
Abstract
Splenogonadal fusion (SGF) is a rare malformation that involves immature splenic tissue connecting and adhering to gonadal tissue during embryologic development. SGF is typically diagnosed during surgery or autopsy. This case study reports a case of discontinuous SGF found on sonography with correlative magnetic resonance imaging.
Splenogonadal fusion (SGF) is a rare congenital anomaly that occurs when immature splenic tissue adheres to the developing gonad, epididymis, or vas deferens. The splenic tissue is subsequently pulled in a caudal direction as the gonad descends.1–3 Although this anomaly was first described in 1883 by Bostroem, there have been only approximately 150 cases reported in the literature.4,5 SGF can be continuous, with splenic tissue trailing down to the gonad, or discontinuous, with ectopic splenic tissue or a splenule found fused to the gonad. The findings of the discontinuous type and the use of magnetic resonance imaging (MRI) to differentiate the mass from polyorchidism will be described in this article.
Case Report
A 16-year-old boy presented to a physician with a 3-day history of fever, sweats, nausea, and fatigue and decreased appetite for 1 month. There was concern for possible mononucleosis, viral infection, strep throat, or upper respiratory infection based on the patient’s symptoms. During the office visit, the patient commented on a palpable area within the left scrotum present for the past few weeks, with no associated pain or discomfort. On physical examination, normal right and left testicles were identified in the expected locations, but the left hemiscrotum was found to have an additional mass at the upper portion of the testicle, which was slightly more firm in comparison to the testicle. The two palpable areas within the left scrotum could not be separated, with the mass appearing to be larger than the left testicle. This finding had never been detected on any prior physical examinations, and the patient was referred for scrotal sonography for further classification.
A sonogram was performed using a GE Logiq 9 (GE Healthcare–Ultrasound, Waukesha, WI) with a 9-MHz linear transducer. Both right and left testicles were present and in the expected location along with the normal epididymides. The lateral aspect of the left testicle appeared heterogeneous in echo texture. Adjacent to this area of heterogenicity was an additional ovoid structure that measured 2.9 × 2.2 × 3.0 cm (Figure 1). This area demonstrated similar echotexture, size, and blood perfusion in relation to the left testicle (Figure 2). No epididymis could be identified for the additional structure. These findings suggested the diagnosis of polyorchidism. Differential diagnoses based on the sonographic findings may have also included rhabdomyosarcoma, seminoma, choriocarcinoma, teratoma, germ cell tumor, spermatocele, testicular torsion, and bi-lobed testis.
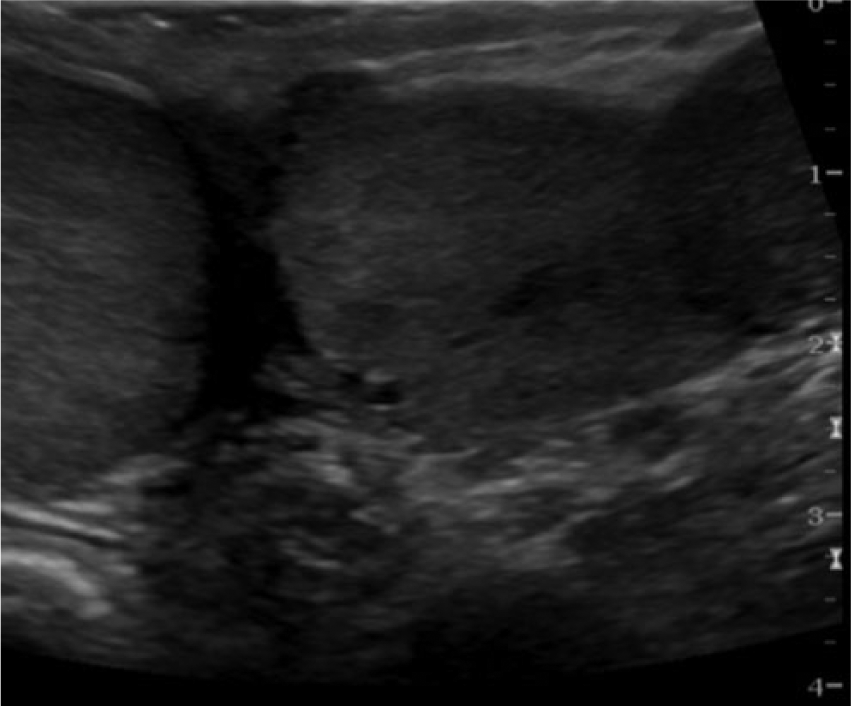
Gray-scale sonogram of the right and left testes. A very nearly isoechoic round solid mass can be seen adjacent to the left testis on the far right of the image.
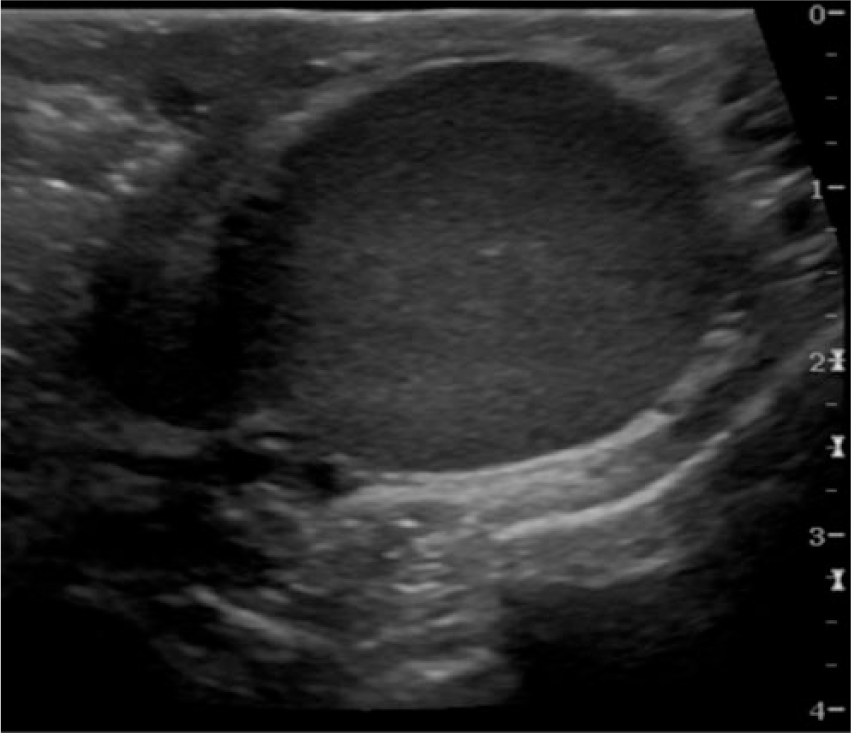
Gray-scale sonographic image of the extratesticular mass. The mass can be seen to have a homogenous echotexture, very similar to that of the adjacent normal testes.
Because of the patient’s age and because the left extratesticular mass was felt to be more firm, rapidly growing, and painless, there was a clinical concern for testicular malignancy. Although the excess tissue in the left hemiscrotum did not appear to have normal appearance of testicular cancer, malignancy could not be excluded. The patient was referred for MRI of the abdomen and pelvis with and without intravenous contrast. The laboratory results for tumor markers came back negative for malignancy.
The MRI of the abdomen and pelvis revealed a homogeneous, circumscribed, ovoid-shaped extratesticular mass anterior to the left testicle. The lesion had isosignal on T1-weighted images (Figure 3) and decreased signal on T2-weighted images compared with the normal testicle and no invasive involvement of the testicle (Figure 4a and b). Since there were different signal intensities appreciated on the MRI, polyorchidism was considered unlikely despite similar echotexture, size, and blood perfusion on the sonography examination. Differential diagnoses based on the MRI findings included rhabdomyosarcoma, liposarcoma, leiomyosarcoma, malignant fibrous histiocytoma, mesothelioma, and lymphoma. Mimickers of rhabdomyosarcoma include inflammatory processes such as pseudo-tumor, adenomatoid tumors, and chronic epididymitis. Based on the patient’s clinical history, it was recommended that the lesion be biopsied and/or excised.
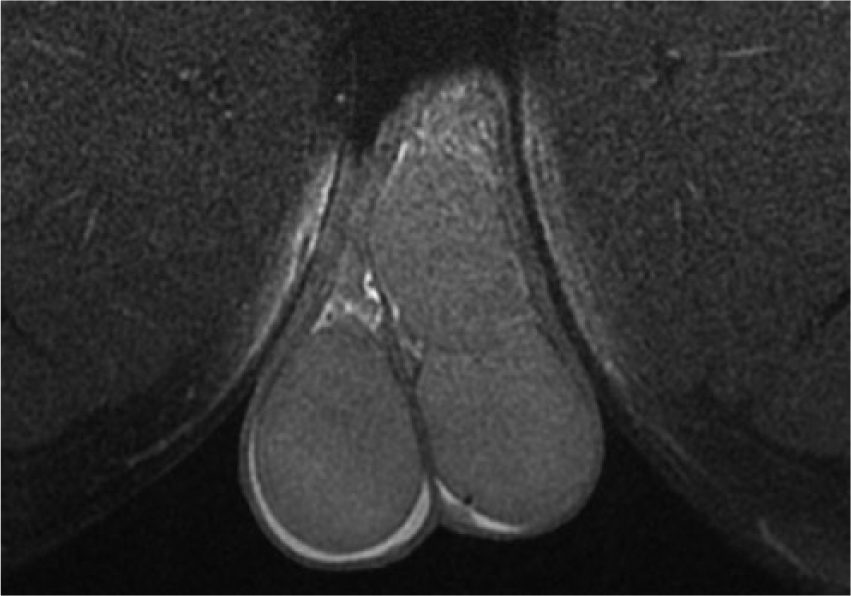
A T1-weighted magnetic resonance image (dark fat image) with intravenous contrast showing a nonenhancing mass superior to the left testis.
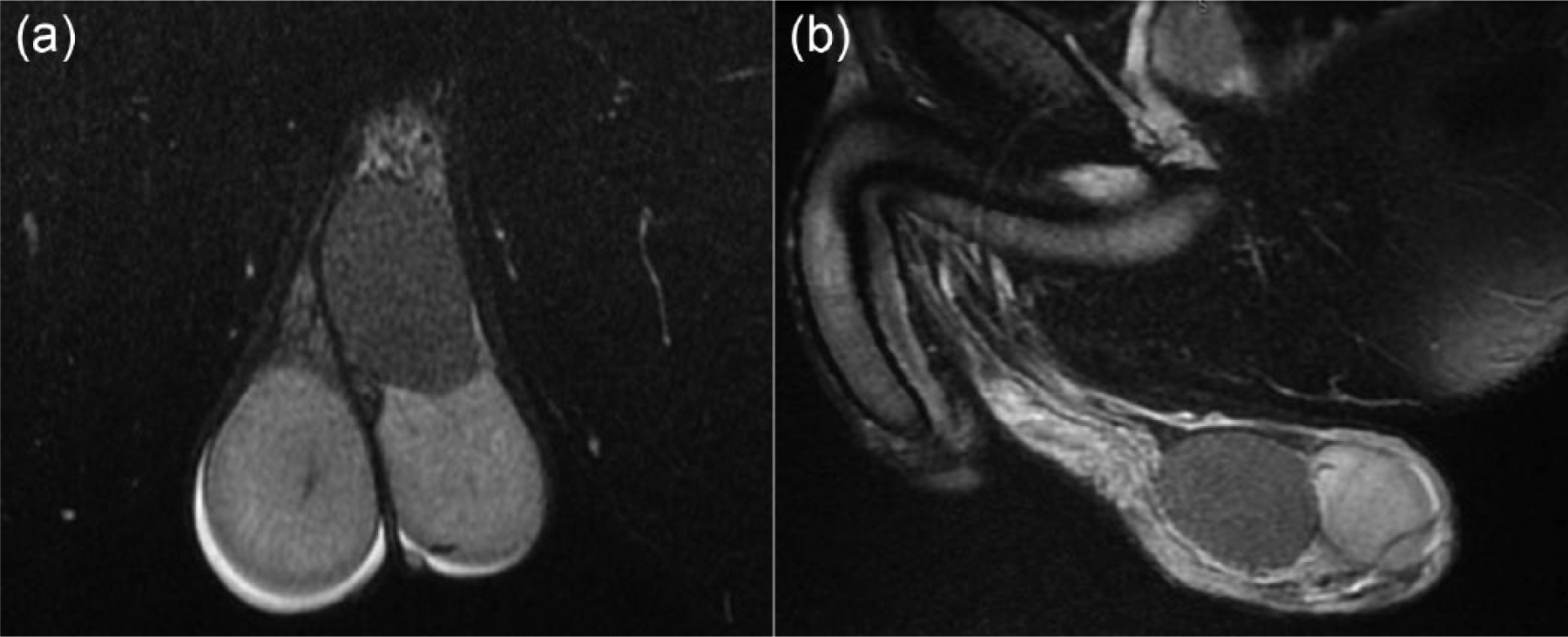
T2-weighted coronal (a) and sagittal (b) magnetic resonance images of the scrotum. The images show a homogenously hypointense, adherent mass superior to the left testis.
Left inguinal exploration was performed, and the gross specimen of the extratesticular lesion appeared to be malignant as it was firm and black in color (Figure 5). The mass was entirely contained within the left hemiscrotum. It was noted to be contiguous to the superior aspect of the left testis and appeared to be contiguous with the vas deferens and spermatic cord. Because of the malignant appearance of the mass, biopsy or excision was not considered for fear of tumor spillage, and a radical left orchiectomy was performed. Because of the patient’s age, back-table harvest of normal left testicular tissue for sperm preservation was also performed.

A gross specimen photograph of the excised testicle (lighter brown) and the adjacent mass (darker brown).
Histologic evaluation of the extratesticular mass showed normal splenic tissue adherent to the testicular parenchyma, consistent with discontinuous splenogonadal fusion with no evidence of malignancy. The specimen of tissue from the normal left testis revealed very few healthy viable sperm upon freezing of the specimen. It was unclear whether this was an overall reflection of poor spermatogenesis or if it reflected poor sperm production from the single left testis due to the splenogonadal fusion.
Discussion
SGF is a rare congenital abnormality that is most commonly found incidentally during surgical exploration for an inguinal hernia or orchiopexy.4,5 This abnormality involves immature splenic tissue being fused with the testicle, which occurs embryologically around the fifth to eighth week of gestation. During this time, an insult can occur that causes the embryonic splenic anlage to fuse with the developing gonadal ridge. During typical testicular descent into the pelvis (around the 8th to 10th week of gestation), the fused splenic tissue can be pulled down along with the gonad (Figure 6). 6
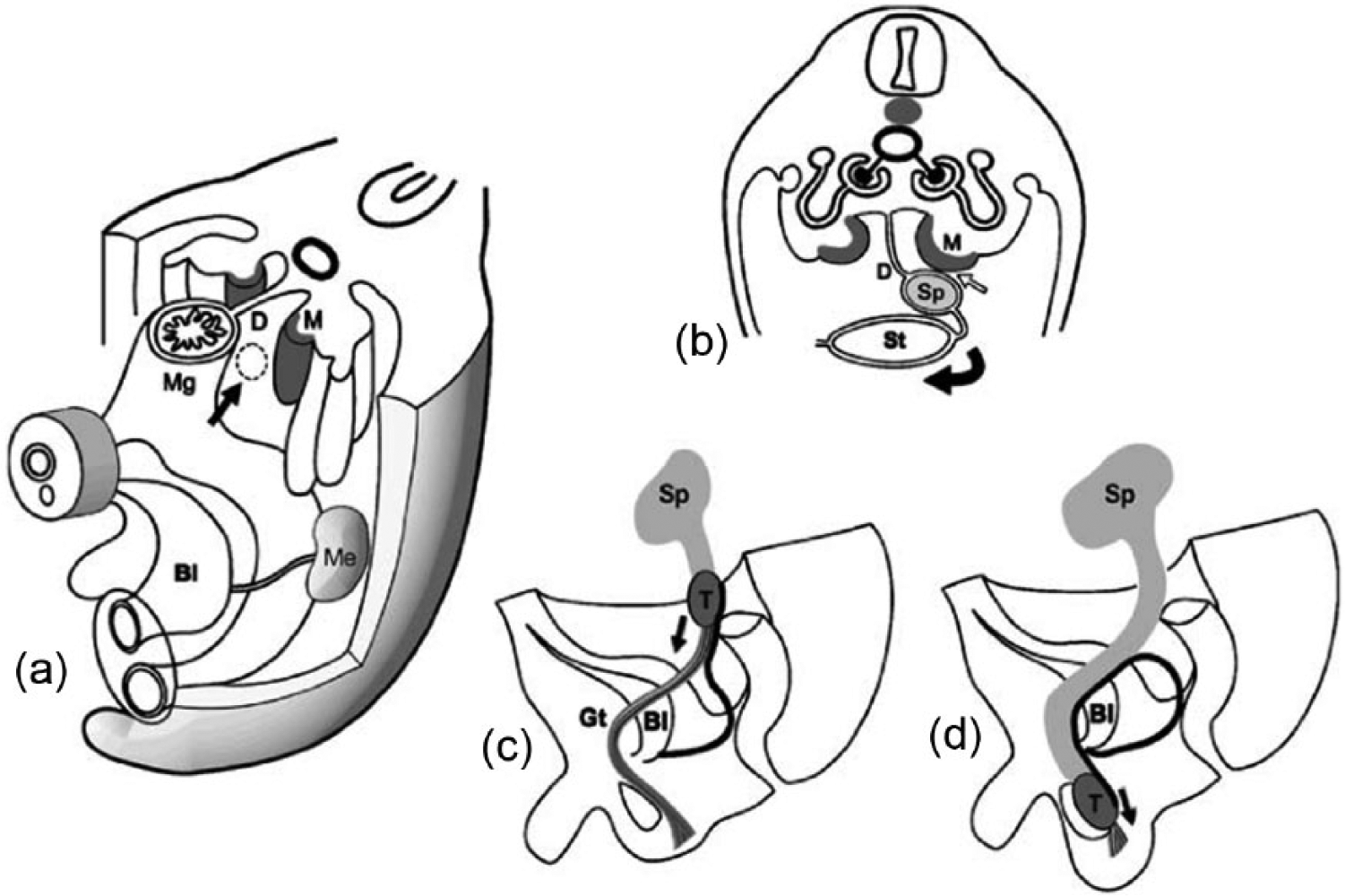
Schematic drawing of the embryology of continuous-type splenogonadal fusion. (a) The spleen (arrow) develops within the dorsal mesogastrium (D). (b) Fusion (small arrow) of the developing spleen (Sp) to the mesonephros (M) during rotation of the stomach (St, curved arrow). (c) Descent of the testis (T, arrow) that has developed from the mesonephros results in descent of a portion of the spleen (Sp) along with it. (d) The aberrant splenic tissue extends up to the root of the scrotum. Mg, midgut; M, metanephros; Bl, bladder; Gt, gubernaculum testis. Reprinted with permission from Varma DR, Sirineni GR, Rao MV, et al. Sonographic and CT features of splenogonadal fusion. Pediatr Radiol. 2007;37:916–919.
There are two types of SGF: continuous and discontinuous. Continuous SGF involves a piece of splenic tissue being pulled down with the testicle during descent, and this ectopic piece of splenic tissue remains attached to the orthotopic spleen (Figure 7). 4 The discontinuous type involves an ectopic piece of splenic tissue attached to the gonad; however, with this type, there is no connection between the ectopic splenic tissue and the main spleen. 7
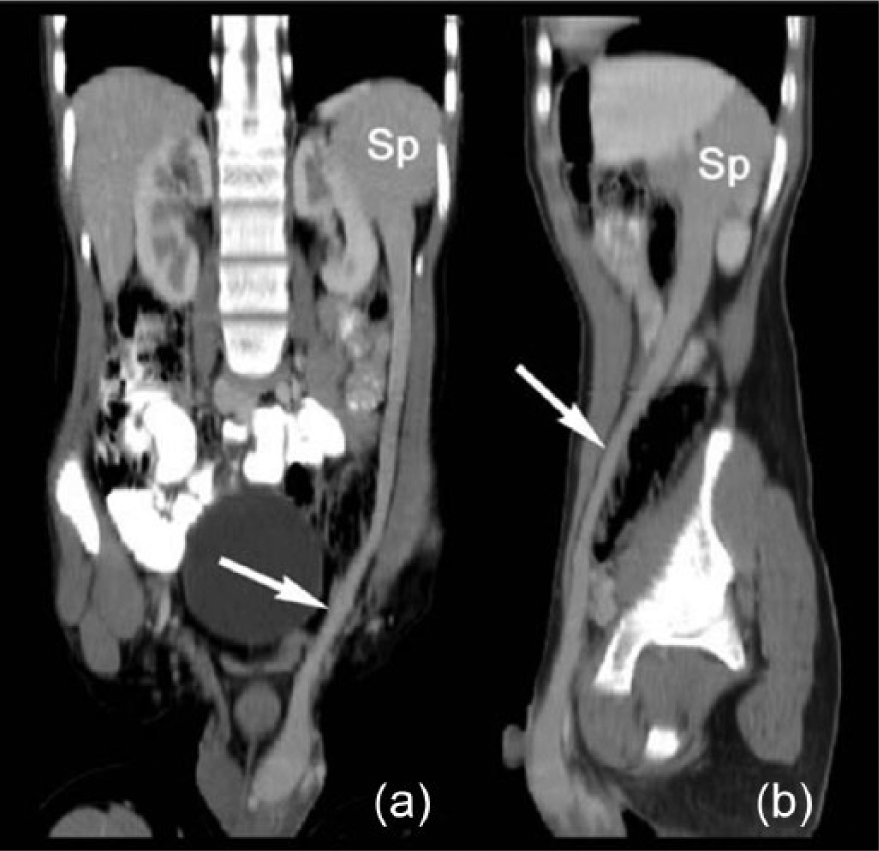
Curved planar reconstructions from a computed tomographic scan of the abdomen showing a case of continuous-type splenogonadal fusion. The course of the aberrant splenic tissue (arrow) from the native spleen (Sp) to the scrotum is demonstrated. Reprinted with permission from Varma DR, Sirineni GR, Rao MV, et al. Sonographic and CT features of splenogonadal fusion. Pediatr Radiol. 2007;37:916–919.
SGF can be associated with congenital gonadal and inguinal problems to include cryptorchidism and inguinal hernia. These problems most likely arise because SGF can cause problems with normal gonadal descent and closure of the processus vaginalis. 6 Along with the above congenital problems, there have also been reports of other congenital anomalies associated with SGF, including cleft palate, spina bifida, anal abnormalities, microgastria, cardiac anomalies, thoracopagus, craniosynostosis, lung anomalies, and diaphragmatic hernia. These anomalies have been found in approximately 33% of patients who have had the continuous type of SGF. The discontinuous type does not appear to have the same anomalies associated with it.5,6
In the literature, reports of the two types appear to occur equally; approximately 98% of reported cases occur on the left side.5,6 The male-to-female ratio is 16:1, which could be due to the fact that the testicle is easier to access for palpation in comparison with the ovary. Overall, there have been approximately 150 cases of SGF reported in the literature, and most cases have been found in the first two decades of life.1,5
Patients with SGF most commonly present with left inguinal hernia, cryptorchidism, painless swelling of the testis, or a mass palpated in the left scrotum.1–5 Less common symptoms can include painful scrotal swelling related to exercise, mumps, mononucleosis, malaria, or leukemia. Rare reports have been made of patients presenting with bowel obstruction or ectopic splenic tortion or rupture. These types of symptoms can be related to complications of the fusion of the spleen to the gonad.1,4
There are a number of differential diagnoses in males in addition to the possibility of SGF, including orchitis, epididymitis, testicular malignant tumor, polyorchidism, hematoma, or hemangioma.1,8 Typically, SGF may be an incidental finding during sonography, but the sonographic appearance is not specific.9–12 For the case presented above, given the sonographic appearance of the mass, the initial diagnosis was felt likely to be polyorchidism. MRI proved that this was not the case, particularly by the T2-weighted image,6,12 but it did not specifically confirm a diagnosis of SGF. One can diagnose SGF nonsurgically through a technetium-99m sulfur colloid scintigraphy study 12 ; otherwise, most cases are confirmed during surgical exploration, in which the testicle is typically removed.1,5,6,12
Conclusion
SGF is a rare congenital anomaly that should be considered as a possible differential diagnosis of left extratesticular scrotal mass. Including this rare entity as a possible finding could save the patient a trip to the operating room and prevent an unnecessary orchiectomy.
Footnotes
Acknowledgements
The authors would like to thank the University of Wisconsin Hospital and Clinics Ultrasound Department for allowing the authors to use this case for publication and Dr Yonker Wang for his expertise in reading and interpreting this case.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.