
Abstract
Diastolic function represents the filling property of the heart during diastole. Diastole comprises four phases: isovolumic relaxation, rapid filling, slow filling (diastasis), and active filling. Diastolic function is correlated to heart rate, atrial systolic function, ventricular compliance, preload, heart rhythm, and atrioventricular valve function. Diastolic dysfunction is a common condition; therefore, assessment of diastolic function should be a part of every routine echocardiogram. The latest recommendations for assessment of left ventricular diastolic function are practical and simple to implement in daily practice, and these recommendations are mainly based on six parameters: E wave, E/A ratio, septal or lateral e′, average E/e′, left atrial volume indexed, and peak tricuspid regurgitation velocity. The values of these parameters interact differently within many algorithms to diagnose and classify diastolic dysfunction. A summary is presented of the latest guidelines regarding assessment of diastolic function by echocardiography.
Diastolic function represents the filling property of the heart during diastole. Diastolic function applies to both the right and left ventricle (LV), but this review addresses mainly LV diastolic function given its clinical relevance. The LV is filled with blood initially by a pressure gradient between the left atrium (LA) and the LV (passive filling); the atrial contraction allows ventricular filling at end diastole (active filling). Diastolic dysfunction (DD) is understood as impaired LV relaxation, with increased LV stiffness at advanced stages and elevated filling pressures at more advanced DD stages. 1
DD is a prevalent condition; asymptomatic mild left ventricular diastolic dysfunction (LVDD) is estimated at 21% in the general population, whereas moderate or severe diastolic dysfunction is estimated at 7%. 2 Cardiac mechanics classically implies evaluation of systolic function, but diastolic dysfunction has proven to be an essential and integral component of cardiac mechanics, and the most striking demonstration is heart failure with preserved ejection fraction.3,4 In this regard, assessment of LV diastolic function should be a routine integral part of every echocardiographic evaluation, whether in healthy subjects or in patients with cardiac or extracardiac symptoms and conditions.
Despite the relative simplicity of the 2016 guidelines 4 (DD2016) for assessment of diastolic function, some authors still find complexities in diagnosing and grading LVDD according to the DD2016, and therefore they proposed a modified scheme that aims to simplify assessment of LVDD. 5
This short review presents a concise description of the physiology of diastolic function, a summary and short review of the latest guidelines regarding assessment of diastolic function by echocardiography, and a discussion regarding novelties in diagnosis and grading of diastolic dysfunction.
Method
The 2009 recommendations for assessment of diastolic function by echocardiography (DD2009) 1 and DD2016 were analyzed and data regarding diagnosis and grading of LVDD were specifically examined. Moreover, a Medline/PubMed search was performed to identify relevant articles using the following keywords: diastolic dysfunction, guidelines, and recommendations. Specifically, articles published after the DD2016 and addressing these recommendations were searched.
Background and Physiological Summary of Diastole
In July 2016, the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) released the new recommendations 4 for assessment of LV diastolic function by echocardiography. The previous recommendations dated from 2009 1 ; therefore, nearly seven years lapsed between the two most recent guidelines.
The LV exhibits ideal performance when generating efficient contraction followed by an optimal filling, and these two alternating functions of the LV are essential to generate an appropriate stroke volume. Classically, the four phases of diastole comprise isovolumic relaxation, rapid filling (represented by E mitral inflow wave), slow filling (diastasis), and active filling (represented by A mitral inflow wave) (Table 1).
Four Phases of Diastole.

The first phase consists of isovolumic relaxation, during which all four valves are closed.1,6 After isovolumic relaxation, the atrioventricular valves open due to higher intra-atrial pressure compared to that in the ventricles, and the second diastolic phase starts (passive filling), represented by the E wave. Of note, ventricles of young healthy individuals create a more powerful suction effect in the early phase of filling, and this is correlated to the more elastic expansion of the LV. 1 The third phase (diastasis) extends between the passive and the active filling of the LV, just before atrial contraction. During this period, filling decreases due to elevation in ventricular pressure, and therefore the flow from the atria into the ventricles is significantly reduced or even halted. The fourth phase is represented by active LV filling by atrial contraction and is manifested on spectral Doppler by the A wave.1,7
Grading of DD is classically as follows: grade I, impaired relaxation and decreased suction of the LV; grade II, pseudonormalization, increased stiffness of the LV, and possible elevated filling pressure; and grade III, restrictive filling with elevated filling pressure and noncompliant LV. This latter grade may be reversible with reduction of preload or irreversible with no benefit from reduction of preload. 1 Elevated filling pressures are the main pathophysiological consequence of advanced diastolic dysfunction. 8 Filling pressures represent the left atrial pressure (LAP) and the LV end-diastolic pressure, which are considered elevated when the mean pulmonary capillary wedge pressure is >12 mm Hg or when the LV end-diastolic pressure (left ventricular filling pressure [LVFP]) is >16 mm Hg (hemodynamic method). 9 However, LVFP and LAP are often used interchangeably to designate elevated filling pressure.8,9
Echocardiographic Approach and Useful Parameters for Diastolic Assessment
Many modes are implemented for assessment of LVDD—namely, bidimensional (BD) mode along with pulsed wave Doppler (PWD) and tissue Doppler imaging (TDI); moreover, many variables are considered in the comprehensive assessment of LVDD, and each of these variables may exhibit physiological variation. Also, no single variable can certainly evaluate diastolic function. In view of this and for the most successful evaluation of LVDD, it is mandatory for the echocardiographer to have a solid understanding of the physiologic rationale behind each variable along with the situations that make any given variable less or more reliable.4,6
The initial step in evaluating diastolic function consists of LA dimensions with the BD (left atrial volume indexed [LAVI]), followed by evaluating the mitral inflow patterns. LA dimensions are better measured using apical views; also, measuring indexed atrial volume is more accurate than linear dimensions measurements. Using PWD, the mitral inflow pattern is obtained with the peak of passive filling (E wave) and the peak of active filling (A wave) to calculate the E/A ratio. 10 Deceleration time of the E wave (DT) is also measured, together with the isovolumic relaxation time (IVRT). PWD also measures the tricuspid regurgitation peak velocity (TRpV), an essential parameter in the diagnosis of DD. 4
The presence and characteristics of the E and A waves vary considerably according to many physiological and pathological conditions. For example, the A wave disappears in atrial fibrillation. The characteristics of the E wave (duration, amplitude, and slope) depend on the physiological status and on the underlying heart condition; namely, the E wave amplitude decreases with age, and the E deceleration time increases with relaxation disturbances. 1 Moreover, the time delay between the E and A waves varies considerably according to atrioventricular delay. Of note, the E wave timing is dependent on the previous R wave timing, whereas the A wave is dependent on the previous P wave. In this regard, a long interval between P and R in an EKG will displace the previous R wave to the right and therefore yield an E wave closer to the A wave, and sometimes they merge together (Figure 1A,B).1,7
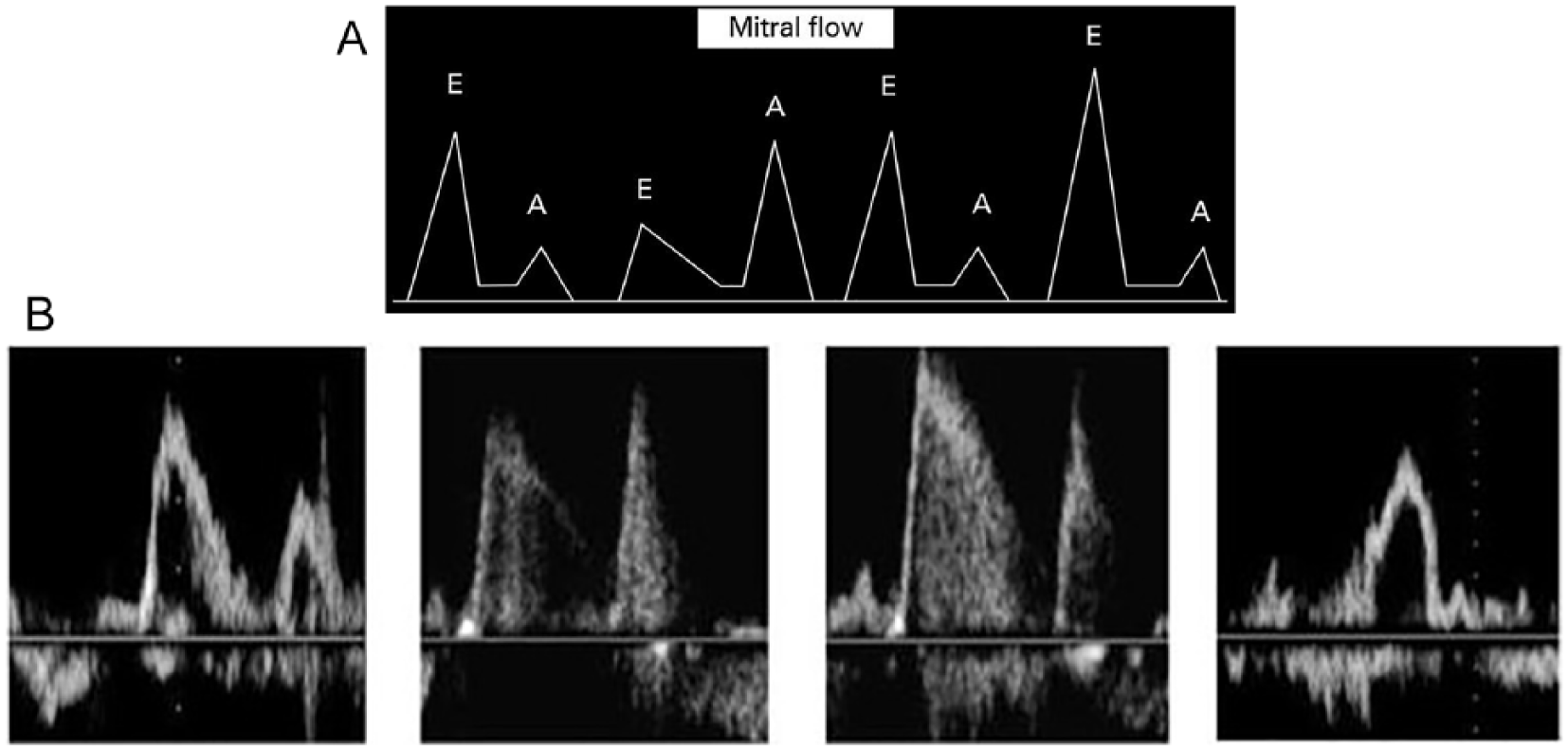
Drawn image (A) and actual image (B) showing the E and A Doppler waves and their variations according to diastolic dysfunction grades. This schema shows the different grades of DD (normal DF, grade 1 DD, grade 2 DD, and grade 3 DD from left to right) as initially suggested by Appleton et al. 10 DD, diastolic dysfunction; DF, diastolic function.
TDI is performed in the apical views to acquire mitral annular velocities; spectral recordings are better obtained at a sweep speed of 50 to 100 mm/s at end expiration, and measurements should reflect the average of three consecutive cardiac cycles at least. Moreover, minimal angulation (<20 degrees) should be sought between the ultrasound beam and the analyzed cardiac tissue axis. The early diastolic annular velocity is often expressed as (E′) and the late diastolic velocity as (A′) (Figure 2). In the presence of impaired LV relaxation and irrespective of LA pressure, the E′ velocity is reduced and delayed.1,11
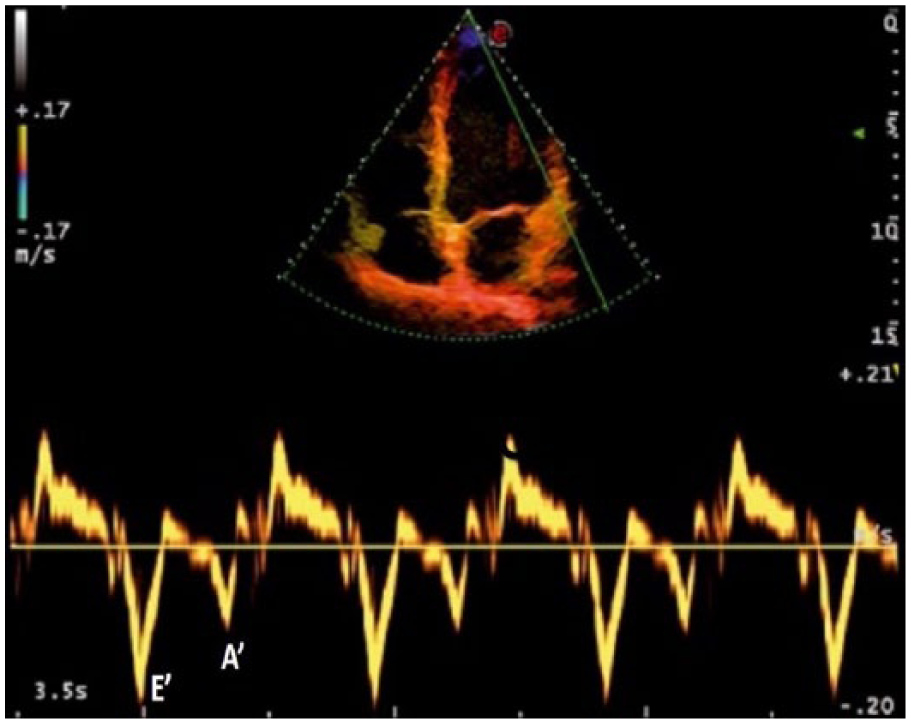
The tissue Doppler values recorded during early diastole (E′) and late diastole (A′) taken from the lateral mitral annulus.
Relevant variables for evaluation of LVDD
Many variables are used for the evaluation of LVDD, but not all variables have the same physiopathological values; also, each variable yields a different diagnostic and severity value, according to the algorithmic association provided by the latest recommendations. 4 Some cutoff values are presented as significant, but these cutoff values should not be used as isolated values to qualify or quantify LVDD. It is the algorithmic association that is meaningful in this regard as stated above:
Peak E velocity—cutoff value: >50 cm/s
Mitral E/A ratio
E/e′ ratio—cutoff value: average >14 (septal >15, lateral >13)
LAVI—cutoff value: >34 mL/m2
TRpV—cutoff value: >2.8 m/s
Septal e′—cutoff value <7 cm/s or lateral e′—cutoff value <10 cm/s
The above parameters are the essential parameters implemented in the DD2016, 4 but many other maneuvers or parameters may be useful, either as additional parameters or in specific clinical scenarios:
IVRT 12 : time delay between aortic valve closure and mitral valve opening (Figure 3A,B)
E wave DT 12
Pulmonary venous systolic/diastolic (S/D) ratio 13 : a normal pulmonary venous flow usually shows a tri- or quadriphasic pattern consisting of a pulmonary venous first systolic wave (S1), second systolic wave (S2) (S wave velocity is made by adding S1 and S2), pulmonary venous early diastolic wave (D), and pulmonary venous atrial reversed flow wave (Ar) (Figure 4)
Ar-A duration: the time difference between Ar duration and mitral A duration
Color M-mode flow propagation velocity (Vp): a normal Vp is >55 cm/s 14 (Figure 5)
L wave (abnormal wave during diastasis) 15 : representing an ongoing LV filling in mid-diastole
Valsalva maneuver and ΔE/A 16 : a decrease of E/A ratio of ≥50% is highly specific for increased LV filling pressures
IVRT/TE-e′: ratio of IVRT to time difference between E wave onset and e′ onset 4
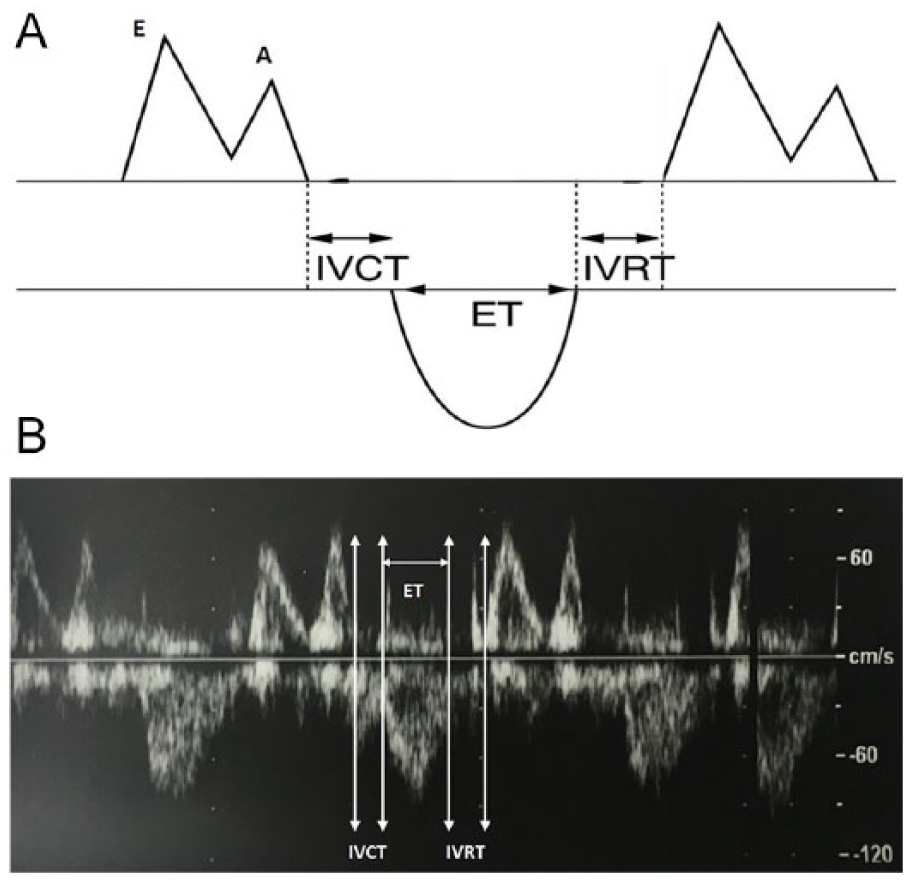
Drawn image (A) and actual image (B) showing the isovolumic contraction time (IVCT), ejection time (ET), and isovolumic relaxation time (IVRT).
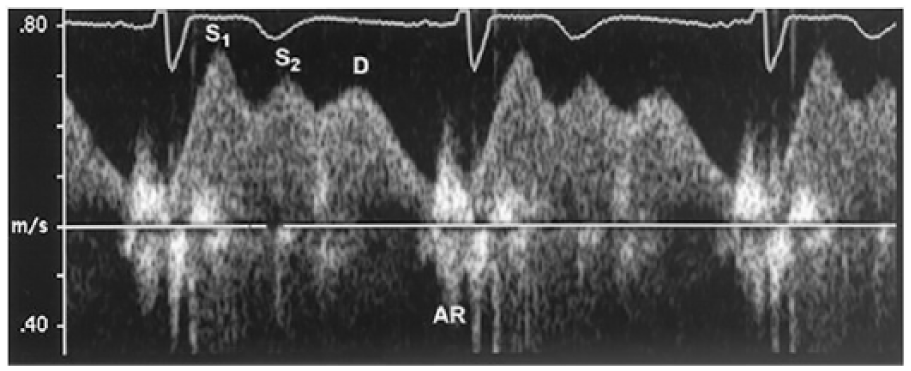
Pulmonary venous flow. AR, atrial reversed flow; D, diastolic wave; S1, S2, systolic waves.
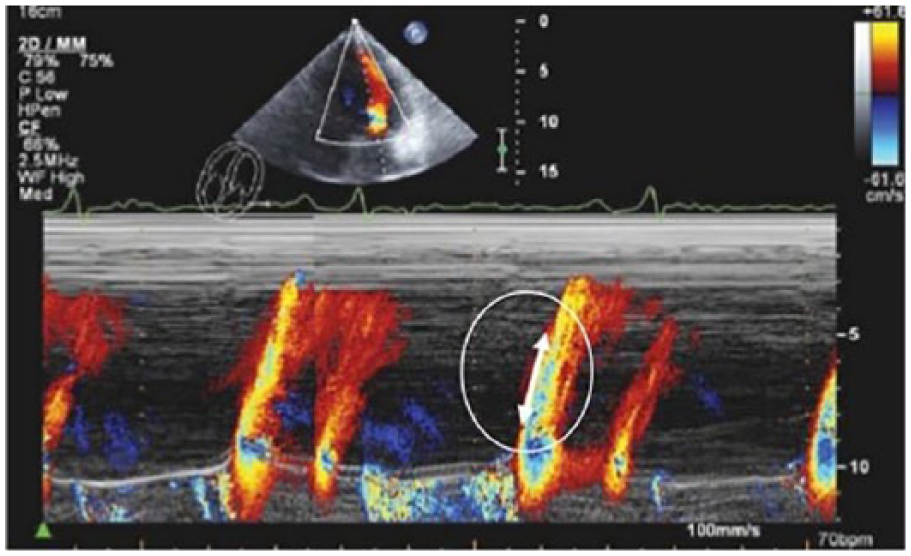
Transmitral color Doppler M-mode flow propagation velocity (Vp). Vp is measured as the slope of the first aliasing velocity during early filling (E wave); a normal Vp is >55 cm/s.
Summary of the 2009 Recommendations for Evaluation of LV Diastolic Function by Echocardiography
Evaluation of LVDD according to the DD2009 was essentially based on the mitral inflow pattern and TDI measurement of the mitral annular velocity (e′). 1 Accordingly, diagnosis and grading of LVDD was performed, and diastolic function was classified as following: normal, impaired LV relaxation (mild DD, grade 1), pseudo-normal (moderate DD, grade 2), or restrictive pattern (severe DD, grade 3).1,10,11
According to DD2009, 1 a septal e′ >8 and lateral e′ >10 (or average e′ ≥ 9 cm/s) and LA dimensions <34 cc/m2 imply a normal diastolic function (Table 2). Of note, reduced mitral E/A ratio in the presence of normal annular tissue Doppler velocities can be seen in volume-depleted normal subjects, so an E/A ratio <0.8 should not be universally used to infer the presence of DD. 1
Diagnosis of Diastolic Dysfunction According to DD2009.
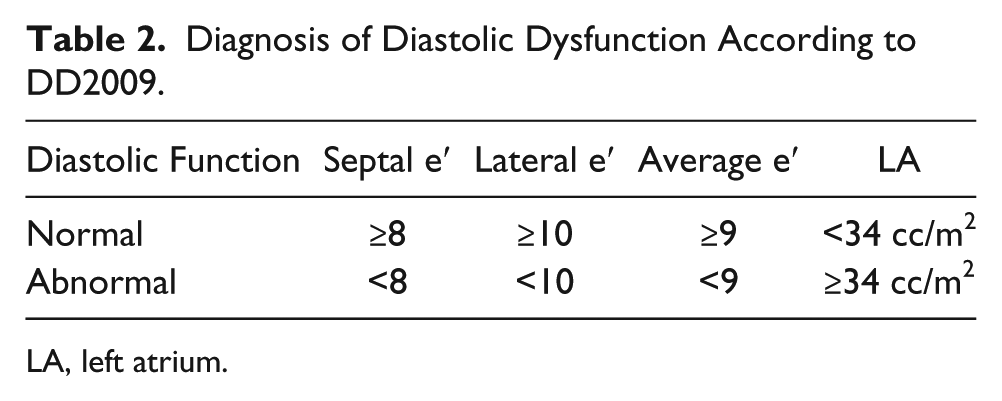
LA, left atrium.
DD grade I represents impaired myocardial relaxation with normal LV filling pressures: average E/e′ ratio is <9, E/A ratio is <0.8 cm/s, DT is >200 ms, and IVRT is ≥100 ms with predominant systolic pulmonary venous flow (S > D). 1
Grade II DD represents impaired myocardial relaxation with mild to moderate elevation of LV filling pressures: E/A ratio is ≥0.8 and may go up to 2 (pseudo-normal); also, the ratio decreases more than 50% during the Valsalva maneuver, and the average E/e′ is from 9 to 12. Other supporting data include an Ar velocity >30 cm/s and an S/D ratio <1. 1
With severe diastolic dysfunction (grade III), restrictive LV filling occurs: E/A ≥2, DT <160 ms, IVRT >60 ms, mitral A flow duration shorter than Ar duration, and average E/e′ ratio >13 (or septal E/e′ >15 and lateral E/e′ >12). LV filling may improve partially with successful therapy in reversible cases (grade IIIa), whereas LV filling pressure remains high in an advanced irreversible restrictive pattern (grade IIIb) (Table 3). 1
Grading of Diastolic Dysfunction According to DD2009.
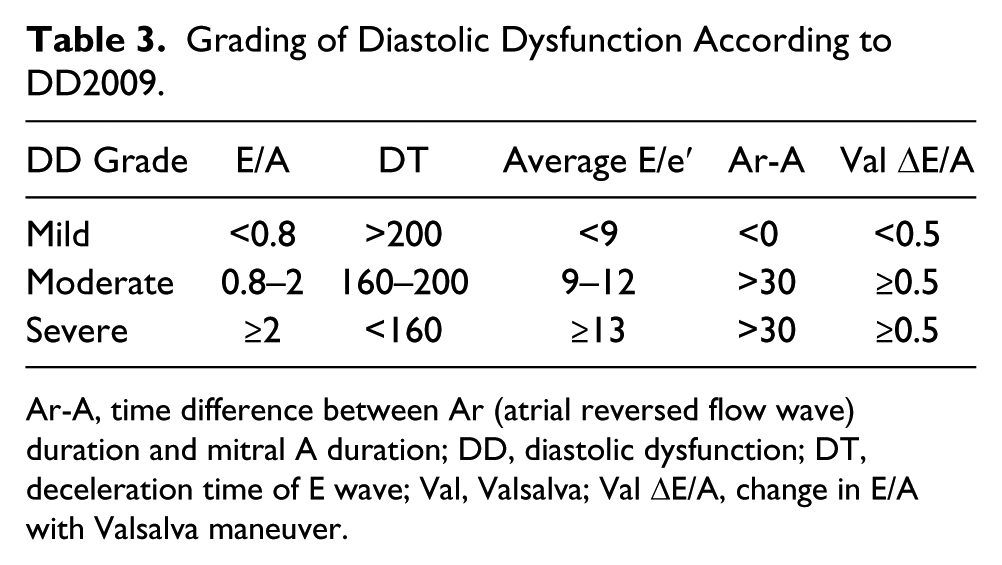
Ar-A, time difference between Ar (atrial reversed flow wave) duration and mitral A duration; DD, diastolic dysfunction; DT, deceleration time of E wave; Val, Valsalva; Val ΔE/A, change in E/A with Valsalva maneuver.
Evaluation of LVFP depends on multiple criteria and algorithms according to whether ejection fraction is normal or not. Table 4 (normal ejection fraction) and Table 5 (abnormal ejection fraction) illustrate these scenarios. Ejection fraction was considered normal in the DD2009 when value was ≥50%.
Evaluation of LV Filling Pressure in Patients With Normal Ejection Fraction According to DD2009.
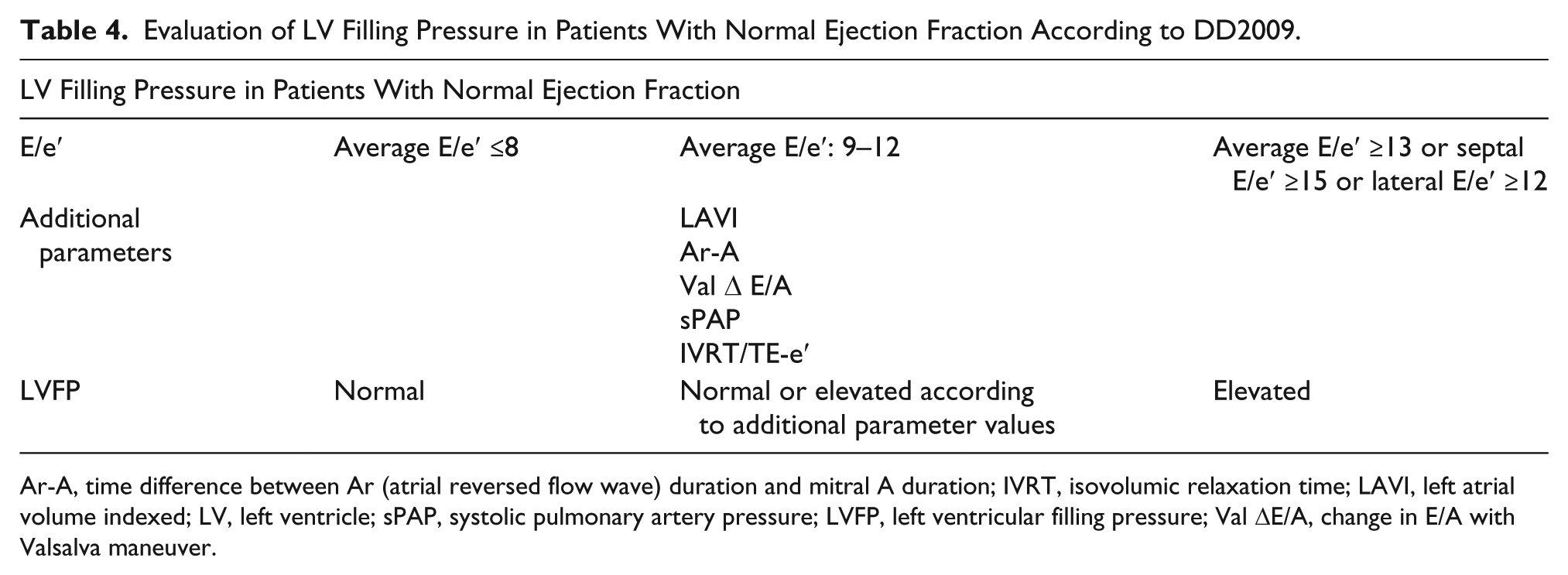
Ar-A, time difference between Ar (atrial reversed flow wave) duration and mitral A duration; IVRT, isovolumic relaxation time; LAVI, left atrial volume indexed; LV, left ventricle; sPAP, systolic pulmonary artery pressure; LVFP, left ventricular filling pressure; Val ΔE/A, change in E/A with Valsalva maneuver.
Evaluation of LV Filling Pressure in Patients With Depressed Ejection Fraction According to DD2009.
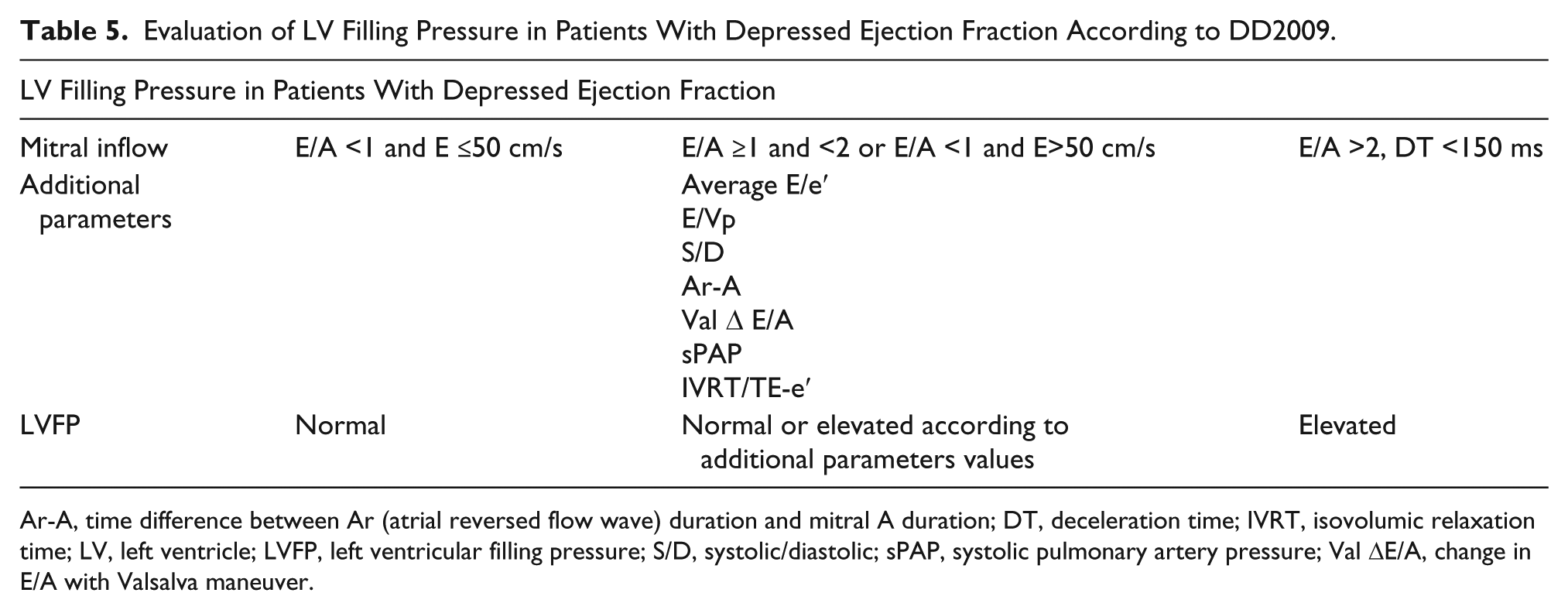
Ar-A, time difference between Ar (atrial reversed flow wave) duration and mitral A duration; DT, deceleration time; IVRT, isovolumic relaxation time; LV, left ventricle; LVFP, left ventricular filling pressure; S/D, systolic/diastolic; sPAP, systolic pulmonary artery pressure; Val ΔE/A, change in E/A with Valsalva maneuver.
Summary of the 2016 Recommendations for Evaluation of LV Diastolic Function by Echocardiography
According to the current guidelines (DD2016) and for patients with preserved ejection fraction, one should evaluate four variables to assess diastolic dysfunction: e′, E/e′ ratio, LAVI, and TRpV. If three of the parameters are abnormal, there is DD; if two are abnormal and two normal, diastolic function cannot be assessed; and if three are normal, diastolic function is normal. The four criteria used to diagnose LVDD and their cutoff values are as follows: septal e′ <7 cm/s or lateral e′ <10 cm/s; average E/e′ >14, LAVI >34 cc/m2, and TRpV >2.8 m/s. 4
Figure 6 illustrates the algorithm for the diagnosis of LVDD in patients with normal LV ejection fraction, and Figure 7 illustrates the algorithm for diagnosis and grading LVDD in patients with reduced LV ejection fraction or in patients with preserved ejection fraction and with myocardial diseases.
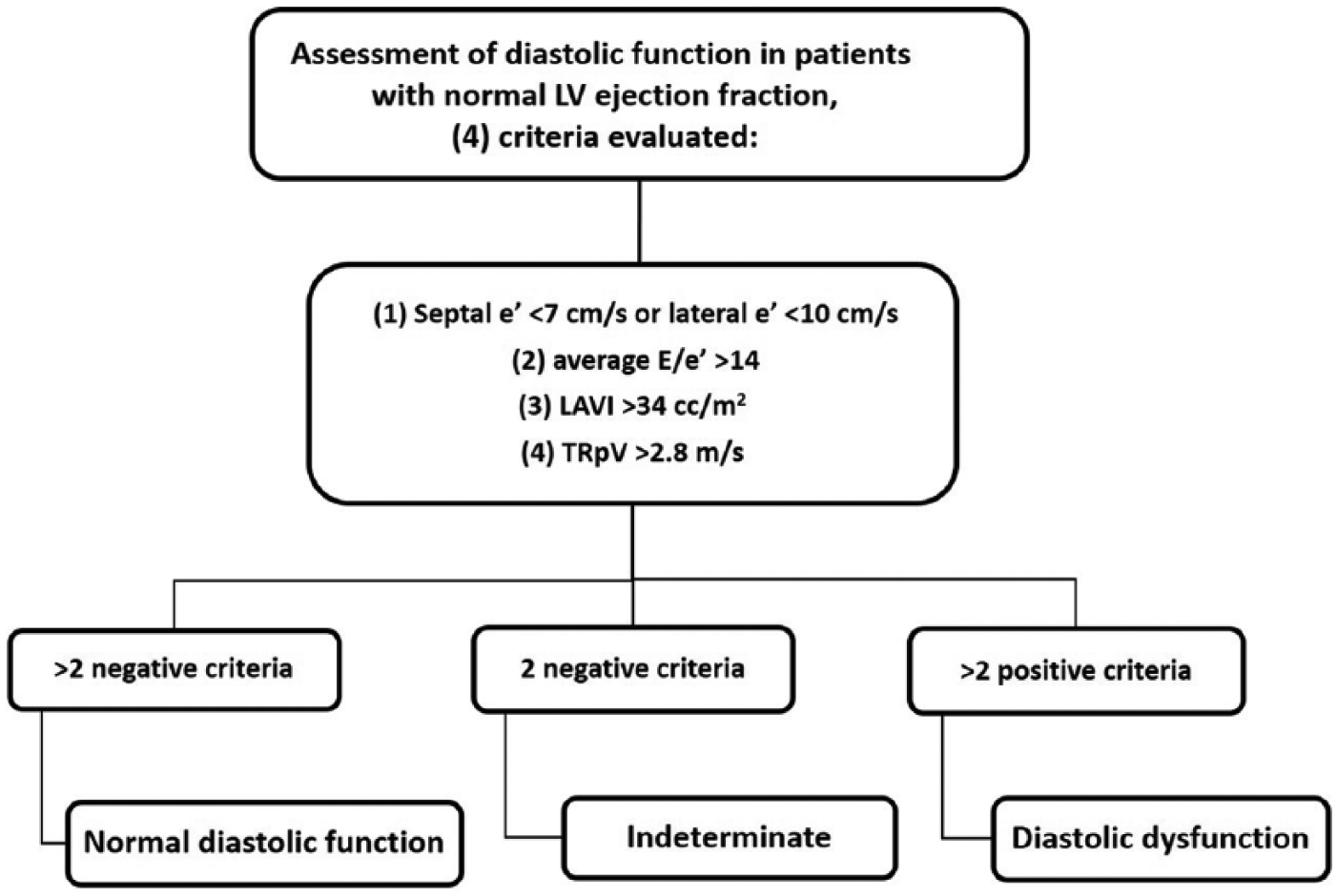
Algorithm showing diagnostic criteria of left ventricular diastolic dysfunction (LVDD) in patients with normal left ventricle (LV) ejection fraction. 4
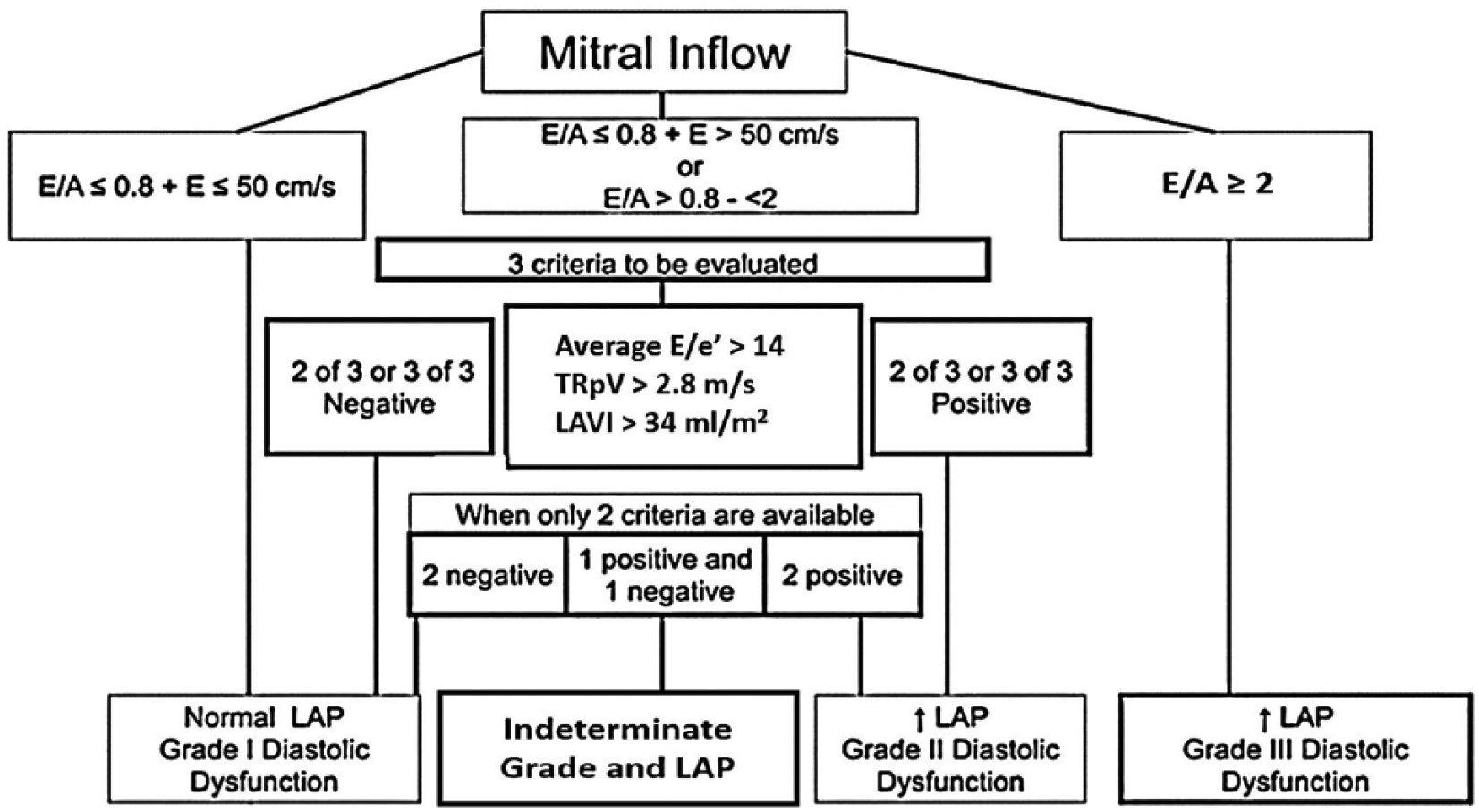
Algorithm showing grading of left ventricular diastolic dysfunction (LVDD) in patients with reduced left ventricle (LV) ejection fraction and in patients with preserved ejection fraction and with myocardial diseases. 4
In patients with reduced LV ejection fraction, E/A ratio ≤0.8, and a peak E velocity ≤50 cm/s, there is normal LAP, representing grade I of DD. If E/A ratio is >2, this represents elevated filling pressures and LVDD is classified as grade III. When E/A is >8 and <2 or when E/A ≤8 with E velocity >50 cm/s, additional parameters (average E/e′, TRpV, and LAVI) are required to evaluate grading and filling pressures: if two or three of these are positive, diastolic dysfunction is grade II and filling pressures are elevated; if two or three are negative, filling pressure is normal and DD is grade I; if one is positive and one negative (one indeterminate), pulmonary vein S/D should be used; and if S/D <1, LVDD is grade II and LVFP is elevated. 4
Discussion
In patients with normal LV ejection fraction and with myocardial disease or in patients with low ejection fraction, LVDD is likely to be present (Figure 7), and the different parameters and their algorithmic relationship allow grading of LVDD and LVFP. Pratap et al. 17 reported that isolated diastolic dysfunction is rare, and it is almost always associated with systolic dysfunction when evaluated by strain imaging.
Sanchis et al. 18 performed an evaluation of LV diastolic function using initially the DD2009, and then patients were reevaluated using the DD2016. The authors concluded that the DD2016 resulted in a more accurate classification of patients, according to their brain natriuretic peptide (BNP) levels, heart failure diagnosis, and cardiovascular outcomes; in addition, most patients previously diagnosed with DD grade 1 using the DD2009 were reclassified as having normal LV diastolic function with the DD2016. This observation confirmed findings from other authors who reported a significant decrease in DD prevalence when using the DD2016 compared to the DD2009. 19 Similarly, Almeida et al. 20 reported a poor concordance between the DD2016 and the DD2009 with consequently a much lower prevalence of LVDD when using the DD2016.
Conversely, Clancy et al. 21 reported that DD2016 identified a significantly higher incidence of DD in patients with severe sepsis and septic shock compared to the DD2009; moreover, the authors found that DD2016 yielded less indeterminate diagnosis of DD.
Interestingly, Prasad et al. 22 reported that in patients with acute myocardial infarction, advanced stage DD (grade 2 or 3) as assessed by DD2016 is a robust independent predictor of clinical outcomes (death, myocardial infarction, and heart failure), whereas advanced DD (grade 2 or 3) using the DD2009 algorithm was not a significant predictor of major clinical outcomes. Sanfilippo et al. 23 reported that the DD2016 allows for a practical approach in evaluating patients in intensive care or during operative procedures when a rapid and simplified assessment of diastolic function is required. Sato et al. 24 reported that significant DD (grade 2 or 3) as assessed by the DD2016 was associated with a higher risk of mortality and that the grading algorithm proposed by the DD2016 detects elevated LVFP and correlates with clinical outcome better than the DD2009.
Novelties in the DD2016
The latest recommendations for assessment of LV diastolic function are practical and simple to implement in daily practice. Diagnosis and grading of LVDD are mainly based on the value of six parameters: E wave, E/A ratio, septal or lateral e′, average E/e′, LAVI, and TRpV. The values of these parameters interact differently within many algorithms to diagnose and classify LVDD.
E/A ratio is not implemented for patients with normal ejection fraction and with no myocardial disease. Moreover, the TRpV is a newly used parameter for diagnosis and grading of LVDD, as it was not used in the DD2009. 1 The different grades (I, II, III) of DD did not change, although the various criteria for grading changed. Indices and maneuvers that are not used regularly anymore as per the DD2016 include the Valsalva maneuver, IVRT, DT, Ar-A, and the following ratios: E/Vp, IVRT/TE-e′, and S/D. 4
Limitations and Specific Situations
Evaluation of echocardiographic indices of LVDD should be performed while putting them into the general clinical context, mainly the patient age, symptoms, heart rate, rhythm, and loading conditions. In this regard, the DD2016 states that the guidelines do not necessarily apply to children and in perioperative settings where loading conditions may be different compared to baseline status.
Selmeryd et al. 25 reported a substantial interstudy heterogeneity regarding definitions of DD, and they conclude that such heterogeneity severely affects the reported prevalence; for example, some studies present LVDD definition without citing the grade of DD, whereas other studies presented LVDD definition based solely on early diastolic tissue velocity and/or left atrial size. The resulting prevalence of LVDD varied from 12% to 84%, depending on the LVDD definition used.
Suboptimal Doppler signals can lead to misinterpretation; moreover, the variables of the E/e′ ratio are measured at different times in the cardiac cycle, with this ratio being age and preload dependent. When significant heart rate variability is present, a mean of three measurements should be taken for parameters affected by loading conditions (E/A mainly). Moreover, E/A ratio cannot be measured reliably in the presence of atrial fibrillation, significant mitral annular calcification, significant mitral regurgitation or stenosis, prosthetic mitral valve, bundle branch block, and paced rhythm. However, E/e′ is still a valid measurement in patients with atrial fibrillation. 12
A specific approach is recommended for evaluation of LVDD in certain clinical scenarios: hypertrophic cardiomyopathy, restrictive cardiomyopathy, valvular heart disease, atrial fibrillation, heart transplantation, atrioventricular block, and in patients with a pacemaker. 4 In addition, in athletic healthy individuals, a very tall E wave with normal DT along with a small A wave may lead to an E/A ratio >2, simulating a restrictive filling pattern; this is due to supernormal filling owing to a strong suction of the LV during early diastole in a healthy heart. Therefore, it should not be mistaken for a restrictive pattern. 12
Patients with LVDD usually have reduced diastolic reserve, which can be uncovered by stress testing.1,4 Diastolic stress testing is indicated when a resting echocardiogram does not explain the symptoms, especially dyspnea on exertion; it is considered positive if three conditions are met: average E/e′ >14 or septal E/e′ ratio >15 with exercise, TRpV >2.8 m/s with exercise, and septal e′ velocity of <7 cm/s at baseline (if only lateral velocity is acquired, lateral e′ <10 cm/s at baseline).
Conclusion
Echocardiography should be used on a routine basis to evaluate diastolic function, namely in patients showing signs or symptoms evoking LVDD, such as dyspnea. Possible causes of diastolic dysfunction are variable, such as primary myocardial heart diseases (LV hypertrophy, constrictive cardiomyopathies, myocardial fibrosis) or other cardiac conditions leading to myocardial dysfunction (ischemia, valvular heart diseases, etc.). Moreover, diastole is affected by numerous factors such as heart rate, ventricular compliance, preload, atrial systolic function, heart rhythm, and atrioventricular valve function.
Diagnosis of LVDD remains challenging, and many studies have shown heterogeneity in the echocardiographic approach to evaluate LV diastolic function. According to the DD2016, evaluation of LVDD is mainly based on six indices: E wave, E/A ratio, septal or lateral e′, average E/e′, LAVI, and TRpV. The different grades of LVDD as stated by the latest recommendations are similar to the previous classification (grade I, grade II, grade III); however, the criteria and their algorithmic association for grading have changed, namely for evaluation of LVFP, making diagnosis and grading of LVDD more practical and simple to implement in daily practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.