was noted coursing off the left epididymal head. Adjacent to the left testicle, a 7 × 7 × 5 mm ovoid structure was identified. The mass was noted to have the same homogeneous echogenicity as the left testicle and had what appeared to be a mediastinum (Figure 5). Hilar flow was noted within the mediastinum (Figure 6). A benign lesion most likely representing an SNT was considered as the top diagnostic differential. A resection was offered to the patient by his provider, but a follow-up sonogram was recommended in 2 months as the appropriate course of action.

Transverse image of the left-sided supernumerary testicle demonstrating a mediastinum (arrow).
Transverse image of the left-sided supernumerary testicle demonstrating hilar flow within the mediastinum.
Subsequent sonograms were performed at 2 months and 5 months after the initial examination using a Philips iU-22 ultrasound system (Philips Medical) with a 12-5 MHz linear transducer, which redemonstrated the ovoid mass with internal perfusion and same echotexture as the left testicle. PO remained as the top diagnostic differential. Due to the sonographic appearance of the mass, conservative management was selected as the appropriate course of action and the patient was not seen for 2 years. Upon the patients return 2.5 years from his initial scan, a Philips iU-22 ultrasound system (Philips Medical) with a 12-5 MHz linear transducer was used to perform the scrotal exam, where it was documented that the SNT had only slightly increased in size from 7 × 7 × 5 mm to 10 × 9 × 7 mm. The echotexture of the SNT was consistent with previous exams, and the presence of a mediastinum was again noted. The patient decided to continue with conservative management.
Case Report 3
A 31-year-old male presented to his PCP with a palpable scrotal mass that was initially palpated 4 years prior. The patient felt the lump had grown over the previous 2 years. A scrotal sonogram was ordered to evaluate the mass at an outpatient imaging clinic. The exam was performed using a Philips iU-22 ultrasound system (Philips Medical) with a 12-5 MHz linear transducer. The right testis appeared normal and measured 4.3 × 2.8 × 2.2 cm, whereas the left testis measured 4.5 × 3. 1.9 cm and contained a complex cyst. The palpable lump corresponded to a soft tissue lesion inferior-medial to the left testicle, which measured 2.5 × 1.8 × 2.8 cm in size. The lesion was noted to be separate from the left testicle, within the left hemi-scrotum, and had low-resistance arterial waveform. The lesion was similar in echogenicity as the normal testes but was slightly heterogeneous and patchy, with a small area of increased echogenicity present (Figure 7). The top diagnostic differential for the palpable lump was an SNT based off its location and echotexture. The patchy appearance of the SNT was noted to be abnormal and possibly related to chronic inflammation, ischemia, or infiltrating disease. The results were conveyed to the patient via his PCP. A consult with the urology department was recommended by the PCP, but the patient has not yet followed up.
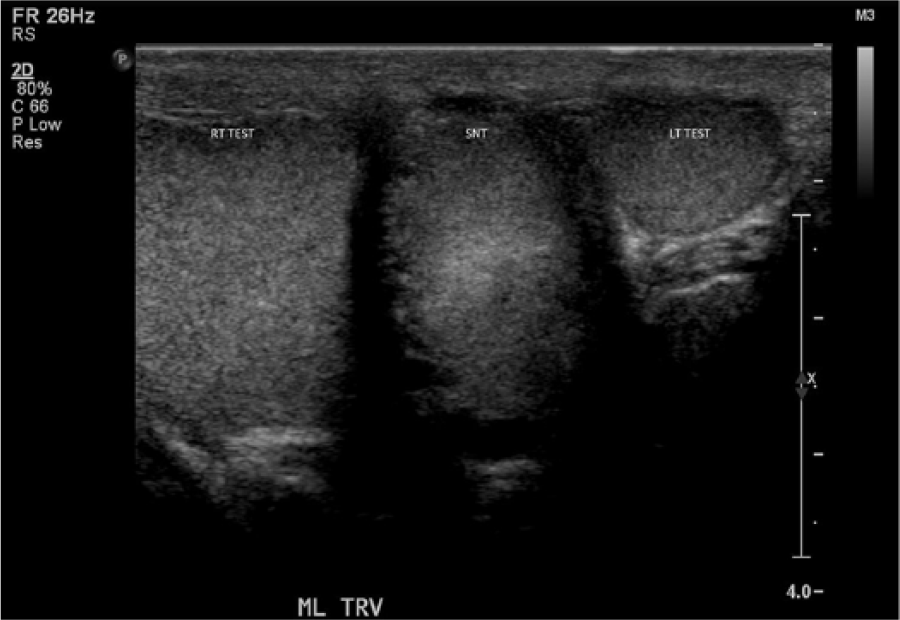
Transverse image of the scrotum showing the supernumerary testicle located between the right and left testicles.
Discussion
The exact etiology of PO has yet to be confirmed, but several theories have been postulated. These include but are not limited to the duplication of the urogenital ridge, the division of the genital ridge by peritoneal bands, and early division of the primitive genital ridge.5–8 Several different presentations of PO have been identified with it not being unusual for an SNT to have a connection to a vas deferens in some capacity. 1 This connection suggests that many cases of SNT have the capability of being functional.1,4
Sonography is the primary imaging modality when evaluating the scrotum for any type of pathology, including PO. 3 The traditional sonographic characteristic used to define PO has been its echotexture, which will be similar to the adjacent testicle.3,4 PO is often seen in the left hemi-scrotum.1,3,4 However, PO can be found in other locations, including the right hemi-scrotum, inguinal canal, and abdominal cavity.1,2 PO has been noted to be an incidental finding in many cases where indicators such as cryptorchidism, torsion, hydrocele, testicular pain, or varicocele were among the primary reasons for the initial investigation. 9 Testicular torsion with PO has been reported to occur in up to 15% of cases as the tunica vaginalis tends to be attached higher than usual, possibly due to the larger testicular volume that passes through the inguinal canal.1,4 PO is typically identified in young adults or adolescents.1,3 The spectral Doppler waveform of normal testicular arteries will show a low-resistant flow pattern, and the appreciation of this type of flow pattern in a suspected accessory testicle may also help aid in the diagnosis of PO.10,11
In two of the three cases presented earlier, the initial indication for a sonogram was to assess a palpable mass that turned out to be an SNT. Only with the first case was the initial indication for an exam a reason other than a palpable mass. Also, all three of these cases differed in that the patients were in their 30s and 40s. The most consistent finding in these cases was the homogeneous, isoechoic echotexture of the accessory testicle to the normal testicle. The presence of what appeared to be a mediastinum was also a useful sonographic feature that helped aid the radiologist, which was seen in two of the three cases. This thin band of slightly echogenic tissue represents where the tunica folds back in on itself and can often be appreciated in a normal testicle. 12 Thus, the presence of a mediastinum implies an association with testicular tissue, helping to confirm an SNT.12,13 A few of the differentials to PO considered by the radiologist in these cases were adenomatoid tumor, appendix testis, or sebaceous cyst. Scrotal calculi and lipomas have also been noted as possible differentials. 3
Historically, management of PO was a surgical resection due to concerns for malignancy. 1 A study performed by Bergholz and Wenke 1 found cancer in only 6.4% of the reviewed cases of PO. However, in all of the cases of PO where cancer was identified, the testicle was undescended. 1 This information would indicate that the risk of cancer may have more to do with cryptorchidism rather than the fact that the testicle is an accessory. 1 Additionally, PO has been estimated to have reproductive potential in up to 65% of cases. 4 Thus, the management of uncomplicated PO is becoming rather conservative.4,9 Improvements in medical imaging have also helped the trend toward conservative management. 1 In the cases presented earlier, a biopsy or resection was offered, but conservative management through sonographic observation was the course of action taken. The attending urologist typically recommended a 2- to 3-month follow-up sonogram after the initial scan indicating PO to verify that no concerning changes occurred. Case two in particular supports the concept of conservative management when no concerning findings are identified on the initial scan as 2.5 years passed between sonographic examinations with no significant change in the SNT.
Conclusion
PO is a rare congenital malformation in which three or more testicles are present. Management for PO historically was the surgical resection of the testis due to concerns for malignancy. With an improved understanding of the process and advanced imaging technology, a more conservative approach is quickly becoming the accepted standard. The sonographic diagnosis of PO has traditionally been based off the homogeneous echotexture of the accessory testicle, which is typically identical to the ipsilateral testicle. In addition to this echotexture, the identification of a mediastinum, which implies testicular tissue is present, can be used as an additional sonographic indicator to help aid in the diagnosis of SNT.
Footnotes
Acknowledgements
The author thanks Teresa Bieker and Julia Drose for their insight with the development of this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.