
Abstract
The purpose of this study was to compare the disinfection rate of a laboratory environment before and after glow powder exposure and training of sonography students (n = 23) and establish if glow powder was an effective teaching technique for infection protection and control (IPC). Fourteen locations at four scanning stations were contaminated with glow powder, visible under ultraviolet light. Students were shown contaminated areas and debriefed on the importance of disinfection. This activity was repeated to ascertain effectiveness of the training. In total, 204 areas were examined for contamination. Observation 1 revealed 21 locations (30.8%), and observation 2 detected glow powder on 12 locations (17.6%). Overall decrease in contamination rate was 13%. The gel bottle was the most frequently contaminated. The curved 3.5-MHz transducer was consistently cleaned. Disinfectant spray, time gain compensation, bed, stool, screen, and handles of the machine remained contaminated. Students’ IPC increased significantly after glow powder training, and secondary spread was reduced by 16%.
Keywords
Health care–acquired infections (HAIs) are a significant problem in hospitals and medical facilities and have a substantial effect on the health of the population. A HAI is an infection acquired by a patient 48 to 72 hours after treatment at a hospital or other health care facility. 1 It is a major contributor to morbidity, mortality, quality of life, and drug-resistant bacteria1–3 and carries significant financial cost to care for hospitalized patients, nearly $45 billion annually. 4 The Centers for Disease Control and Prevention (CDC) reported 687,000 patients with HAIs, and 72,000 patients with HAIs died while hospitalized in 2015. 5 HAIs can occur due to human error or equipment failure. 6 Proactive measures can be implemented in all health care settings to reduce the risk of HAIs. The US Department of Health and Human Services (HHS), in tandem with the Agency for Healthcare Research and Quality, have made infection protection and control (IPC) a priority for patient safety. 7 The Joint Commission identified reducing risk of HAIs as Goal 7 in the 2018 National Patient Safety Goals. 8 One of the areas it identified as essential for preventing the spread of HAIs included proper cleaning and disinfection of patient care equipment and the environment.
Diagnostic medical sonography is a commonly used imaging modality to aid in medical diagnosis and treatment. Many do not realize sonographers, the sonographic work environment, patients, and machines can be a source of infection or potential vectors for transmission of disease.9–11 Pathogens are present in the environment and on many people, even when surfaces appear clean and people present with no symptoms. The sonography department has a high volume of patients who may harbor illness and disease. Because ultrasound equipment is in direct contact with the patient’s skin, there is potential for transmission of pathogens to or from patients, health care workers, or inanimate surfaces in the environment.12–14 A sonographer should practice proper hand hygiene, wear gloves when in contact with patients, and also maintain a clean environment. After every patient is examined, the conductive gel should be wiped off the transducer and cleaned. The cables, docking stations, keyboards, screens, and transducers all have potential to carry bacteria and be a source or vector of infection, as do laboratory coats worn by practitioners. Infectious agents and blood have been found on the ultrasound equipment in operating rooms, intensive care units, and emergency departments. 12 Studies have described the risks of cross-transmission by health care workers touching inanimate objects such as medical charts, bedrails, equipment in the patient zone, or contaminated gel bottles.12,14 Although it is understood that equipment should be adequately cleaned and disinfected, there are many opportunities for noncompliance, inadequate compliance, or simply lack of knowledge in proper use of products. If special cleaning procedures are not performed on equipment correctly or disinfectants have expired, the equipment will not be adequately prepared. Because there are a variety of disinfection products, methods, and techniques, confusion may exist regarding appropriate disinfection techniques for sonography equipment. In addition, this information and the availability of products are always changing.
Although there is limited evidence regarding transmission of infection to patients due to poor sonography cleaning techniques, methicillin-resistant Staphylococcus aureus, Pseudomonas, Acinetobacter species, Candida albicans, hepatitis B and C viruses, and human papillomavirus have been detected on the ultrasound equipment.10,15 Studies that cultured samples taken from transducers in hospitals reported findings of bacteria, fungus, blood, and microbial contamination in generally low-risk areas.12,16 While there are suggested guidelines by the American Institute of Ultrasound in Medicine (AIUM), the Australasian Society for Ultrasound in Medicine, and the World Federation of Ultrasound in Medicine and Biology regarding disinfection of transducers, there is a lot of ambiguity and a range of practices found across countries, hospitals, and even within institutions.3,17 Unfortunately, there is no recommended cleaning practice for the patient zone or sonography laboratory. 18
Rationale
De Jong 6 described the importance of educating sonographers about IPC and the role that sonographers and students can play in preventing HAIs. Measures for IPC should protect patients and sonographers. While handwashing is the first step in reducing HAIs and preventing transmission of bacteria and pathogens from patient to patient, it is equally important to maintain a clean sonography department. Despite increased awareness and national HAI action plans by the HHS, 1 in 25 hospitalized patients still acquire HAIs. 19 Many are unaware of the risks for transmission of pathogens in a sonography suite. It is imperative sonographers and students be properly educated regarding the unique challenges of maintaining clean equipment and work environment. IPC may not be emphasized enough in many health care training programs.
Significance
The HHS noted that when protocols for IPC were implemented, HAIs could be reduced by 70%. 20 No specific infection prevention protocols have been established as being most effective, and none have been tailored for the sonography work environment. By having students learn and apply proper IPC procedures, they develop better habits and teach others to disinfect equipment and the work environment, as well as prevent transmission of disease.
The purpose of this study was to ascertain if using glow powder (Glo Germ Powder; Glo Germ Company, Moab, Utah) could be an effective teaching tool to help students understand the importance of IPC. Glow powder was used as a visual tool to demonstrate how germs spread when students did not practice proper infection prevention techniques (see Figure 1). The purpose of the activity was to promote application of knowledge and compliance with IPC techniques through experiential learning. There is a significant gap in the literature addressing best practices for teaching IPC techniques and protocols for a sonography department. 18

Ultrasound equipment with glow powder under normal lighting (left) and ultraviolet lights (right).
Methods
This study was a quasi-experimental prospective study that measured and evaluated the effect of a purposively applied intervention that involved contamination of laboratory equipment with Glo Germ powder and debriefing. Glow Germ powder consists of powder-based simulated germs, which glow under ultraviolet (UV) light. It is a product approved by the CDC to teach handwashing and aseptic techniques. Glow powder is available in liquid, gel, and powder form, and it washes off with adequate soap and water.
The study population was derived through a purposive sample of convenience, including students enrolled in a college imaging program (n = 23). Study participants consisted of first-year sonography students who received instruction and training on IPC as part of a course curriculum. These students were enrolled in a sonography course with a scan laboratory component at the time of the study. Students did not receive any grade, reward, or penalty for participation.
The student scan laboratory was contaminated with glow powder at four different scanning stations on specific locations at each station, prior to a scanning session, without student knowledge. The researcher documented the initial location of the placement of glow powder. After a scanning session, students were notified the laboratory was contaminated with germs and shown the areas of contamination using an UV light. The instructor reviewed areas originally contaminated and those that remained contaminated after the students used the laboratory. A debriefing session was conducted to explain that the glow powder represented fake simulated germs as well as highlight the importance of proper infection control. The instructor pointed out the specific vulnerable areas. This activity was repeated later in the academic year to ascertain if the glow powder and debriefing activity had an effect on compliance with IPC protocols.
The laboratory was evaluated for the presence or absence of contamination represented by glow powder. When powder was detected with the UV light, it was documented on the worksheet at baseline, after observation 1, and after observation 2. Data (detection of glow powder) were observed and recorded from multiple sites at all four stations in the student sonography scan laboratory. Each station was equipped with a stool, stretcher, sonography machine, gel bottles, transducers, and disinfection spray. These data were then collated and entered into SPSS, using SPSS Statistics Version 24 software (SPSS, Inc, an IBM Company, Chicago, Illinois) for statistical analysis. Descriptive statistics were used to analyze the data for this study. Normality tests were not conducted because this study collected nominal data and nonparametric testing was used. Frequency and percentages were tabulated for observation 1, observation 2, and the total numbers of contamination sites. A set of summary scores was used to report the overall contamination rate, which compared observation 1 to observation 2. The Excel chi-square tool was also used to evaluate the difference and significance between glow powder detection seen during observation 1, observation 2, and baseline.
This study was reviewed and approved by the Institutional Review Boards of State University of New York Downstate Medical Center and A. T. Still University.
Results
Fourteen locations distributed across four scanning stations in the student scan laboratory were contaminated at baseline with glow powder. Sixteen objects at each station were evaluated for exposure to fake germs (glow powder) and secondary spread. Secondary spread was defined as a location that was not originally contaminated at baseline but then acquired detectable glow powder. In total, 204 areas were identified and evaluated for contamination over three sessions: baseline, observation 1, and observation 2 (68 each time). Data were observed and recorded from multiple sites in the student sonography scan laboratory (see Tables 1–3).
Data Collection Sheet for Glow Powder Detection in Student Scan Laboratory, at Baseline.
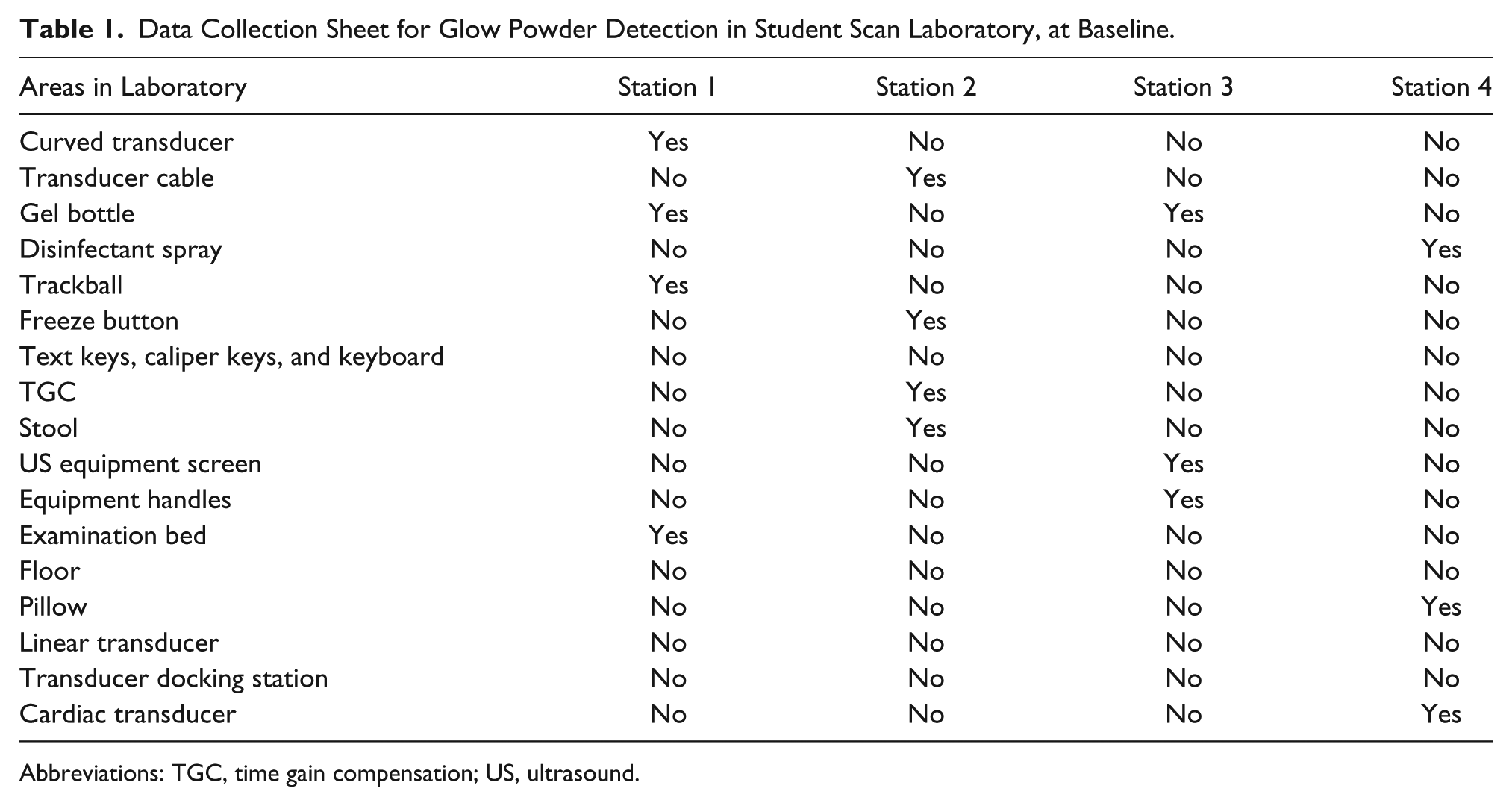
Abbreviations: TGC, time gain compensation; US, ultrasound.
Data Collection Sheet for Glow Powder Detection in Scan Laboratory, First Observation.
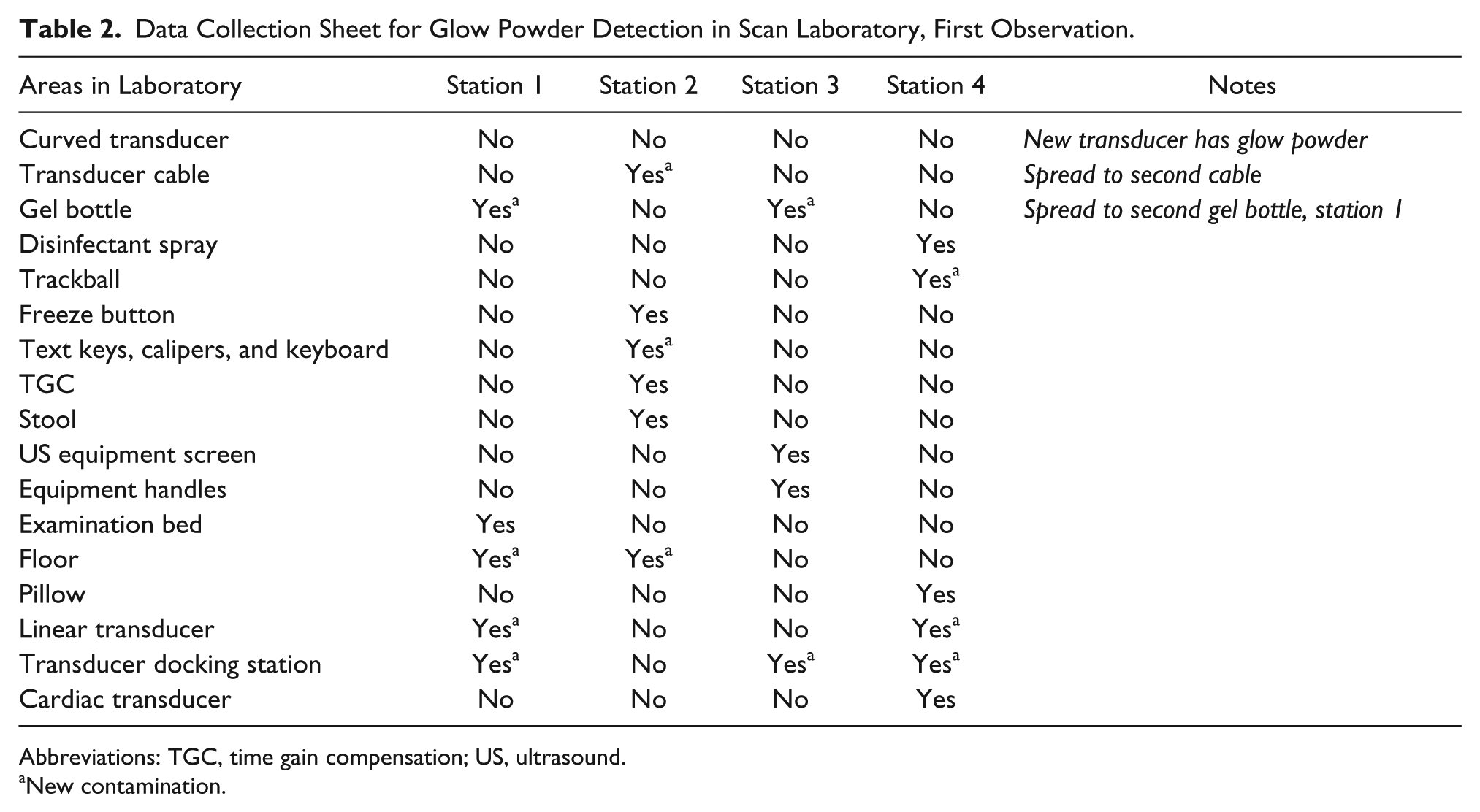
Abbreviations: TGC, time gain compensation; US, ultrasound.
New contamination.
Data Collection Sheet for Glow Powder Detection in Scan Laboratory, Second Observation.
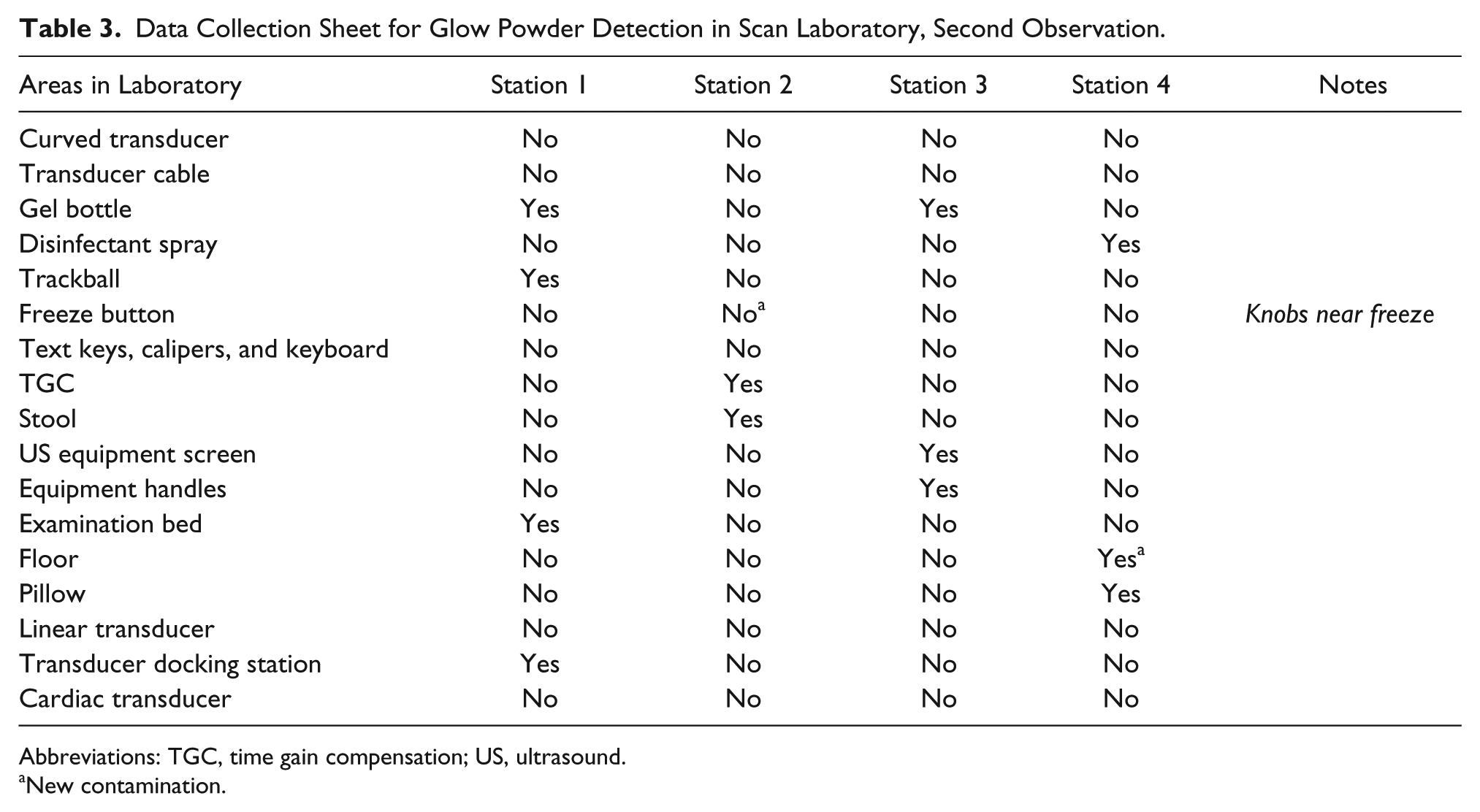
Abbreviations: TGC, time gain compensation; US, ultrasound.
New contamination.
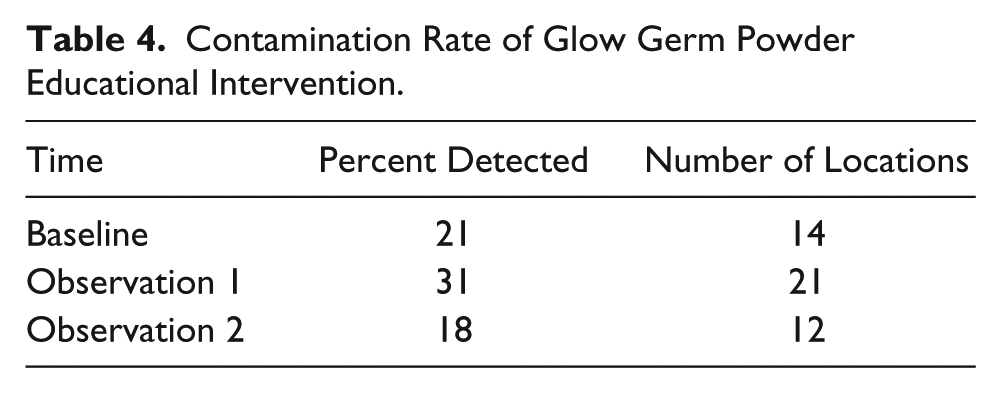
While the baseline collection included 14 areas of contamination with glow powder, observation 1 yielded 21 locations and observation 2 demonstrated detection of glow powder contamination on 12 locations (see Table 4). The descriptive report of frequency and percentages of contamination were documented during the two separate student scan laboratory sessions. The percentage of originally contaminated areas was calculated and compared with baseline, observation 1, and observation 2. The overall decrease in contamination rate after the glow powder demonstration and debriefing activity demonstrated a 13% reduction in contamination.
Contamination Rate of Glow Germ Powder Educational Intervention.
Primary Site of Contamination: Equipment
Students consistently cleaned the curved 3.5-MHz transducer. On both occasions, it was originally contaminated with glow powder, and during both observations 1 and 2, it was found to be clean (see Figures 2 and 3). This is the transducer most frequently used by students and sonographers for general sonography and is generally in direct contact with patients’ skin. Students demonstrated appropriate attention to cleaning this piece of equipment. The cardiac transducer was contaminated at baseline at one station, despite the fact that this group of students did not perform cardiac scanning. During observation 1, it was still contaminated, but after the debriefing session and demonstration of contamination with glow powder, the cardiac transducer was cleaned at observation 2. The item most frequently contaminated was the gel bottle.

Testing the curved 3.5-MHz transducer: baseline demonstrates glow powder (left); observation 1 demonstrates a lack of glow powder (right).

Testing the curved 3.5-MHz transducer: baseline demonstrates glow powder (left); observation 2 demonstrates a lack of glow powder (right).
Items that remained contaminated throughout both scanning sessions were gel bottles, disinfectant spray, TGC controls, the ultrasound equipment’s screen, the handles of the equipment, a stool, pillow, and an examination table.
Secondary Spread of Contamination
In a possible lapse in proper infection control prevention, items that were not initially contaminated subsequently acquired simulated germs (secondary spread). The items with secondary spread included the transducer docking area, linear transducers, text keys on the keyboard, gel bottles, transducer cables, and the floor. During observation 1, three of four stations demonstrated new contamination of the docking station as well as two stations that demonstrated a spread of contamination to the linear array transducer. It is uncertain if gel bottles, disinfectant spray, or another transducer contaminated the docking station. It is likely the contaminated docking station caused further contamination of the linear transducer. Glow powder also spread to another gel bottle and cable of the transducer. Detection of secondary spread of glow powder during observation 1 and observation 2 was noted (see Table 5). Secondary spread was significantly reduced after the glow powder intervention, with only two locations identified during observation 2. Those items that were identified as having new secondary spread detection of glow powder were the floor and one machine’s keys on the keyboard. The items identified were compared to the 13 initially detected, prior to the glow powder intervention and debriefing.
Secondary Spread of Glow Powder During the Educational Intervention.
The results reported reflect an identification or lack thereof of glow germ powder on 68 locations over three periods (n = 204). An example of a location that demonstrated glow germ powder at baseline and after a scanning session can be seen in Figure 4. Incidentally, a spread of glow powder on a pair of shoes, a cellphone, two pairs of pants, and a coat belonging to students was also noted. Glow powder also spread to two of the privacy dividers separating the scanning stations. While students were trained to clean the ultrasound equipment and accessories, it was noted that routinely mopping floors or cleaning privacy screens was not completed unless biohazardous material had been splashed during a sonogram.

Testing the trackball: baseline demonstrates glow powder (left) and observation 2 demonstrates residual glow powder (right).
Detection of glow powder contamination was 31% during observation 1 and 18% during observation 2. To establish a measure of significance, Excel was used to aggregate total new contaminations and total removed, subtracting observation 1 from baseline and comparing it to observation 2 minus baseline. Using the Excel chi-square tool, observation 1 differed from observation 2 with a P value of <.00, which demonstrated that using glow germ powder with debriefing was an effective method to educate sonography students. It also resulted in a better practice of infection control techniques.
Discussion
Disinfection of ultrasound equipment can be one of the most significant methods used in preventing the transmission of infection to patients. Sonography students learn cognitive, affective, and psychomotor skills during training, with an emphasis on knowledge of anatomy, pathology, and clinical skills. IPC techniques and prevention of infection are a small part of an extensive curriculum. There is a significant need to ensure sonographers and students are knowledgeable in IPC techniques and practice proper disinfection to provide safe care for patients while preventing HAIs.6,18 The best time to educate and establish these routines is during training. The purpose of this study was to determine if using glow powder and a debriefing session was effective in conveying this important message and that it translated into better practice. Glow powder has been noted to be an effective tool for training nurses in standard precautions. 21
The results of this study revealed contaminated ultrasound equipment was a potential avenue for infection transmission. It demonstrated that an educational intervention, with glow powder and debriefing, could increase awareness and the need for proper disinfection of the sonography work environment. Most significantly, the study was able to identify areas most commonly missed for disinfection. This information could play an important role in the development of training exercises that teach and reinforce proper IPC practices. 14
Few studies have been conducted on the outcomes of IPC training because they are so difficult to measure. However, the most successful IPC training initiatives were believed to be due to a multimodal and motivational approach. 22 Monistrol et al. 23 described a successful multimodal approach using face-to-face seminars, a UV light activity with fluorescing lotion, leaflets, and signage. Their work demonstrated increased overall health care worker hand hygiene compliance by moving from 54.3% in the preintervention to 75.8% in the postintervention. 23 Wiles et al. 24 also described success with multimodal activities in training nursing students. Sonography students are taught about infection control during their coursework using lecture and discussion. The students in this study were also required to report on the practices they observed at their clinical rotation sites, as well as research the products and describe proper usage and application. This project allowed students in the present study to apply their knowledge to the student scan laboratory.
The students in this study were actively engaged in scanning during the laboratory sessions but did not adequately disinfect all laboratory surfaces prior to the educational glow powder intervention. The students were knowledgeable regarding transducer disinfection but were not cognizant of the importance of cleaning keyboards, gel bottles, and docking stations. It has been demonstrated that cables, keyboards, screens, and examination tables can be breeding grounds for bacteria and viruses,1,9,10,12,25 so this was the rationale for evaluating these areas for contamination. These areas are not currently included in the Cleaning and Disinfection official statement by the AIUM, 26 but this study’s findings regarding contamination on keyboards, cables, and gel bottles were consistent with other studies.3,25 Westerway and Basseal 27 reported more people cleaned the transducer cables than the keyboards, and only 10% cleaned the keyboard after every patient. Even when the transducers are cleaned between patients, most sonographers do not clean the cables or keyboards between patients. This was evident in the present study of students’ practice as well. Bacteria can exist on patients’ skin, and if a transducer or cable is not disinfected between each patient, bacteria can potentially be shared with other patients. This study also indicated that bacteria can be transmitted to the docking station where a transducer hangs between patient examinaitons. 9 This might explain how the linear array transducers, in the current study, became contaminated during the first exposure. Concurrent with the established literature, gel bottles were easily contaminated and a further source of vector transmission.16,18 Manufacturers also have reported incidents of contamination of coupling gel 3 as well as bacterial growth when gel bottles are refilled and warming units are used.6,16,18 There have been documented incidences of infection due to contaminated gel. 28
The students in this study were initially surprised by seeing the glow powder, and they expressed a desire to improve their cleaning and be more attentive to the equipment after it is used. Keeping a clean patient zone and sonography work environment can be challenging due to the volume of patients, design of equipment, multiple users, poor knowledge or practice of IPC, and a lack of sonography-specific disinfection guidelines.9,29 The AIUM issued a new official statement regarding cleaning and disinfection and noted that a review of recent literature pointed to a need for education in this area. 26 The updated AIUM official statement still does not address keyboards and work areas but does include gel bottles. The Compendium update, based on World Health Organization guidelines, indicated that one of the ways to prevent HAIs is to educate health care workers and enforce proper cleaning and disinfection of equipment and the environment. 19 The Joint Commission underscores this concept regarding disinfecting equipment. 8 This compounds the need for an effective means to improve student education in IPC practices. Visual inspection is insufficient to assess for contamination. 12 The students in this study benefited from the glow powder activity and assumed everything was contaminated and had to be cleaned accordingly after each patient. It was notable during observation 2 that the overall contamination rate was reduced, as students responded well to the experiential activity. It appeared to have had a positive effect on IPC practices.
Education About IPC
The Commission on Accreditation of Allied Health Education Programs (CAAHEP) accredits many sonography programs in the United States, providing standards and guidelines for a sonography curriculum. CAAHEP is not specific as to the requirements of teaching IPC, but under the topic of patient care, it states, “Maintain infection control and use standard precautions.” 30 It is also important to note that the National Education Curriculum for Sonography, endorsed by the Joint Review Committee on Education in Diagnostic Medical Sonography, indicates that standard precautions, personal protective equipment, and transducer disinfection should be addressed. Unfortunately, it did not provide more specific learning goals, objectives, or curricular materials for this important responsibility.
Sonography departments need to educate sonographers as to the specific use and applications of the variety of cleaning products that are recommended for their varied equipment. The CDC recommendations are general and neither ideal nor completely applicable to this type of environment and sensitive equipment. Transducers and ultrasound equipment cannot withstand an autoclave or be completely immersed in chemical baths without being damaged. Therefore, it is important to acquire products that can adequately disinfect without destroying this sensitive equipment. Students rotating through different hospitals can observe different habits, products, and techniques used for infection control and become familiar with varied ways to handle IPC.
There is no consistency in type of product used for cleansing and disinfection or standard approach to this challenge. General infection control guidelines for hospitals may be adapted for sonography departments, but there is a lack of specific guidelines for sonographers. 18 With regard to cleaning ultrasound equipment, information varies between ultrasound machine manufacturers as to the preferred products for cleaning. IPC and terminology have also changed over time. 31 This study would seem to indicate that guidelines should be established and disseminated. 12
Limitations
This study evaluated practices of students in a sonography scanning laboratory and therefore had a small sample size. Although hand hygiene is an important factor in IPC, this study was not designed to assess hand hygiene compliance. Individual student behavior was not evaluated in this study. In the future, it might be interesting to corroborate the study with a microbiological study using swabs and agar plates to test for real bacterial growth. This current study may have been strengthened if one more repeat observation had been performed.
Recommendations to Sonography Educators and Sonographers
Everyone performing sonography should be educated about the need for proper disinfection and IPC in the sonography examination room. Focus should be on the work environment as a whole, not just the ultrasound transducers. National organizations representing the sonography community should take the initiative to communicate the need to disinfect all clinical areas due to the potential for vector transmission. It is imperative that sonography department IPC guidelines be developed and disseminated.
Conclusion
Student sonographers require more education about the importance of cleaning the gel bottles, docking stations, cables, and patient care areas. Glow powder is an effective teaching technique that could be used to highlight deficiencies in infection control practices. It also helps students identify areas that require greater cleaning compliance in concert with IPC protocols. This study enabled students to increase their knowledge of transmission of infection and adherence to IPC practices. Student compliance increased significantly after exposure to glow powder training. The sonography community should address all aspects of the sonographic work environment to promote proper IPC.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.