
Abstract
A review of recent literature has demonstrated that ultrasound transducers may harbor bacteria and viruses that could cause cross-contamination for patients. Reducing the risk of cross-contamination is achieved by high-level disinfection of ultrasound transducers. One of the main types of high-level disinfectants (HLD) used in performing sonography is glutaraldehyde (GA). While GA-based HLDs are cleared in abundance by the FDA and compatible with most transducers, GA has been reported to cause extensive adverse effects and has limited efficacy as a disinfectant. This literature review provides a current set of studies that discuss high-level disinfection of ultrasound transducers, GA use, exposure, and alternatives. This information could be used by practitioners to carefully consider how to effectively clean ultrasound transducers and supporting equipment. Additional guidance is provided on how to potentially minimize GA exposure and suggestions for protecting patients during their imaging examination.
Infection control is becoming a vital issue in sonography practices. 1 Soiled ultrasound transducers pose the risk of cross-contamination as they are used from one patient to the next. 2 There has been a wave of recent data underscoring the risk of infection from ultrasound transducers, triggering the American Institute of Ultrasound in Medicine (AIUM) to release guidelines 3 on the importance of cleaning ultrasound transducers and highlighting the necessity for effective high-level disinfection (HLD).
According to the AIUM guidelines, 3 ultrasound transducers need to undergo high-level disinfection, which should include intracavitary transducers such as transesophageal, rectal, vaginal, and intraoperative transducers, as well as transducers that come in contact with bodily fluids, blood, or cracked skin. These intracavitary transducers are classified as semi-critical devices. In addition to high-level disinfection, transducer covers should be utilized for all transducers that may come in contact with blood or bodily fluids.
High-level disinfection (HLD) is defined as the destruction of all microorganisms except for bacterial spores. 3 The use of HLD is specific to equipment, such as transducers, that are sensitive to heat but can be exposed to liquids. 4 The AIUM does not endorse any specific HLDs as part of the guidelines. The guidelines do indicate that precautions should be taken to protect workers and patients from the toxicity of chemical disinfectants. 3 The AIUM guidelines provide a reference to the FDA website, since this is the agency that regulates HLDs. 3
There are 36 cleared HLDs on the FDA website as of 2018. 5 Of the 36 HLDs, 56% are glutaraldehyde (GA)-based (See Table 1). This review of the literature focuses on the use of GA, since such a high percent of FDA-approved HLDs are GA-based.
GA-based HLDs Cleared by FDA as of March 2015 a .
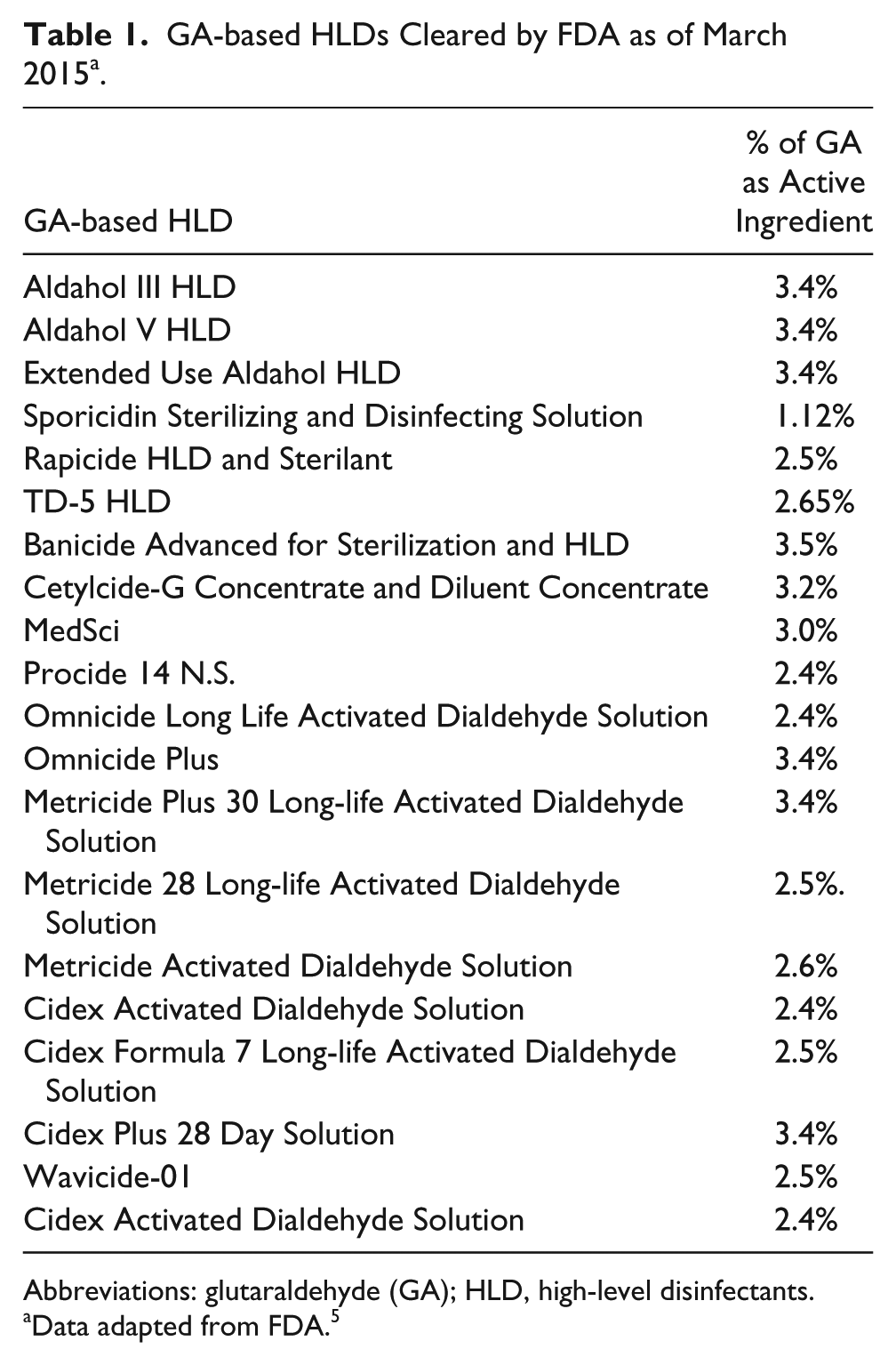
Abbreviations: glutaraldehyde (GA); HLD, high-level disinfectants.
Data adapted from FDA. 5
The breakdown of GA is as follows. The molecular formula for GA is C5H8O2 and the chemical abstract service (CAS) registry number is 111-30-8. 6 The permissible exposure limit for GA set by the National Institute of Occupational Safety and Health (NIOSH) is 0.2 parts per million (ppm), while the American Conference of Governmental Industrial Hygienists and the United Kingdom Health and Safety Executive have a threshold limit value of 0.05 ppm. 4
The compatibility of GA with ultrasound transducers is uniform. In accessing five ultrasound manufacturers’ current compatibility lists, Table 2 indicates the approximate percentage of GA-based HLDs approved for compatibility with varying transducers.
Percentage of GA-based HLDs Approved by Five Ultrasound Manufacturers.
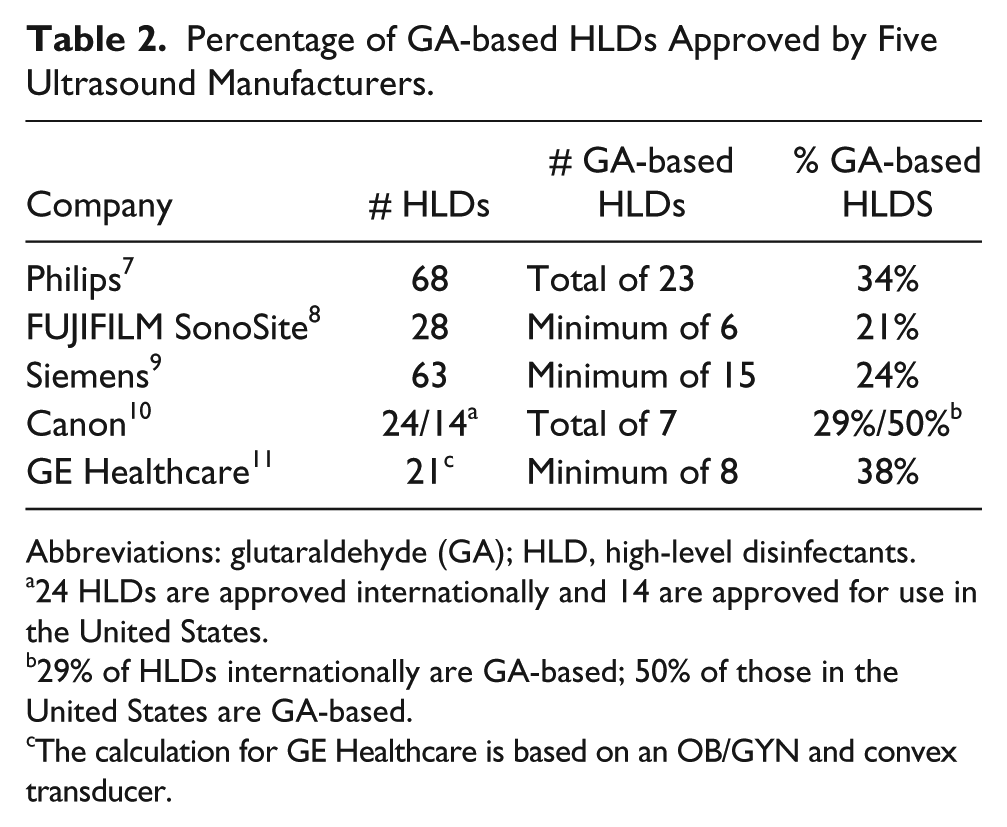
Abbreviations: glutaraldehyde (GA); HLD, high-level disinfectants.
24 HLDs are approved internationally and 14 are approved for use in the United States.
29% of HLDs internationally are GA-based; 50% of those in the United States are GA-based.
The calculation for GE Healthcare is based on an OB/GYN and convex transducer.
There is a valid concern that GA has been suspected of causing adverse effects, such as occupational exposure, and that it is perhaps ineffective against certain bacteria and viruses. 12 The concern is how and when GA-based disinfectants should be used in the sonography department.
Materials and Methods
This literature review was guided by the PICO method for evidence-based research, which also assisted in the development of the research question. 13 When using the PICO method, the letter “P” represents the population to be considered for research. In this literature review, the population is those occupational workers who practice sonography. “I” represents the intervention, which in this review indicates that the use of GA-based HLDs has been called into question. The “C” is the opposite of “I” and identifies the comparison group of occupational workers who are not using GA- based HLDs. “O” represents an outcome in which patients and occupational workers are protected from GA, and patients suffer no adverse effects from disinfected transducers. Therefore, the question that is used to drive this literature review is: Can the use of GA-based HLDs be eliminated from the practice of sonography while protecting occupational workers and their patients?
A literature review was performed by using key words and MeSH terms to obtain peer-reviewed research from PubMed, Medline, Google Scholar, and CINAHL. The final search was completed on July 23, 2018. The terms used to conduct the search included glutaraldehyde in the title or abstract, as well as the following terms: occupational exposure, glutaraldehyde and high-level disinfectant, glutaraldehyde, high-level disinfectant, and ultrasound, glutaraldehyde, high-level disinfectant, and sonography, glutaraldehyde, high-level disinfection and alternatives, high-level disinfection and ultrasound, high-level disinfection and sonography, ultrasound transducers and high-level disinfection.
The resulting articles were evaluated for eligibility using inclusion criteria. The inclusive criteria were based on articles released from 2005 to 2018, articles in English, and full articles, unless the abstract provided sufficient information. The articles were then evaluated for their relevance in addressing the use of GA and high-level disinfection in sonography.
The total search results returned 183 articles. The following articles were removed: 73 duplicates, 2 articles not in English, 14 articles with abstract only, 6 reviews of studies already included, and 58 were not specific to either GA use or high-level disinfection. A total of 30 articles were included in this final review of the literature. The articles were then split into three categories: high-level disinfection and ultrasound transducers, GA use and exposure, and GA alternatives. The GA alternatives section was then split into four categories: o-phthaladehyde (OPA), hydrogen peroxide, peracetic acid (PAA), and ultraviolet-C light (UV-C). The literature within categories was organized by publication year.
Review of the Literature
High-level Disinfection and Ultrasound Transducers
In 2016, Aryanti completed a meta-analysis regarding the contamination of transvaginal ultrasound transducers. 14 The results showed that high levels of bacteria remained on transducers even after appropriate disinfection and that new disinfection procedures are necessary. The possible benefit of using an automated system for disinfection was also noted.
Considering how important the issue of infection control in sonography has become, a recent survey was completed in the United Kingdom regarding disinfection practices. 15 The results of the survey found that disinfection practices for cleaning the ultrasound transducer and associated machine varied greatly among the 188 respondents. Training on disinfection products and procedures was also lacking. The study found that when buying ultrasound equipment, 56% of the sonographers in the study did not receive any training from the manufacturer on how to clean the transducer. When buying an HLD, 46% of the sonographers in the study did not get any training from the manufacturer on how to utilize the disinfectant. These results were concerning for both patient and sonographer safety.
Sartoretti et al. also found that training on disinfection procedures was very important for sonographers. 16 The results of the study showed that, prior to disinfection training, levels of bacterial contamination of ultrasound transducers was higher than bacteria counts on toilet seats and on poles on public buses.
The continued concerns regarding disinfection of ultrasound probes was addressed in a survey completed in the United States and released in 2018. 17 The results gleaned from 358 respondents indicated that a variety of high-level disinfection products are used with ultrasound transducers at this time and that 91% of respondents would prefer to have an automated disinfection system. The study also pointed out that a number of respondents did not have standard disinfection procedures at their institution, nor did they have proper training on disinfection protocols.
GA Use and Exposure
In 2006, Smith and Wang 18 reviewed the effects of GA exposure. The acute effects of GA exposure were skin irritation, eye irritation, contact dermatitis, and headache. The chronic effects were dermatitis, systemic sensitization, and occupational asthma. The study found the most important methods in minimizing exposure to GA were keeping the lids tight on GA containers, proper ventilation, and the use of personal protective equipment (PPE).
Takigawa and Endo 19 also reviewed the effects of GA exposure. The most prevalent toxic effects of GA use were irritation and sensitization of the skin, eyes, and respiratory tract. The effects also included asthma, headache, fatigue, and onset of multiple chemical sensitivity. Effects of GA exposure for patients caused fever, vomiting, tachypnea, tachycardia, and colitis. GA was studied among animals and it was found to be ten times more toxic to the nasal epithelium than formaldehyde. Increased nasal lesions and hyperplasia of respiratory epithelium were identified in the study animals, however carcinogenic or reproductive toxicities were not found. The study also underscored that chronic toxicity information was not available. The study identified that the best type of gloves for handling GA were butyl rubber or nitrile rubber gloves. It was also suggested that use of an automated disinfection machine would be beneficial in minimizing exposure.
Katagiri et al. studied GA levels among endoscopy workers in six Japanese hospitals. 20 The symptoms of the workers exposed to GA included nausea, pain/itching/and tearing of the eyes, nose irritation and odor disturbances, irritation/pain/and swelling of the pharynx, coughing, airway problems, and asthma. The study found that keeping lids on GA containers is essential to minimizing exposure. The use of PPE and ventilation was also important to minimize exposure. The study noted that the use of GA in Britain for endoscope disinfection was banned in 2002 and OPA was introduced as an alternative.
Collins et al. studied workers with GA exposure who might have had an increased risk of cancer. 21 The study found no associated cancers within the sinus, nose, nasopharynx, or leukemia. The source for this information was the death certificates of those patients who had indicated an exposure to GA.
In 2007, Nayebzadeh examined health care workers with GA expsoure. 22 Forty-two air samples were taken and 53 workers were interviewed. The reported symptoms from GA exposure were headache, burning/watery/and itchy eyes, itchy and runny nose, cough, and sneezing. The study reported that proper use of PPE when handling GA and a dedicated local ventilation system were helpful in reducing exposure. The highest cause of exposure to GA vapors occurred when a GA spill was being removed.
Martini et al. studied multiple chemical sensitivity (MCS) and associated occupational health effects. 23 The article noted that GA has been identified as a chemical of concern for healthcare workers with regard to MCS.
In 2013, Waters et al. completed a study on occupational asthma in health-care workers in the United Kingdom. 24 The study found that from 1991 to 2011 there were 182 cases of occupational asthma (OA) in the Midland Thoracic Society’s Surveillance Scheme of Occupational Asthma database. The highest number of cases of OA (N=69) were due to GA exposure.
In 2014, Meyers et al. found GA to be an ineffective disinfectant against human papillomavirus (HPV) 16. 25 This was the first study to show the inefficacy of GA against HPV.
Psaltikidis et al. reviewed the general use of GA alternatives. 26 The article focused on disinfection of endoscopes. The advantages of using GA were low cost, good compatibility and stability. The toxic effects of GA were irritation of eyes, throat, nose, and skin, as well as sensitization. The inefficacy of the GA noted in the article was related to an outbreak of over 2000 cases of post-operative infections in Brazil due to mycobacterium from probes cleaned in GA.
A guideline for HLDs for endoscopes also reviewed the advantages and disadvantages of GA use. 27 The advantages of using GA were the excellent biocidal activity and general effectiveness of the product, the low cost, its noncorrosiveness, the fact that it can be used in an automated or manual procedure, and that is not currently classified as a human carcinogen. The disadvantages were the adverse effects of skin irritation, dermatitis, eye/nose/throat and mouth irritation, epistaxis, asthma, and rhinitis. Residual GA on instruments can cause patients nausea, vomiting, abdominal cramps, diarrhea, and colitis. The pungent odor and the inefficacy against mycobacterium were also listed as disadvantages.
Ngu et al. completed the first study to investigate contamination of transvaginal transducer handles. 28 One group of transducers was disinfected in GA and the handle was left untreated. A second group of transducers was disinfected, including the handle, in an automated system. The results showed that 80.5% of the GA group transducer handles were contaminated, while 5.3% of the probes that were entirely disinfected were contaminated. The study suggests the importance of using disinfectant methods that include the transducer handles in order to minimize infection.
Copeland and Nugent studied respiratory effects after prolonged GA exposure. 29 The results found that GA can cause both irritant-induced or sensitization-induced asthma, along with irritation of the skin and airways, and an increased immune response. The symptoms of chest tightness and persistent cough were associated with GA-induced occupational asthma.
In 2015, GA was classified by The Association of Occupational and Environmental Clinics as an asthmagen. 30 Rosenman and Beckett noted that health effects from GA exposure can include irritation of eyes, nose and throat, contact, and allergic dermatitis. This is in addition to as many as 44 documented cases of GA-induced occupational asthma that have been identified in peer-reviewed journals.
With previous studies questioning the efficacy of GA, a hospital in Delhi that used GA conducted a study on the effectiveness of commercially available disinfectants before deciding whether or not to change disinfectants. 31 The results showed that 2.4% GA was the most successful high-level disinfectant.
The Japan Society for Occupational Health published new occupational exposure limits for GA in 2017. 32 The exposure limit must be kept below 0.03 ppm. GA was categorized as a substance that induces allergic reaction in humans in both the airway and skin.
GA Alternatives: O-phthaladehyde
Anderson et al. studied the use of topical applications of o-phthaladehyde (OPA) on mice. 33 The study found that OPA has the potential to be both an irritant and sensitizer, highlighting concerns of its use as a glutaraldehyde alternative.
A 2011 study conducted by Johnson et al. 34 was prompted due to numerous reports about OPA causing respiratory problems, skin sensitizations, anaphylaxis, and producing antibodies. The study focused on the potential for OPA to be a respiratory sensitizer. The results were that mice exposed to OPA vapor had increased lymphocytes and antibodies indicating that OPA has potential to be a respiratory sensitizer.
In 2014, Meyers et al. found OPA to be an ineffective disinfectant against HPV 16. 25 This was the first study to show the inefficacy of OPA against HPV.
Also, Psaltikidis et al. reviewed the use of OPA as a disinfectant. 26 In this study, OPA was found to be a good disinfectant as far as time and compatibility are concerned, but its potential for anaphylaxis and irritation made it a chemical of concern.
A guideline for high-level disinfectants for endoscopes also reviewed the advantages and disadvantages of OPA. 27 The advantages of using OPA were that the disinfection time is low, it has high efficacy, no activation is needed, it is not carcinogenic, and it can be used manually or in an automated system. The disadvantages were the irritant potential for eyes/skin/nose, aggravation of lung conditions, high cost, and the fact that it stains easily.
In 2016, Ryndock et al. examined the efficacy of OPA against HPV 16 and 18 on ultrasound transducers. 35 The results showed that OPA was not an effective disinfectant against the tested strains of HPV.
Likewise, Chatterjee et al. studied the effectiveness of OPA as a disinfectant. 31 The findings showed that OPA was effective but took longer than the specified time of soaking to achieve efficacy.
Additionally, Burgess et al. investigated the efficacy of OPA against GA-resistant mycobacterium. 36 The results found that OPA was not consistently successful at destroying the mycobacterium.
Lastly, Catlin et al. 37 studied the effects of OPA inhalation on mice. The study found that rats and mice exposed to OPA for 3 months developed numerous lesions throughout the respiratory tract and experienced problems with the nasal cavity.
GA Alternatives: Hydrogen Peroxide
Johnson et al. studied the use of an automated hydrogen peroxide-based system (AHPS) in a sonography department. 38 The findings showed that the sonographers in the study found that the automated aspect of the system eliminated some of the error that could occur from a manual system and that it increased the safety of the disinfection process. Overall, the sonographers found the AHPS to be efficient, easier, and safer to use than prior disinfectants. The downside to using the AHPS was the increased cost.
Similarly, Vickery et al. evaluated the efficacy of an AHPS with six different ultrasound transducer models. 39 The results showed that the simulated disinfection tests against 21 types of bacteria, viruses, and fungi were successful. The HLD standards were met with the system and like the prior study, there was satisfaction with the ease and safety of using an automated system for disinfection.
Additionally, a guideline for HLDs for endoscopes reviewed the advantages and disadvantages of hydrogen peroxide. 27 The advantages of hydrogen peroxide were good efficacy, no activation, no odor. The disadvantages were compatibility, and irritation to eyes/skin/GI-tract/nose/throat/lungs.
In 2016, Ryndock et al. examined the efficacy of an AHPS against HPV 16 and 18 on ultrasound transducers. 35 The results showed that the AHPS achieved efficacy against both forms of HPV.
Combs and Fishman created a proposal to reduce HPV transmission, via ultrasound transducers, in 2016. 40 The proposal concluded that an AHPS should be used in place of aldehyde disinfectants and that the transducer should be covered with a condom.
Importantly, Rutala et al. evaluated the efficacy of an AHPS with ultrasound transducers. 41 Ultrasound transducers were inoculated with one of four test organisms. The transducers were then disinfected with an AHPS. The findings showed that the system completely inactivated two of the test organisms (vancomycin-resistant Enterococcus and carpabenem-resistant Klebsiella pneumoniae) and did not completely inactivate the other two organisms (Mycobacterium terrae and Clostridium difficile).
Becker et al. evaluated an AHPS according to European and German test methods. 42 The results showed that the system was effective against human pathogenic enveloped and nonenveloped viruses and HPV.
Lastly, Burgess et al. investigated the efficacy of hydrogen peroxide against GA-resistant mycobacterium. 36 The results showed that hydrogen peroxide was successful at destroying the mycobacterium.
GA Alternatives: Peracetic Acid
In 2014, Meyers et al. tested the efficacy of peracetic acid (PAA) against HPV 16. 25 The findings showed PAA to be an effective disinfectant against HPV 16.
A study by Psaltikidis et al. reviewed the use of PAA as a disinfectant. 26 PAA was beneficial as far as disinfectant time and stability. The use of an automated system made it even more effective. The disadvantage of PAA was that it can be an irritant to both the eyes and the respiratory tract.
Additionally, a guideline for high-level disinfectants for endoscopes also reviewed the advantages and disadvantages of PAA. 27 The advantages of PAA were compatibility, quick disinfection time, good efficacy, and that fact that is environmentally friendly. The disadvantages were corrosion, higher cost, and the fact that contact with the chemical can cause eye and skin damage.
Chenjiao et al. evaluated the use of PAA for disinfecting endoscopes. 43 The results showed that after disinfection of a test endoscope from nine strains of microorganisms, the bacterial count was much lower with PAA than with alternatives. The PAA was also effective against certain antibiotic-resistant bacteria.
Finally, Burgess et al. investigated the efficacy of PAA against GA-resistant mycobacterium. 36 The results showed that PAA was successful at destroying the mycobacterium.
GA Alternatives: Ultraviolet-C light
One article from 2017 focused on the use of ultraviolet-C (UV-C) light as a disinfectant against HPV16 and HPV18, with intracavitary transducers. 44 The UV-C process used was an automated system with a 90-second cycle. The results showed that the UV-C was effective in destroying the viruses.
Discussion
GA Use
GA use has been associated with numerous health risks, both acute and chronic, for patients and health-care workers (see Figure 1).18–20,22–27,29,30,32 The new occupational exposure limit set in Japan, of less than 0.03 ppm for GA, is even lower than the limit of 0.05 ppm previously set in the United States and the UK. 32 Several studies have also demonstrated the inefficacy of GA against HPV and mycobacterium, both of which can be found on ultrasound transducers.25,36 Patient and sonographer safety are of the utmost concern in performing sonography. With the recent safety concerns, the literature shows there appears to be a downward trend in the use of GA. 17
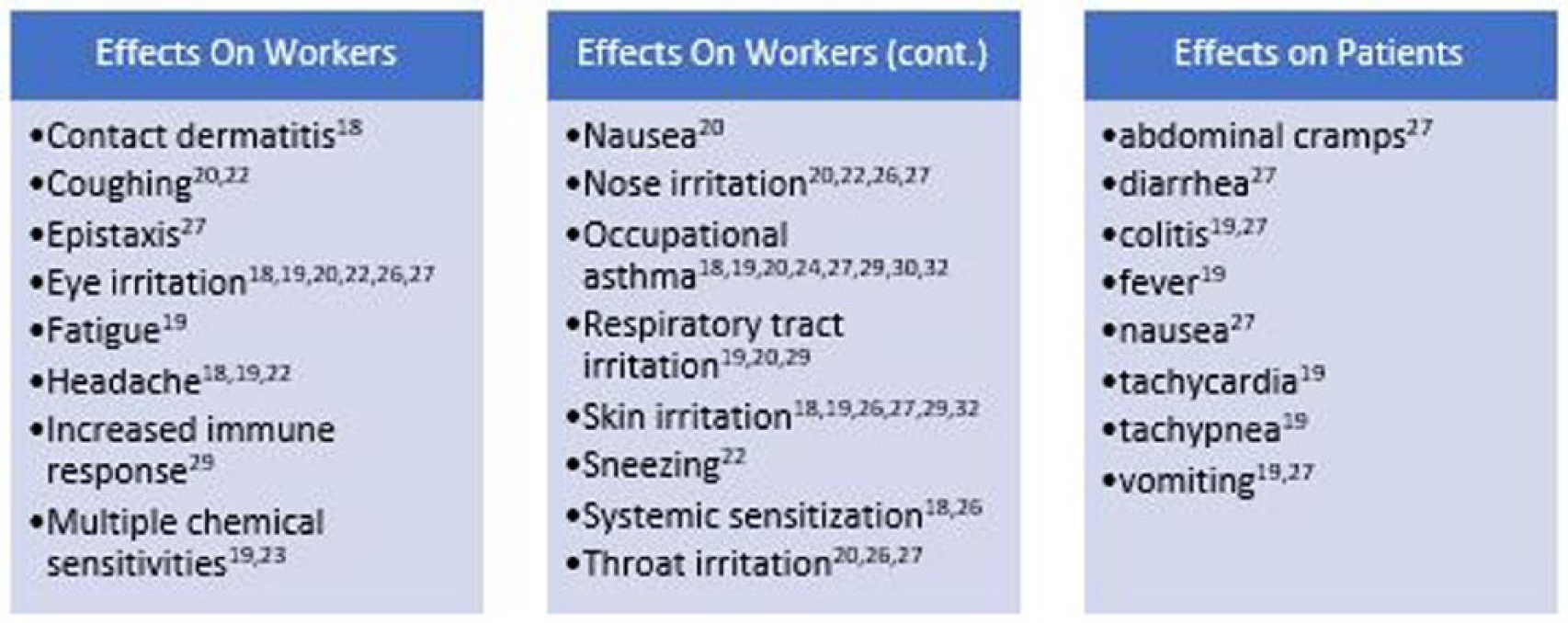
Effects of glutaraldehyde exposure on workers and patients documented in reviewed articles.
Best Practices With GA
If patients and sonographers continue to be exposed to GA, then there remains a need to continue examining the proper use of GA in sonography. This is especially important with the recent literature indicating that many sonographers are lacking training on the use of HLD chemicals and associated HLD procedures.15,17 As a reference for sonographers who currently work with GA, Figure 2 provides a list of some best practices, adapted from both the information in the reviewed articles and OSHA, for minimizing GA exposure in sonography.
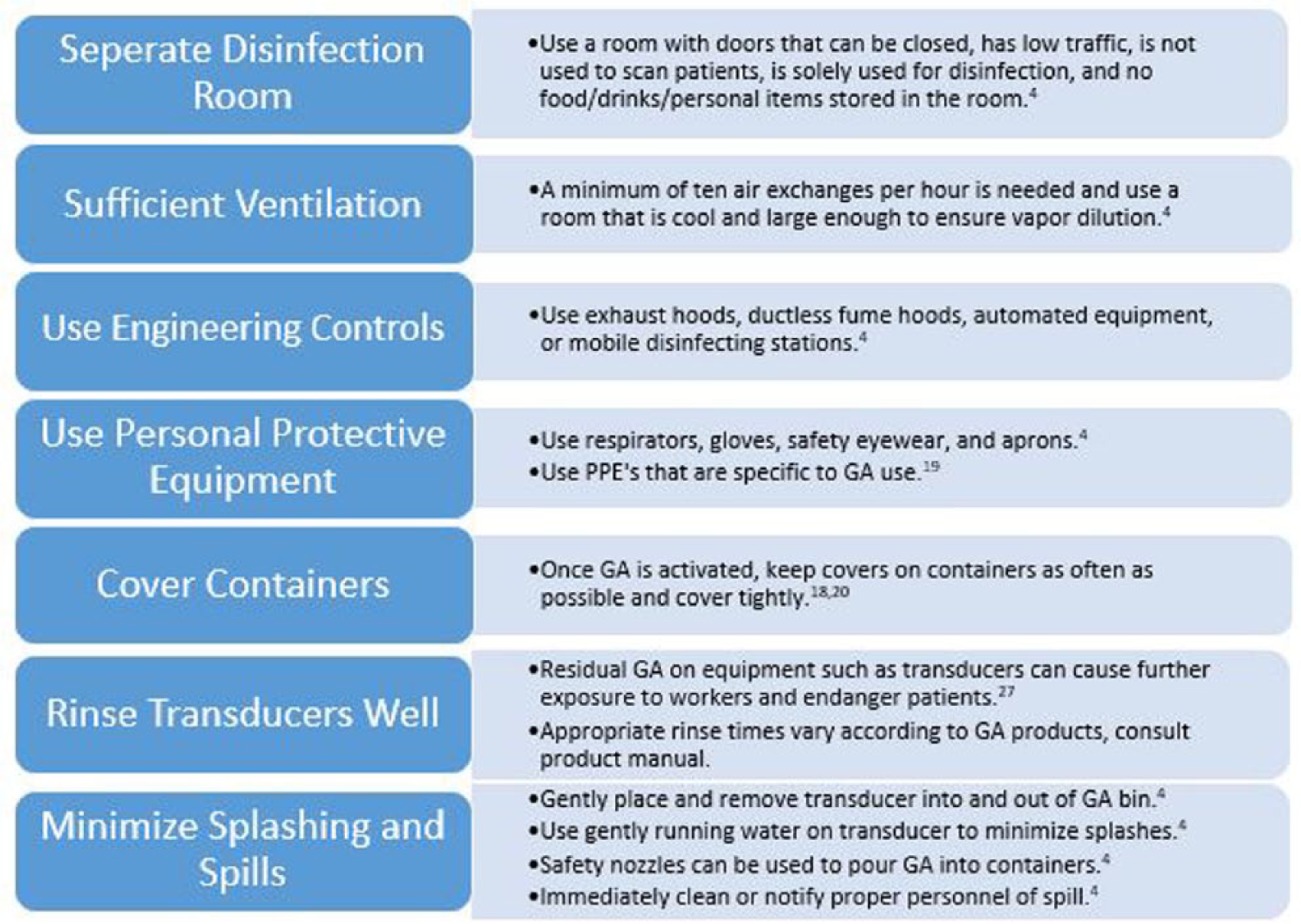
Best practices for minimizing glutaraldehyde exposure in sonography.
Alternative HLDs
The alternatives reviewed in the literature included OPA, hydrogen peroxide, PAA, and UV-C. Each of the alternatives has its own set of adverse effects (see Figure 3). In comparing the adverse effects of the four alternatives, OPA appears to have the widest range of adverse effects and has sensitizing potential. Both hydrogen peroxide and PAA were found to be irritants and to have the potential to cause tissue damage. The adverse effects of UV-C were not available. It is important to keep in mind that some of the alternatives are newer than others and have not been studied enough to determine their full potential toxicity.26,27
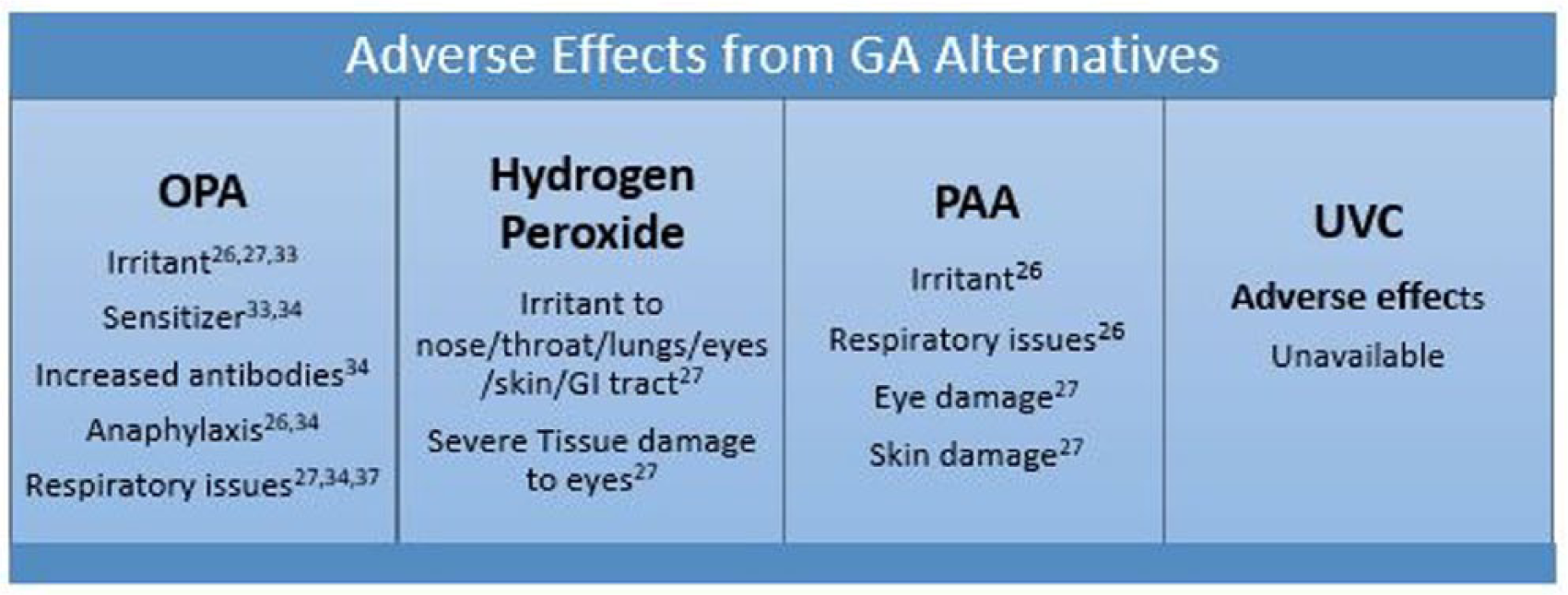
Adverse effects from glutaraldehyde alternatives.
The efficacy of the alternatives was not uniform. OPA was found to be at a disadvantage.25,35,36 OPA was not effective against HPV 16, HPV 18, and certain mycobacterium. Hydrogen peroxide had high efficacy and was found to be effective against HPV 16, HPV 18, and certain mycobacterium.27,35,36,39,41,42 PAA also had high efficacy and was found effective against HPV 16, antibiotic-resistant bacteria, and certain mycobacterium.25,27,36,43 There was no information available on the efficacy of PAA against HPV 18. UV-C was found to be effective against HPV 16 and HPV 18. 44 However, the efficacy of UVC was only supported by one study.
The four alternatives vary with respect to adverse effects and efficacy. These alternatives would need to be evaluated by each institution to determine the best available match. Multiple studies did suggest a possible benefit from using an automated disinfection system with the alternative HLDs.14,17,19,40 It appears that continued research into new alternative disinfection methods and toxicity remain very important.
Conclusion
The literature review and resulting information should be used to assist sonographers in limiting the use of GA-based HLDs as part of the practice of sonography. The aim is to provide high-quality disinfection and at the same time protect occupational workers and the patients. Best practices are important with the use of GA but do not eliminate the dangers of exposure to sonographers and patients. The literature indicates the need to minimize GA exposure and to consider possible alternative disinfectants to continue to provide high-quality disinfection. There are alternative disinfectants available and the goal should be to move towards a GA-free environment in sonography.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.