
Abstract
Clear cell renal cell carcinoma (RCC) is proposed to arise from the proximal convoluted tubules within the kidney. Diagnostic imaging plays a role in the detection of RCC. A case is presented of a clear cell RCC that was initially identified sonographically. Sonography detected and characterized the mass, which was further evaluated with computed tomography (CT) to obtain additional information, prior to a radical nephrectomy. The use of both CT and sonography led to proper diagnosis and treatment of this suspected tumor.
Renal cell carcinoma (RCC) is the most common of all renal neoplasms and represents 85% of all kidney tumors. Diagnostic imaging plays an important role in detecting renal carcinomas. In this case, clear cell RCC was initially detected using sonography. Computed tomography (CT) helped diagnose, determine size, and discern whether or not metastasis had occurred. The typical sonographic findings of RCC include but are not limited to cystic or complex mass, areas of calcifications, displacement of renal pyramids, irregular margins, and hypervascularity. Although sonography can reveal RCC characteristics, the importance of providing a differential diagnosis can also aid in determining the renal pathology. The 2007 statistics for RCC indicated that there were 51,190 new cases and 12,890 deaths from renal cancer; the trend is expanding and growing over time. The discovery with diagnostic imaging modalities of RCC is crucial in the outcomes for many patients. The imaging presentation of renal pathology is unique, and viewing multiple case studies can aid in providing a proper diagnosis.
Case Report
A 61-year-old woman presented to the sonography department with an indication of nausea. A right upper quadrant sonogram was ordered as well as a CT with contrast of the chest. The CT examination demonstrated the aorta and great vessels to be in proper position, normal heart size, and no supraclavicular or axillary adenopathy. The CT images displayed no significant interstitial, intraparenchymal, or pleural abnormality. The patient did not have any prior medical lab work.
Using a GE Healthcare (Chicago, IL) ultrasound machine with a 5-MHz curvilinear probe, real-time transabdominal sonography was performed. The sonogram revealed a 12-cm × 8-cm × 10-cm complex, lobulated, soft tissue mass in the inferior half of the right kidney (Figures 1 and 2). Malignancy was immediately suspected due to the hypervascularity (Figure 3). The probable diagnosis was RCC or hypernephroma. The liver had uniform echogenicity without any metastatic extension or abnormal vascularity. The pancreas was well imaged with normal echotexture. The gallbladder had no evidence of cholelithiasis or cholcystitis. The common bile duct was normal in size. The patient exhibited no tenderness in the right upper quadrant during the examination.

Sagittal gray-scale sonogram of the right kidney showing a complex, lobulated mass measuring 11.95 cm long and 8.01 cm wide.
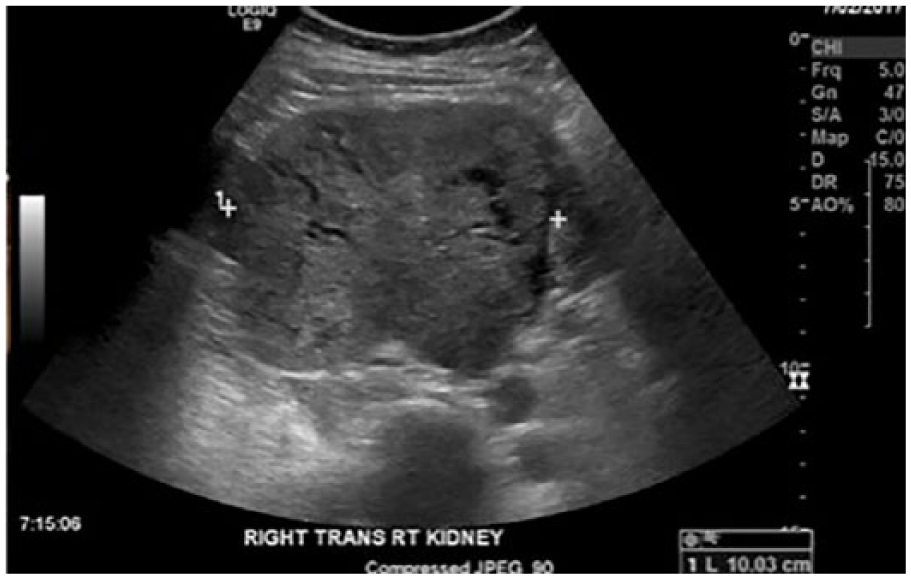
Transverse gray-scale sonogram of the right kidney showing the complex, encapsulated tumor, measuring 10 cm wide.
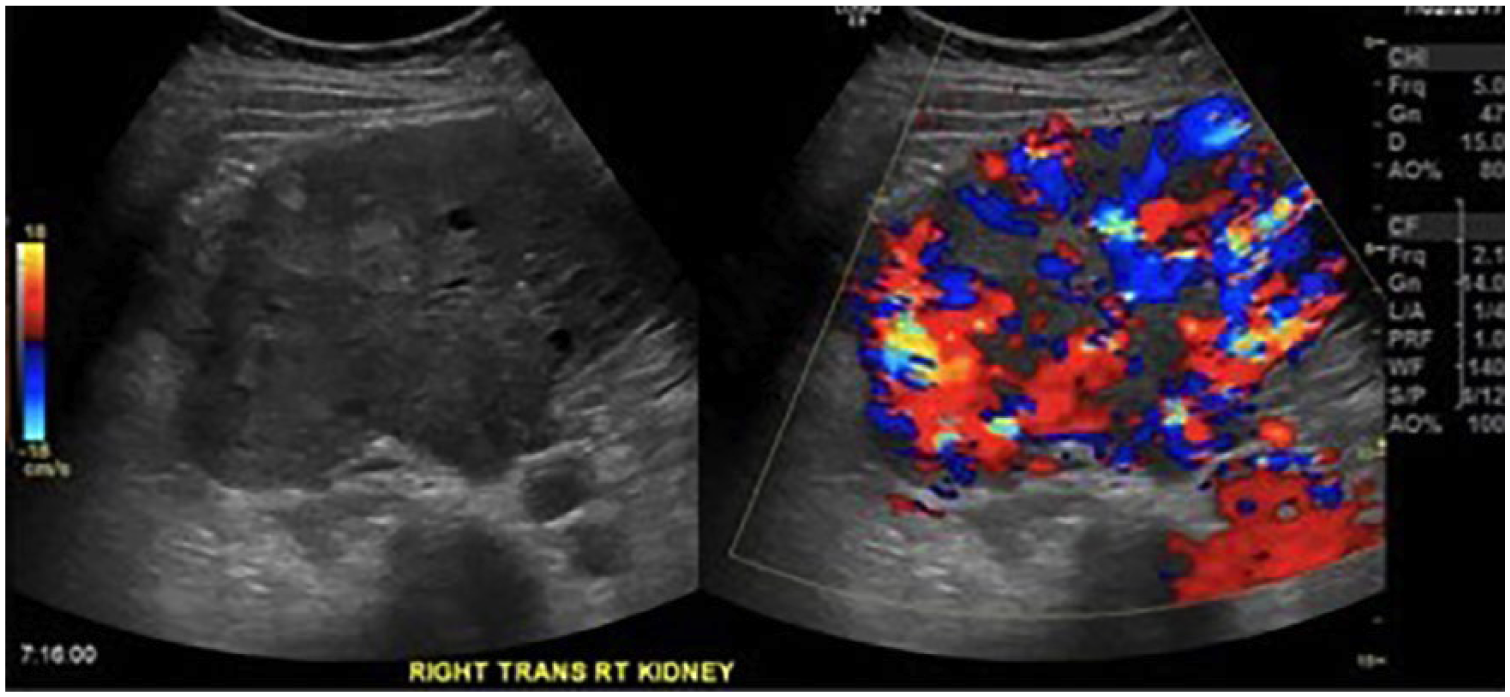
Transverse color Doppler sonogram of the right kidney showing hypervascularity within the mass.
Due to the sonographic findings, a CT of the abdomen with and without contrast was ordered. The liver was uniform in density, and enhancement of the contrast did not reveal any masses or abnormal vascularity. The left kidney, adrenal glands, spleen, and pancreas were all unremarkable. The right kidney was asymmetrically enlarged, with a microlobular mixed density involving the inferior two-thirds of the kidney consistent with RCC (Figure 4). The CT revealed calcifications in the inferior collecting system, hydronephrosis, and nephrolithiasis in the right kidney. The renal artery showed no obstructive change, thrombus, or abnormality.

Computed tomogram showing the mass located in the right kidney, measuring approximately 13 cm.
A CT of the pelvis with and without contrast was ordered and displayed no free fluid, adenopathy, or bony abnormality. The bowel, ureters, and bladder were unremarkable.
Due to the severity of the disease, a right radical nephrectomy was performed. The operative report stated that the tumor showed signs of necrosis but was limited to the right kidney. The approximate tumor size was 13 cm with no evidence of local, regional, or distant disease in the chest, abdomen, or pelvis. The final diagnosis was clear cell RCC, grade 4. The patient had no plan for chemotherapy, but the oncologist prescribed targeted therapy drugs postsurgery to ensure remission.
Discussion
The kidneys are located in the retroperitoneal cavity along the posterior abdominal wall. 1 The kidneys are “bean-like” in shape and narrow medially, where the vessels converge to form the hilum. The hilum consists of the renal vein, artery, and pelvis of the ureter. The kidneys are made up of a complex variety of components to control the composition of blood by removing harmful wastes and conserving water and metabolites. 1 The outer portion of the kidney is the cortex and the inner portion is the medulla. The nephrons within the kidney are the functional units of the kidney. 1 The nephrons are composed of the renal corpuscle and renal tubules. The blood is filtered in the renal corpuscle through a variety of parts, including the glomerulus (network of capillaries), Bowman’s capsule (surrounds the glomerulus), afferent arteriole (blood enters glomerulus), and efferent arteriole (blood exits the glomerulus). 1 The renal tubule is where the filtrate passes into the renal tubule from Bowman’s capsule to go through the proximal convoluted tubule, to the loop of Henle, and to the distal convoluted tubule. The juxtaglomerular apparatus forms the distal convoluted tubule and the afferent arteriole to regulate blood pressure within the kidney.
Adult renal tumors both benign and malignant have many different types. The most common malignancy of the kidney is RCC. RCC can present in different forms, including clear cell adenocarcinoma, papillary, chromophobe, collecting duct, and unclassified. 2 RCC is the eighth most common malignancy affecting adults and accounts for between 3% and 4% of new cancer cases in the United States. 2 The classic presentation of RCC is flank pain and hematuria. Clinical signs and symptoms can also be nonspecific such as anorexia, weight loss, and fatigue. 2 In the United States, there were an estimated 51,190 new cases and 12,890 deaths from renal cancer in 2007, accounting for 2.3% of all cancer deaths. 2 The incidence has steadily increased over the years.
Most RCC occurs between the fifth and seventh decades of life. African Americans and males are at increased risk of developing this type of cancer. 2 Certain genetic conditions can also increase the risk, including von Hippel-Lindau (VHL) disease and tuberous sclerosis. Patients with acquired cystic renal disease who are on long-term dialysis carry a 3- to 6-fold increased risk of RCC. Other risk factors include smoking, obesity, hypertension, and human immunodeficiency virus infection. 2
Clear cell RCC is a heterogenous group of renal carcinomas with a clear or eosinophilic cytoplasm. 3 Clear cell RCC can be referred to as hypernephroma or Grawitz tumor and accounts for approximately 65% to 70% of adult renal cancers. 3 Clear cell RCC has a characteristic vasculature and common molecular signature of VHL inactivation. 3 When the VHL gene is inactivated, the VHL protein complex cannot degrade HIF-1-α (a transcription factor). 3 HIF stands for hypoxia inducible factor, and due to the inactivation of the VHL, there would be an increase in HIF leading to hypernephroma. 3 The proposed origin of the tumor is the proximal convoluted tubule. 3 Most RCCs appear encapsulated, solid, cystic, or mixed, including calcifications. 2 Histologically, clear cell carcinoma displays large uniform cells with abundant clear cytoplasm rich in glycogen and lipids. Clear cell carcinoma is highly vascular. 2
Sonographic evaluation of RCC can be useful when assessing for venous thrombosis, distinguishing cysts from hypovascular solid tumors, and revealing septations due to complex interfaces. 2 Venous thrombosis or venous migration of the RCC occurs in 4% to 10% of patients with renal neoplasms, and within this group, 2% to 16% may have tumors extending into the right atrium. 4 Moreover, venous thrombosis of RCC corresponds to the inferior vena cava (IVC) and the evaluation of metastatic spread of the disease. CT evaluation helps determine preoperative protocols and assess tumor staging. Magnetic resonance imaging is only used if CT cannot be performed due to allergies or pregnancy. 2 Percutaneous biopsies of renal lesions are not generally performed because the results usually do not affect recommended therapy, except in cases of multiple tumors or predisposing condition. 2
Clear cell RCC has two different prognostic factors: grading and staging. Grading for clear cell RCC is a three-tiered system in which nodular size, shape, and nucleolar prominence are assessed. 3 Grade I involves nucleoli inconspicuous or absent at 400× magnification. Grade II is when the nucleoli are prominent at 400×. Grade III is when the nucleoli are prominent at 100× magnification. Grade IV is when there is extreme nuclear pleomorphism, multinucleated giant cells, and sarcomatoid and/or rhabdoid change. 3
The staging system is more complicated. The TNM staging system is a tool to answer questions about the tumor (T), lymph node involvement (N), and metastasis (M). 5 The letter is placed in front the number to describe the size and location of the tumor. The numbering ranges from zero (no evidence of a primary tumor) to four (the tumor has spread beyond the areas of Gerota’s fascia and adrenal gland on the same side of the body as the tumor). 5 By combining the T, N, and M classifications, doctors are able to assign the stage of the cancer. 5 Stage I is when the tumor is 7 cm or less and only located in the kidney and has not spread to lymph nodes or distant organs. 5 Stage II is when the tumor is larger than 7 cm and is only located in the kidney and has not spread to lymph nodes or distant organs. 5 Stage III is when the tumor is of any size in one kidney and has spread to the regional lymph nodes but not other parts of the body or when the tumor has grown into the major veins or perinephric tissue but not other parts of the body. 5 Stage IV is when the tumor has spread beyond Gerota’s fascia, into the lymph nodes or another organ like the brain, bones, or lungs. 5
Treatment for RCC depends on several factors, including the type, cell type, and stage of cancer; possible side effects; and the patient’s preferences and overall health. 5 Surgery is most common to remove the tumor. The types of surgery include radical nephrectomy, partial nephrectomy, and laparoscopic surgery. Radical nephrectomy removes the tumor, the entire kidney, and surrounding tissue. 5 A partial nephrectomy is surgical resection of the tumor. 5 Laparoscopic surgery is a minimally invasive surgery to completely remove the kidney or perform a partial nephrectomy. 5 Other nonsurgical treatments include radiofrequency ablation or cryoablation and chemotherapy. 5
Local recurrence in the nephrectomy bed occurs in approximately 20% to 40% of patients, typically in the first five years after nephrectomy. The risks are highest when the resection margins are incomplete. 2 Chae et al. 6 analyzed the patterns of recurrence in 194 patients with RCC who had undergone complete resection with nephrectomy. Tumor recurrence was found in 21% of the patients within a mean time of 17 months. 7 Tumor recurrence occurred within two years in 83% of the patients. The recurrence rate was highest for those with an original tumor greater than 5 cm.
Patients with a tumor confined within the capsule achieved the highest 5-year and 10-year survival rates (88% and 66%, respectively). Survival rates decreased as the tumor invaded the perirenal fat (67% and 35%, respectively) or regional lymph nodes (17% and 5%, respectively). 8 The prognosis is determined by a combination of multiple characteristics. However, in this case, because the tumor was contained to the kidney and complete resection was performed, the statistics point to a higher survival rate for this patient.
In addition, since RCC is one of the most common solid tumors within the kidney, the more case studies presented can help make symptoms of this pathology more certain. The symptoms presented are very vague. The classic symptoms that are represented of RCC cases are hematuria, flank pain, and a palpable abdominal mass. The patient in this case study did not present with any of these symptoms. Further evaluation of RCC would suggest that the classic triad of symptoms is only present in a small percentage of cases. In the present case study, symptoms included nausea. The symptoms also rely on whether or not the tumor has spread. In this case, the tumor did not spread. Interestingly, the size of the tumor does not correlate to whether or not the tumor will extend into the IVC. Many published cases demonstrate RCC extending into the IVC and right atrium with a much smaller original renal cancer. In this case study, a much larger RCC was found, measuring almost 13 cm in length. The tumor was compelling due to the lack of symptoms and the absence of metastasis outside the kidney. A much smaller tumor that has spread can provoke other types of symptoms. The importance of reviewing the variety of renal cancer presentations is important for diagnosing and treating RCC quickly. Larger tumors in kidneys may go unnoticed due to the lack of symptoms, but recognizing the symptoms as early as possible may lead to further learning and presentation of different RCC stages.
Conclusion
RCC is the most common malignancy of the kidney. Clear cell RCC is a renal cortical tumor typically involving the epithelial cells with clear cytoplasm and a compact alveolar or acinar growth pattern interspersed with vasculature. 6 Surgical resection of the tumor is the primary treatment option; however, treatment depends on many factors. This case demonstrates that sonography can play an important role in detecting clear cell RCC and assist in proper diagnosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.