
Abstract
Paget-Schroetter syndrome (PSS) is a rare diagnosis characterized by thrombosis of the axillary-subclavian veins. It can occur from thoracic outlet syndrome (TOS) that may result in deep vein thrombosis (DVT) or life-threatening complications if left untreated. Sonography is the primary imaging modality used for suspicion of DVT. Other modalities may be used for difficult diagnoses such as PSS where the exact location of venous compromise is important to know for appropriate treatment. This case report details the importance of early diagnosis and treatment of PSS from injury-induced TOS.
Keywords
Paget-Schroetter syndrome (PSS), also known as effort thrombosis, refers to the thrombosis of the axillary-subclavian veins that typically occurs from repetitive strenuous activity of the upper extremities. Injury-inflicting trauma to the thoracic outlet can also contribute to PSS. 1 Paget-Schroetter syndrome is a rare disease with an incidence between 1 and 2 out of 100,000 people annually. It occurs most commonly in young individuals who are physically active and laborers with continued overuse of the upper extremities. 2 In this particular case, PSS resulted from injury-induced thoracic outlet syndrome (TOS).
Case Report
A 40-year-old female patient presented to the emergency department with a sudden onset of worsening right upper extremity pain, swelling, discoloration, and numbness. She reported having a traumatic fall two months prior where she landed on an outstretched arm. Radiographs were taken that showed no evidence of fractures.
An upper extremity ultrasound was performed using a Philips iU-22 system (Philips Medical, Bothell, Washington) with a 9-MHz linear transducer and 8-MHz curvilinear transducer. A lack of venous compression and adequate blood flow showed occlusive deep vein thrombosis of the right external jugular, subclavian, and axillary veins (Figure 1). A computed tomography (CT) angiogram later confirmed the upper extremity deep vein thrombosis (DVT) consistent with PSS and bilateral segmental pulmonary emboli. The patient did not have a significant medical or family history of clotting disorders.
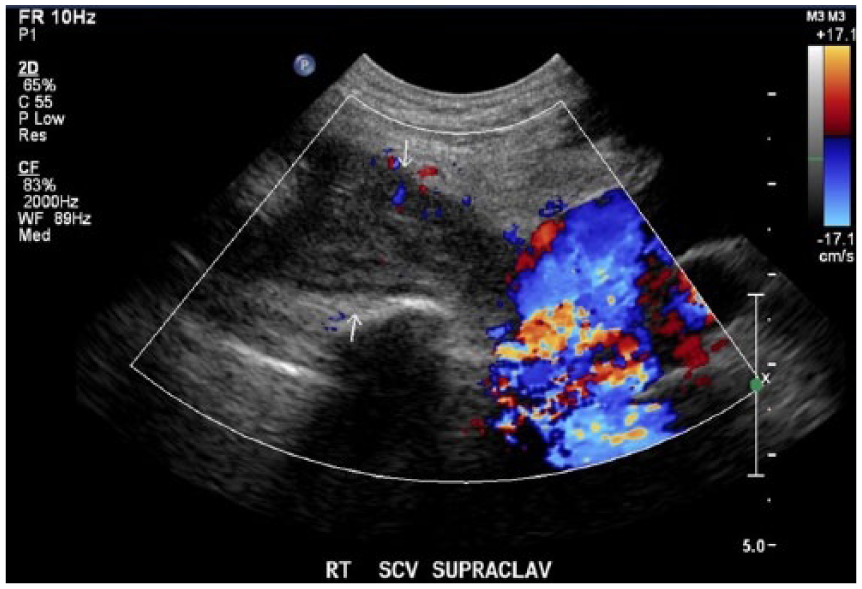
Color Doppler sonogram showing patency of the innominate vein and occlusive deep vein thrombosis (DVT) of the subclavian vein. The arrows point to the occlusive DVT of the subclavian vein.
A thrombectomy procedure was performed following the results from the sonogram and CT. Sonography was used to gain access to the right basilic vein under direct visualization. Fluoroscopy was used for guidance and demonstrated the near-total occlusion of the axillary-subclavian veins (Figure 2). Using a Kumpe catheter and a glide wire, the thrombus was bypassed, and the wire and catheter were placed in the inferior vena cava. Suction thrombectomy of the axillary-subclavian veins was performed. Several passes were made, and approximately 300 cc of blood and clots was removed. A repeat venogram demonstrated relief of the clot within the axillary vein, but a persistent clot in the right subclavian vein was seen. An infusion of tissue plasminogen activator (TPA) and heparin was started to treat the remaining thrombus. The patient tolerated the procedure well; however, a first rib resection was recommended to further resolve the thrombus and alleviate the narrowing of the thoracic outlet from impingement.

Venogram of the axillary-subclavian veins showing the near-occlusive thrombus and catheter placement prior to thrombectomy. Arrow indicates catheter placement in the axillary-subclavian vein.
A follow-up sonogram was performed one month after the procedure, which showed mild recanalized thrombus in the subclavian and axillary veins. The right subclavian vein showed areas of eccentric linear filling defects representing a chronic clot (Figure 3).
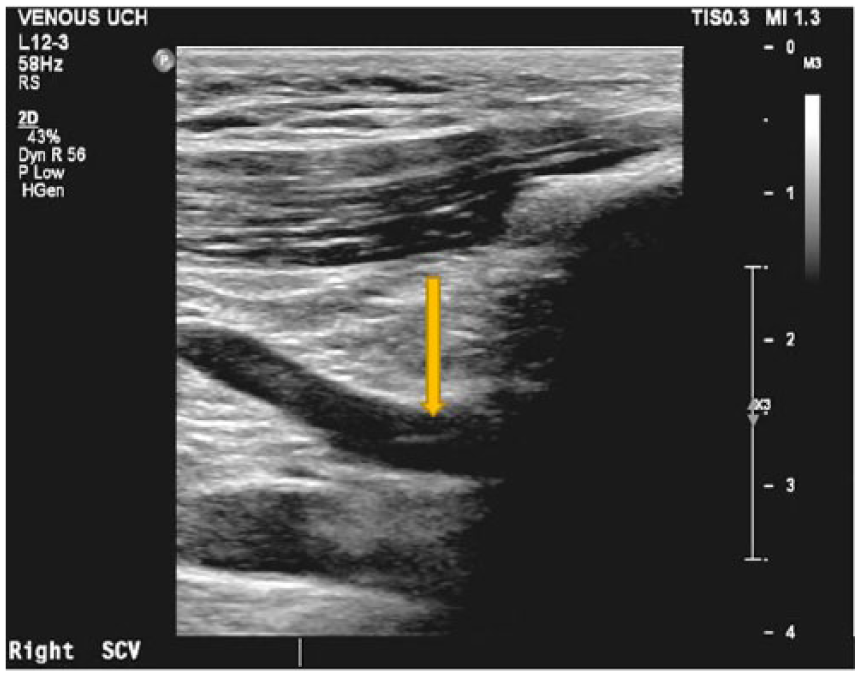
Gray-scale sonogram showing a linear fibrin sheath indicated by the arrow within the right subclavian vein consistent with chronic deep vein thrombosis.
The patient later underwent general anesthesia for a transaxillary first rib resection. A right upper extremity anterior scalenectomy and placement of On-Q pain pump catheter was also performed. A chest radiograph was ordered following the procedure (Figure 4).
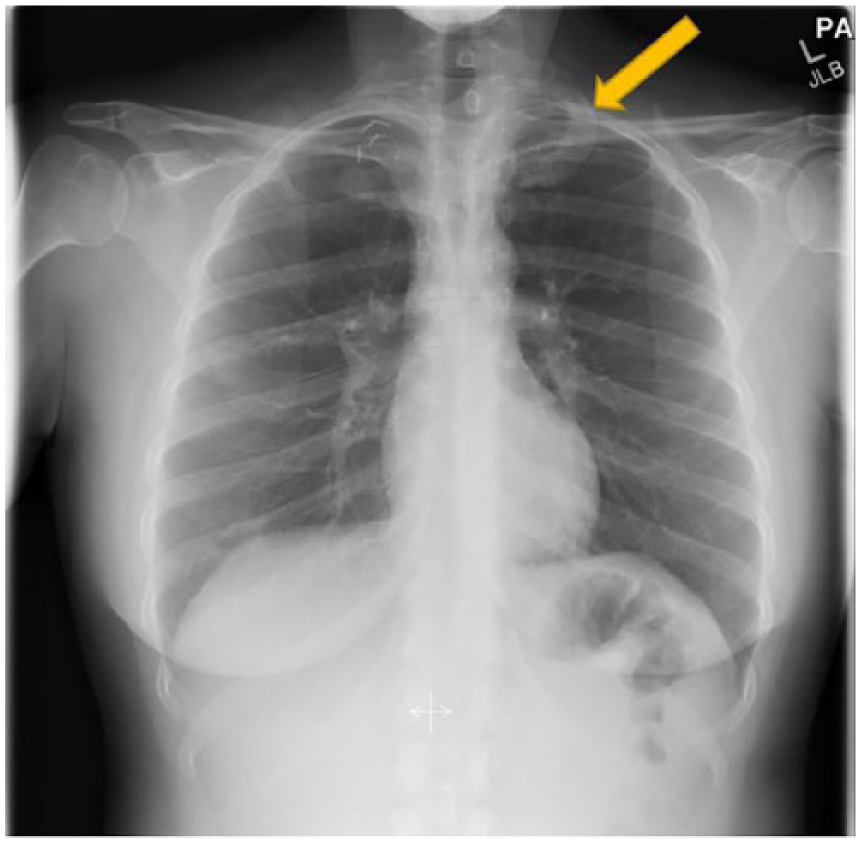
Chest radiograph taken postsurgical resection of the right first rib due to impingement. Arrow indicates the left first rib on the contralateral side for comparison postsurgery.
Following the transaxillary first rib resection, a sonogram was performed that showed patency of the right internal jugular, subclavian, axillary, basilic, brachial, and cephalic veins. Using pulse-wave Doppler, the examination demonstrated continuous flow without pulsatility of the infraclavicular subclavian vein with residual flow restrictions as expected in a posttreated vein (Figure 5). She was discharged the same day without complications.
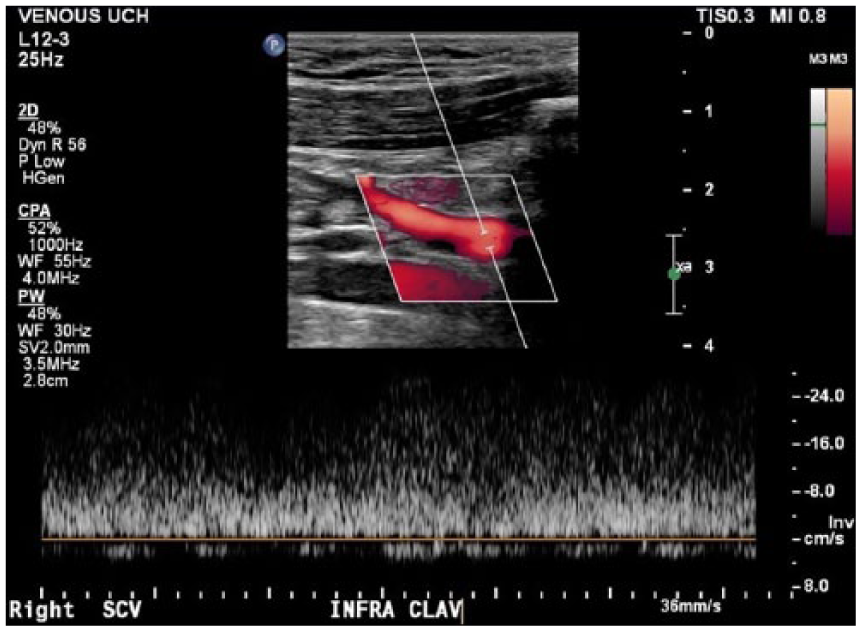
Pulse-wave Doppler sonogram displaying continuous flow with a lack of pulsatility as one would expect in a posttreated vein.
Discussion
Upper extremity DVT accounts for up to 11% of all positive DVT cases and most commonly occurs from central venous catheter placement. 2 TOS increases the risk of developing DVT in the upper limb by restricting proper blood flow throughout the underlying vessels. Injury, obesity, poor posture, repetitive motion, and structural abnormalities can all contribute to TOS. 3
Bone abnormalities may be a potential cause of TOS, with an incidence of approximately 29%. The clavicle accounts for roughly 20% and the first rib accounts for only 10% of all TOS. 4 The most common bone abnormality to cause TOS is a cervical rib (70%) that arises from the seventh cervical vertebra. 4 Although even more uncommon, injury to these structures may also contribute to the development of TOS.
The narrow space between the clavicle and the first rib is considered the thoracic outlet. The subclavian vein extends from the innominate vein peripherally until the cephalic vein confluence and is then considered the axillary vein. Arteries accompany the veins within the deep system, all of which may become compromised from TOS. TOS is a condition in which compression of these blood vessels and also nerve bundles causes symptoms of diffuse pain, swelling, numbness, discoloration, and weakness in the extremity. 3
TOS most commonly affects women, with a ratio of 4 to 1, between 20 and 40 years of age. 5 Several types of TOS are classified according to the structures that are compromised. The most common incidence is neurogenic TOS (94%–97%), whereas venous TOS occurs in less than 5% and arterial TOS in less than 1% of the population diagnosed with TOS. 4 In the setting of a narrowed thoracic outlet, compressed axillary-subclavian veins are referred to as venous thoracic outlet syndrome. Once DVT develops in the subclavian vein, PSS can be diagnosed. 3
The interscalene triangle is the most common site of compression but can also occur in the costoclavicular space or the retropectoralis minor space. Arteries, veins, and nerves can become compromised, causing a variety of symptoms. Neurogenic symptoms are the most common and occur from compression of the peripheral nerves of the brachial plexus and may result in pain, paresthesia, dysesthesia, and weakness in the upper limbs. Vascular compromise may present with swelling, edema, skin changes, and also weakness. It is not uncommon for a patient to present with mixed symptoms if multiple structures are involved. 5 In this case study, PSS resulted from TOS inflicting venous compromise.
The diagnosis of PSS requires various imaging modalities. Venous duplex sonography is typically the initial diagnostic method used for cases of thrombus because it is noninvasive and cost-effective. Compression and color Doppler waveform analysis are highly sensitive in the diagnosis of DVT. Patent veins should fully compress with transducer pressure, whereas a thrombosed segment may not or only partially compress. Color and pulse-wave Doppler are also important for evaluating blood flow in the upper extremity. Dampened venous waveforms may be seen distal to the level of the clot. Magnetic resonance imaging (MRI) and CT angiography can be especially helpful in showing upper extremity DVT and the relationship to surrounding structures. However, these modalities are costly and typically use contrast agents that carry risk factors for the patient. Thoracic outlet syndrome is a complex diagnosis and typically requires several imaging modalities to determine its cause. 6
Early diagnosis is important in the setting of TOS to avoid severe complications. Arterial compression can cause limb ischemia or even stroke if emboli are formed. Venous involvement can lead to postphlebitic syndrome if DVT persists without treatment. Although uncommon, phlegmasia cerulea dolens and venous gangrene have also been reported with untreated TOS. Chronic thrombus may result in scarring and inhibit normal blood flow. In the acute setting, DVT can lead to life-threatening pulmonary emboli. 5 Treatment depends on the specific findings associated with TOS.
Venous thrombolysis is the favorable treatment option for upper extremity DVT. Anticoagulants such as heparin are often used as a first-line defense. If thrombus persists, venography and surgery may be indicated. In severe cases of chronic obstruction, a long saphenous vein patch or an endovascular stent implant may be medically necessary. In the case of lower extremity DVT, an inferior vena cava filter may be used as a form of embolus protection. With TOS, depending on the cause and location of the narrowing, physical therapy can be done to strengthen and stretch the muscles to correct for poor posture, which may relieve pressure in the thoracic outlet. 3 If there is a structural abnormality such as impingement from a rib, surgical decompression may be necessary and is considered the gold standard for treating TOS. 5
Conclusion
This case details the importance of early detection of thrombus to prevent further complications of TOS. Although several imaging modalities may be needed to diagnose TOS, sonography plays a key role in detecting venous thrombosis associated with PSS. Identifying the type of TOS is also important for establishing the correct treatment option.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.