
Abstract
Juvenile fibroadenomas of the breast are benign neoplasms. They present during the development phase of the breast. They are poorly understood because of their rarity and unpredictable behavior. In this article, a series of three different sonographic breast cases are provided of adolescent girls, who were brought for medical evaluation of a large breast lump, which had presented just after menarche. The results of evaluating these cases revealed that sonography of the breast was helpful in characterizing and delineating the extent of the lump. In conclusion, giant fibroadenomas of the breast, at menarche, are also known as juvenile fibroadenomas. They are a dilemma for the clinician, radiologist, and pathologist alike. The use of ultrasound can assist with characterizing these lesions, as an incorrect diagnosis could lead to a disfiguring surgery, for a young girl.
Juvenile fibroadenomas presenting in a young girl at menarche pose a challenge not only for the clinician but also for the interpreting radiologist and the pathologist. The behavior of this neoplasm is unpredictable clinically and radiologically.1,2 Their rapid growth, stretching of overlying skin, prominent overlying veins, and sometimes ulceration give a clinical suspicion of malignancy. In addition, their radiologic findings do not correspond to that of a benign mass lesion. Even their histopathological features can vary from case to case. A misinterpretation may lead to a radical surgery, for this nonthreatening condition. A series of three cases are provided with this same breast pathology.
Case 1
A 12-year-old female presented with the primary complaint of a sudden increase in size of her left breast over a period of three months. On clinical examination, the left breast was grossly enlarged and hard, and the mass occupied most of the breast. The lesion measured 12.2 × 10.6 cm. Due to size of the mass, the skin was stretched over it. The overlying veins were also very prominent. In contrast, the right breast demonstrated normal pubertal growth and was soft with no palpable lump. The mother explained that the daughter had started menstruating just three months prior, and since then, the left breast had grown to the present size. The patient did not complain of any severe pain but was uncomfortable and was tender to the touch.
Sonography evaluation of this mass was performed and revealed a large space-occupying heterogeneous lesion with intervening cystic spaces (Figure 1). The mass was so large that it could not be viewed in a single sonographic frame. There were also echogenic foci seen in the lesion that exhibited posterior shadowing. The mass caused paucity of normal breast tissue. The sonographic pattern of this lesion was confusing and not consistent with that of any of the benign lesions of the breast. Sonography of the right breast was normal.
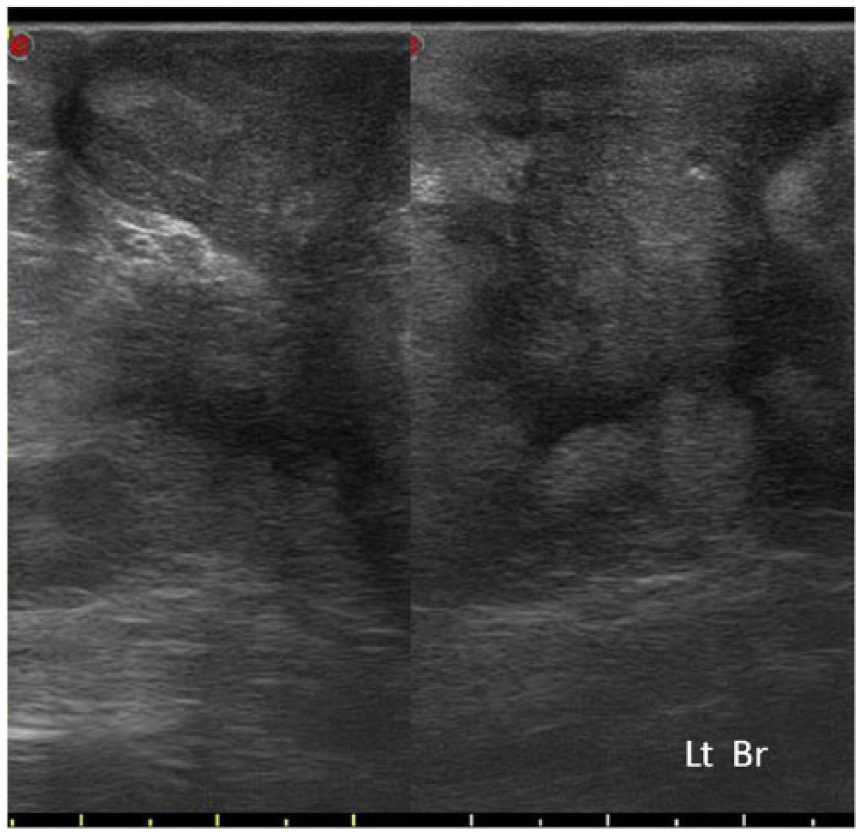
Sonogram of the left breast shows a large space-occupying heterogeneous lesion with intervening cystic spaces. The mass could not be entirely seen on one digital frame.
Seeing the increased anxiety of the parents, the patient was scheduled for surgery the next day and the excision of the neoplasm carried out. Histopathology of the excised tissue showed a juvenile fibroadenoma. There was no recurrence noted clinically or sonographically in the follow-up at six months.
Case 2
A 17-year-old female presented with swelling of the right breast. The patient had a history of delayed menarche with cycles being irregular and scanty. The increase in size of the right breast was initially taken as pubertal growth, but when the right breast was almost double the size of the left, the patient was referred for clinical assessment. On palpation, a large diffuse mass 10.6 × 7.1 cm was found to occupy both the medial quadrants of the right breast and was firm, nontender, and freely mobile. The lesion was not fixed to overlying skin or underlying muscles. The left breast was normal on palpation.
The sonogram demonstrated a diffuse heterogeneous mass of irregular shape, with ill-defined margins (Figure 2). The zone of transition between the normal breast tissue and the mass could not be demarcated. The left breast was determined as normal on the sonogram. The right mass was biopsied by fine-needle aspiration (FNA) and was diagnosed as a juvenile fibroadenoma, which was also histopathologically confirmed.
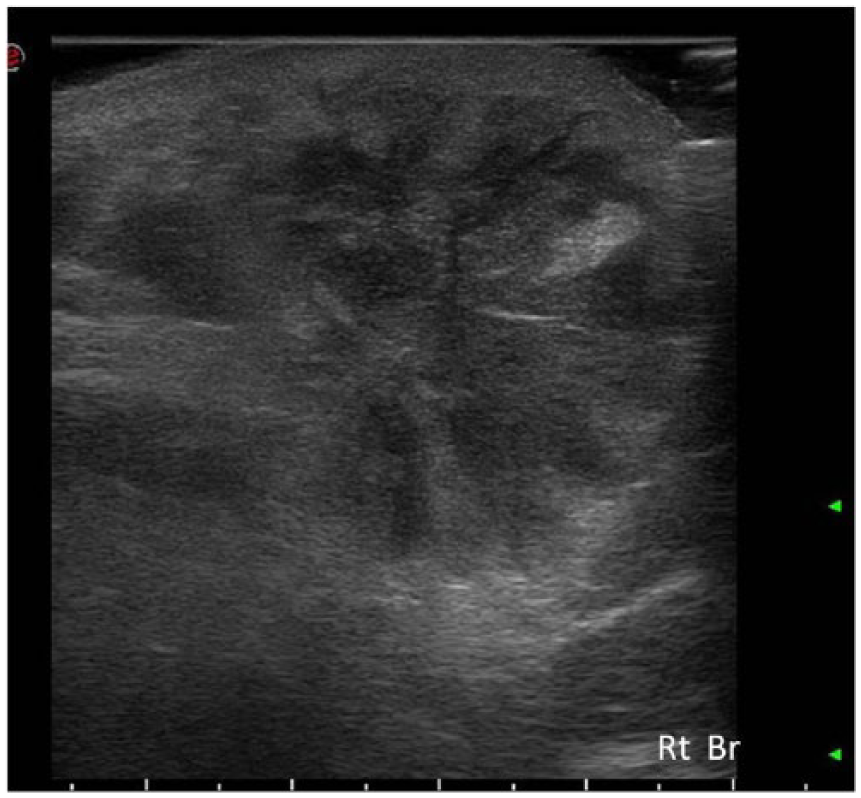
A right breast sonogram shows a diffuse mass with ill-defined margins and heterogeneous internal echo-pattern.
Case 3
A 15-year-old female, having normal periods for the last eight months, presented with a lump in the left breast. The lesion appeared soon after menarche and had grown to the present size. On palpation, it was a freely mobile lump measuring approximately 10.3 × 6 cm, mainly occupying the upper and outer quadrants of the breast.
The sonographic findings demonstrated a large lobulated space-occupying lesion with well-defined margins and mostly homogeneous echo-pattern (Figure 3). This area was iso- to hyperechoic as compared to normal breast tissue. The posterior echo-intensity was unaffected. A biopsy was performed and confirmed the neoplasm to be a juvenile fibroadenoma.
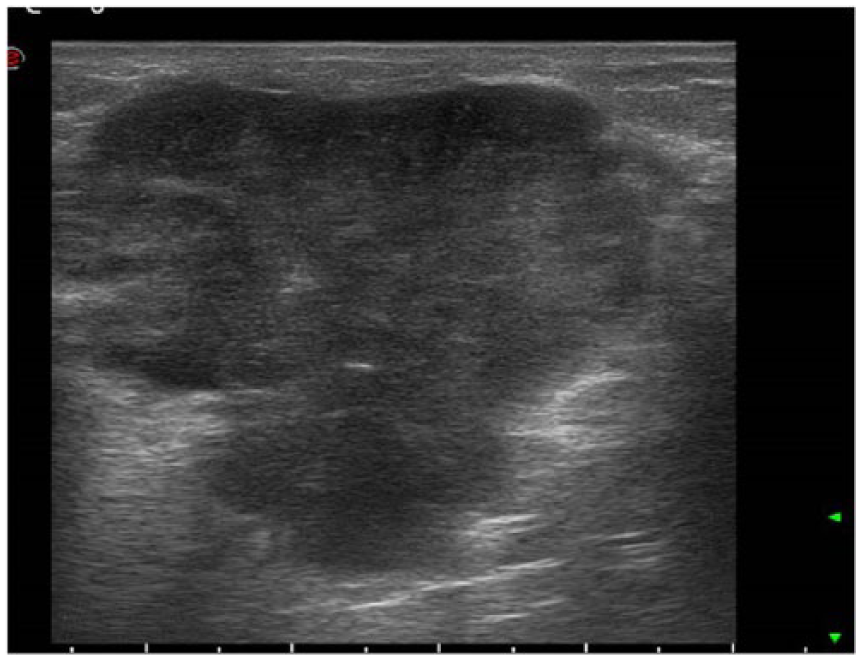
A sonogram of the breast that demonstrates a lesion with well-defined margins and homogeneous echo-pattern.
Discussion
Juvenile fibroadenomas of the breast are benign but rare neoplasms, which most often occur during the developmental phase of the breast and are poorly understood because of their rarity and unpredictable behavior.1–3 Pathologists define them as a variant of a large fibroadenoma. They appear to be more cellular than the adult type of fibroadenoma. 4 These neoplasms are characterized by proliferation of epithelial and connective tissue elements in varying proportions. Hormonal influences are thought to be contributory factors. Biochemical studies have shown that most fibroadenomas have progesterone receptors but lack estrogen receptors. 5
Juvenile fibroadenomas are rapidly growing breast neoplasms with diameters exceeding 10 cm2. The disease is often confined to one breast as a solitary mass occupying part or most of the breast. The mass rapidly grows to a large size and the patient presents with breast enlargement, nipple displacement, and sometimes pain. The overlying skin is stretched and shiny with dilated cutaneous veins.
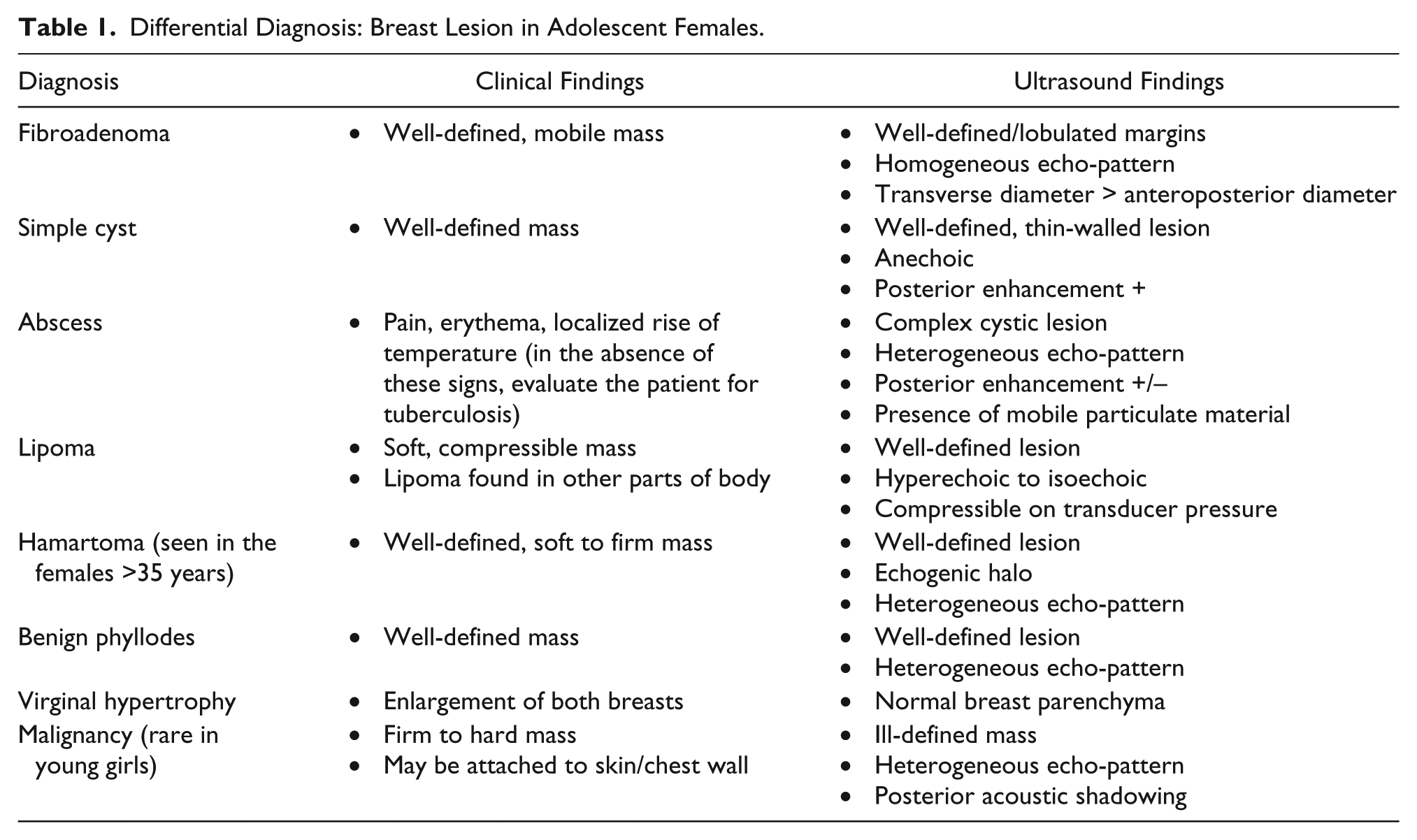
Juvenile fibroadenomas have to be differentiated from other mimicking benign pathologies to include cysts, abscesses, lipomas, hamartomas, phyllodes tumors, and virginal hypertrophy (Table 1). The imaging modalities and the extent of imaging required for the evaluation of a breast mass depend on the age, risk status of the patient, and degree of clinical suspicion. Sonography is the modality of choice for young girls in whom mammography is not preferred because of radiation exposure, dense breast parenchyma at this age, and inability of mammography to distinguish between solid and cystic lesions.1,2
Differential Diagnosis: Breast Lesion in Adolescent Females.
Simple breast cysts are reliably diagnosed using sonography. Cysts are typically seen as a well-defined, round, thin-walled anechoic lesion with posterior enhancement and needs no further intervention, unless the cyst appears complex or is causing symptoms. 1
An abscess appears as a complex cystic lesion. On a sonogram, the margins may be ill-defined. It typically has a heterogeneous internal echo-pattern. There can be the presence of mobile particulate material within it. The demonstration of posterior enhancement depends on the nature of the internal contents. The clinical symptoms can include pain, erythema, and localized rise of temperature at the site of the abscess. The absence of these clinical signs with sonography findings of abscess should warrant a clinician to evaluate the patient for tuberculosis of the breast.6,7 The medical management of the lesion depends on underlying pathology.
A lipoma of the breast is a benign lesion with a very limited risk of malignant transformation. It is a soft, mobile mass felt on palpation. On sonography, a lipoma is hyperechoic to isoechoic. Sometimes it can be hypoechoic. It can have thin echogenic septa. Sonography can also help demonstrate the softness and compressibility of a breast lipoma with a decrease in the anteroposterior diameter of the lipoma with mild transducer pressure. In an adult patient, mammography shows a translucent mass surrounded by a thin radio-opaque capsule. Small lipomas typically are followed up when large lesions require excision. Many patients with a breast lipoma also have lipomas in other parts of the body. 8
Hamartomas are benign lesions composed of variety of normal breast components arranged in disorganized manner. Most of these lesions occur in females greater than 35 years. They are rarely seen in adolescents. Patients present with a soft to firm lump. Sonographically, hamartomas have a heterogeneous appearance with varying internal echotexture. The lesion has an echogenic halo, without intratumoral calcification and absent retrotumor acoustic phenomenon. As there is chance of recurrence and also the possibility of malignancy arising from the epithelial elements of hamartoma, excisional biopsy is the treatment of choice. 9
Another pathology that is clinically not distinguished from juvenile fibroadenoma is benign phyllodes tumor. With this lesion, prominent leaf-like architecture is seen due to stromal cellularity in phyllodes, which is lacking in a fibroadenoma. FNA does not reliably differentiate between juvenile fibroadenoma and phyllodes. Because of this, a complete surgical excision is typically performed for diagnostic and treatment purposes. 10
The pathology has to also be differentiated from benign virginal hypertrophy, which is usually bilateral. There is usually diffuse enlargement of the breast without any associated mass or dilated cutaneous veins. 11
Malignant tumors of the breast are rare in young girls. The age-adjusted incidence of all malignant pediatric breast tumors in 2003 was 0.08 cases per 100,000 people. 12 But occasionally, unusual and aggressive malignant breast lesions are reported. 13
In conclusion, juvenile fibroadenomas are not a common pathology. When radiologists do come across fibroadenomas, they may be perplexed reviewing a large breast mass in a pediatric patient. The discussion above includes differential diagnoses of such breast lumps in this age group and also features that differentiate benign fibroadenoma from more sinister etiologies.
A palpable breast mass in a young female is a cause of worry and motivates parents to seek medical advice. Sonography remains the mainstay for investigating breast lesions in this age group. It is an economical, radiation-free, and readily accessible imaging modality. It reliably differentiates cystic from solid breast masses and reduces the number of biopsies performed for benign cysts. A biopsy would most likely be unnecessary in a patient in whom sonography shows hyperechoic fibrous tissue to be the cause of the palpable lump. Sonography also helps to evaluate suspicious breast masses, which require immediate biopsy or excision rather than follow-up. A breast sonogram can define the extent of the pathology and help to identify nonpalpable masses elsewhere in the breast. These findings can influence the choice of surgery that can be executed, without possibly disfiguring the breast of a young female.14–16
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.