
Abstract
The purpose of this study was to determine the usefulness of virtual touch quantification (VTQ) and virtual touch imaging quantification (VTIQ) techniques for assessing undescended testes stiffness, by age and location. One testicle from each of 84 participants (31 of whom were healthy volunteers) was assessed by the point shear-wave elastography (p-SWE) method, using both VTQ and VTIQ techniques. The patients were grouped by location of assessment (intra-abdominal, inguinal, and scrotal) and age (group 1, healthy patients; group 2, patients age one and younger; and group 3, patients older than age one). Although the VTQ and VTIQ methods for group 2 showed similar results in the Bland-Altman plot, for group 3, the VTIQ method was more effective than the VTQ method. The use of p-SWE with VTIQ may be an appropriate technique for determining the tissue stiffness of testes located in the inguinal canal and for patients over one year of age.
Sonoelastography-based imaging techniques have received substantial attention in recent years for noninvasive assessment of tissue mechanical properties. These techniques take advantage of changed soft tissue elasticity in various pathologies to yield qualitative and quantitative information that can be used for diagnostic purposes. Measurements are acquired in specialized imaging modes that can detect tissue stiffness in response to an applied mechanical force (compression or shear wave). As a 2D shear-wave speed (SWS) measurement in which the SWS value is also expressed in meters/second. Virtual touch quantification (VTQ) and virtual touch imaging quantification (VTIQ) techniques can display color-coded images and measure localized SWS from 0.5 to 10 meters/second, using up to 256 spatial distributions of acoustic radiation force impulse (ARFI) push and pulse beams.1,2
Sonoelastography has been used extensively in pediatric imaging, especially in the assessment of pediatric liver diseases.3,4 There are only a few research studies in the literature regarding the usage of sonoelastography on testicular tissue,3–10 none of which compare the techniques of VTQ and VTIQ on undescended testicular tissue. Both techniques can be performed with a 9L4 linear probe, which can provide additional information about testicular stiffness.
The preferred imaging method to evaluate the undescended testes is sonography. But within sonoelastography imaging, it is easy to distinguish between the undescended tests and lymph nodes. However, the use of VTQ and VTIQ techniques could calculate more appropriate tissue stiffness results in selected areas.
Currently, VTQ and VTIQ techniques can only be assessed with one ultrasound equipment manufacturer. At this point, performing sonoelastography may require software and/or hardware upgrades to the systems. There are no differences regarding the physical principles between VTQ and VTIQ techniques. However, the VTQ technique does require only one measurement in a single area, whereas VTIQ demonstrates multiple tissue stiffness in different regions, within the selected region of interest (ROI). Second, before the assessment of tissue stiffness by the VTIQ technique, it is essential to determine the overall selected area of stiffness by using a color map. This issue is very similar to real-time strain elastography. In addition, color encoding and where to obtain the appropriate tissue stiffness can determine tissue stiffness. This reduces the subjectivity of the sonoelastographic measurements.
The aim of this study was to determine the usefulness of VTQ and VTIQ techniques for assessing undescended testes (cryptorchidism) depending on (1) age (under and over the age of one) and (2) location (intra-abdominal, inguinal, and scrotal).
The hypothesis was that VTQ and VTIQ techniques are useful to measure the tissue stiffness of undescended tests in a pediatric age group.
Materials and Method
Study Design
This was a prospective study conducted between April 2015 and March 2016. The hospital’s ethics committee approved the study and provided the consent form. The form was signed by individuals responsible for the (minor) patients, whose ages ranged from newborn to 12 years. The study was carried out in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Patients in the study were referred to the pediatric sonography department after being examined by a pediatric urology physician. After a physical examination, patients with suspected undescended testes were enrolled in the study for ultrasonographic (US) examination. The patients underwent an US examination of one testicle, and then their medical records were used to confirm the location of the testicle. Testicle location was the initial criterion for inclusion in the research study.
Patient Selection
US studies were conducted on the same day as the patient’s referral to the pediatric sonography department. Patients with bilateral undescended testes, nonpalpable undescended testes, retractile testes, endocrine diseases, systemic diseases, and incomplete data were excluded from the study. Prior surgery was also an exclusion criterion. Patients diagnosed with abnormal lymph nodes were also excluded from the study.
Patients were divided into three groups: group 1 comprised volunteers with normally located testes, group 2 was composed of males age one or under with an undescended testicle, and group 3 members were males older than one year with an undescended testicle. Only one testicle of each patient was evaluated. Normal testicular tissue of the undescended patients was not included in the study because of the principle that histopathologic sections might have been affected in various stages of embryological development.4,11
Pathologic changes in undescended testes occur with age. Microscopic changes in testicle parenchyma begin in undescended testes at six to nine months of age. 5 Many authors consider the age of one year to be the upper limit for surgery 2 ; therefore, one year was chosen as the cutoff value for the treatment of testicular tissue stiffness using sonoelastography in this study.
Equipment and Scanning
A Siemens Acuson S2000 ultrasound system (Siemens, Mountain View, California) was used for the sonoelastography examination, and measurements were made by one expert, a pediatric radiologist with three years of experience in sonoelastography. A surface 9L4 linear probe was used in the studies. B-mode and sonoelastographic studies were performed while the patient was in a supine position. First, B-mode US was used to locate the undescended testicle. None of the patients were sedated during the examination. Patients were measured at a time of inactivity in the appropriate supine position. After locating the testicle by B-mode US, the testicle volume was calculated in three dimensions.
Testicular volume was measured after the maximum length, width, and height were obtained from the US. The volumes were calculated with the formula for an ellipsoid. 3
After testicular volume was determined, testicular blood flow was measured with Doppler sonography. Patients with external factors such as testicular torsion or epididymitis, which may affect testicular parenchymal tissue, were excluded.
Evaluation of Point SWE
During the point SWE (p-SWE) examination, the transducer was placed on the skin surface over the testicle, and the minimum necessary pressure required to achieve the desired result was applied. Where feasible, axial or longitudinal images were used to obtain appropriate images for the p-SWE examination. All measurements were completed with a 9L4 probe. Once the sonoelastography was performed, the testicular tissue was measured within a square determined by the VTQ software. The ROI scale was fixed at 0.5 × 0.5 cm. At least six valid measurements were obtained (Figures 1–3).
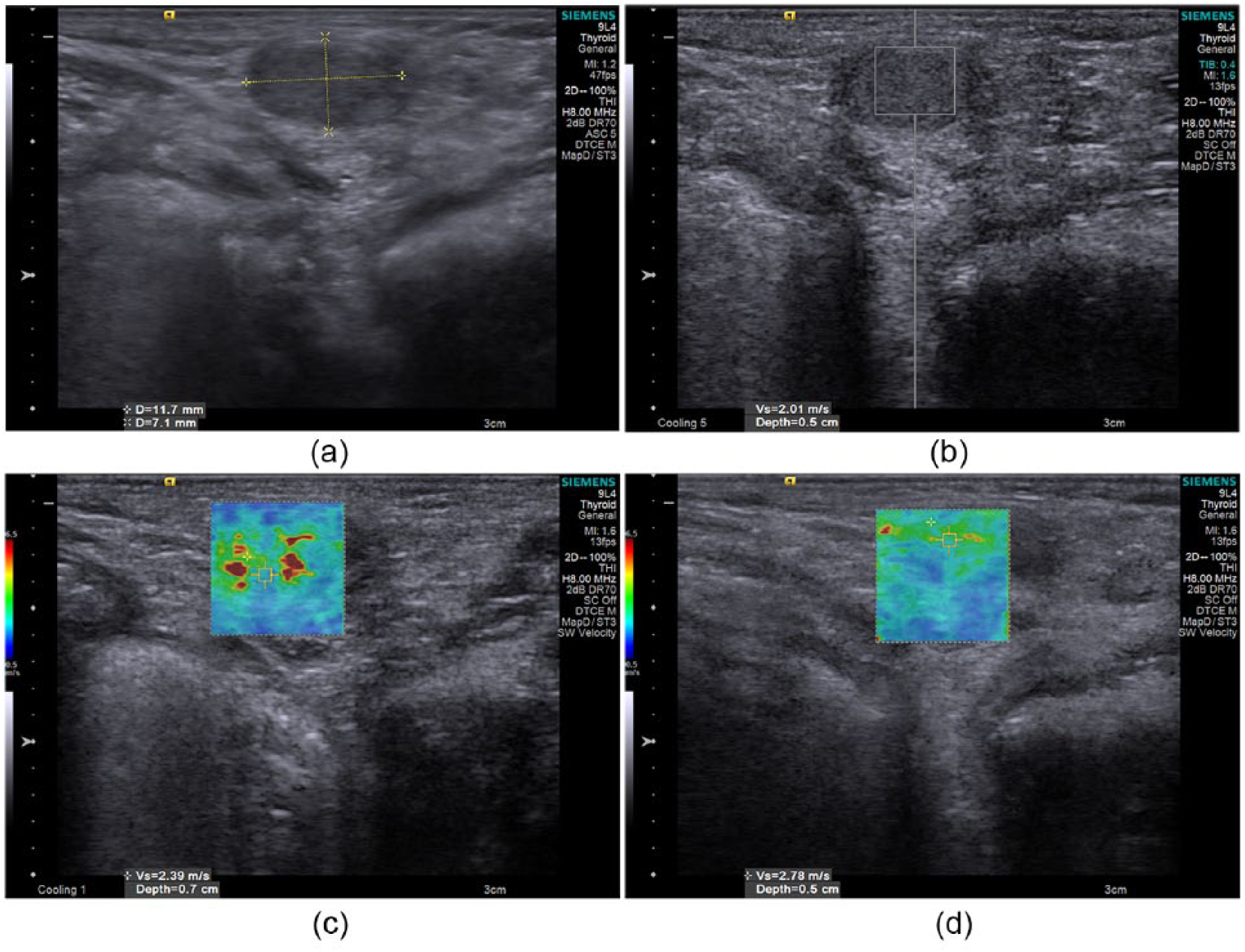
Point shear-wave elastography of undescended testicle located at the superior aspect of the inguinal canal in a two-year-old child. (a) B-mode sonographic examination of undescended testes. (b) Data obtained by virtual touch quantification (VTQ) at the depth of 0.5 cm with a velocity of 2.01 m/s. (c) Data obtained by virtual touch imaging quantification (VTIQ) at the depth of 0.7 cm with a velocity of 2.39 m/s. (d) Data obtained by VTIQ at the depth of 0.5 cm with a velocity of 2.78 m/s.
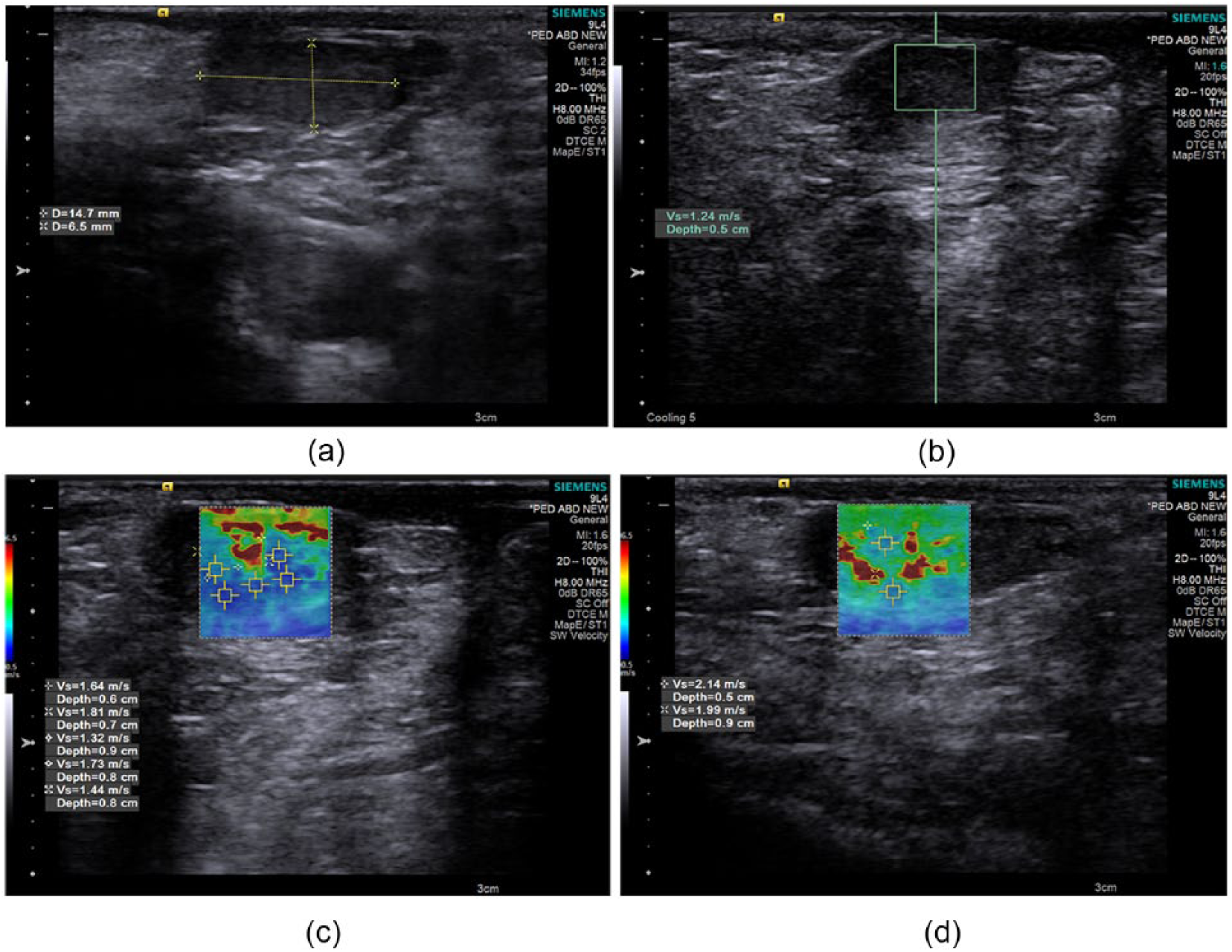
Point shear-wave elastography of undescended testicle located at the intra-abdominal location in a nine-month-old boy. (a) B-mode sonography examination of undescended testes. (b) Virtual touch quantification (VTQ) images of an undescended testes. The shear-wave value was 1.24 m/s when the region of interest was placed within testes at the depth of 0.5 cm. (c) Virtual touch imaging quantification (VTIQ) images of the same patient obtained from different depths. The color scale on the left side (blue to red) also shows the tissue stiffness (ranging from 0.5 to 6.5 m/s). (d) The same patient with different VTIQ measurements from different depths of ranges.
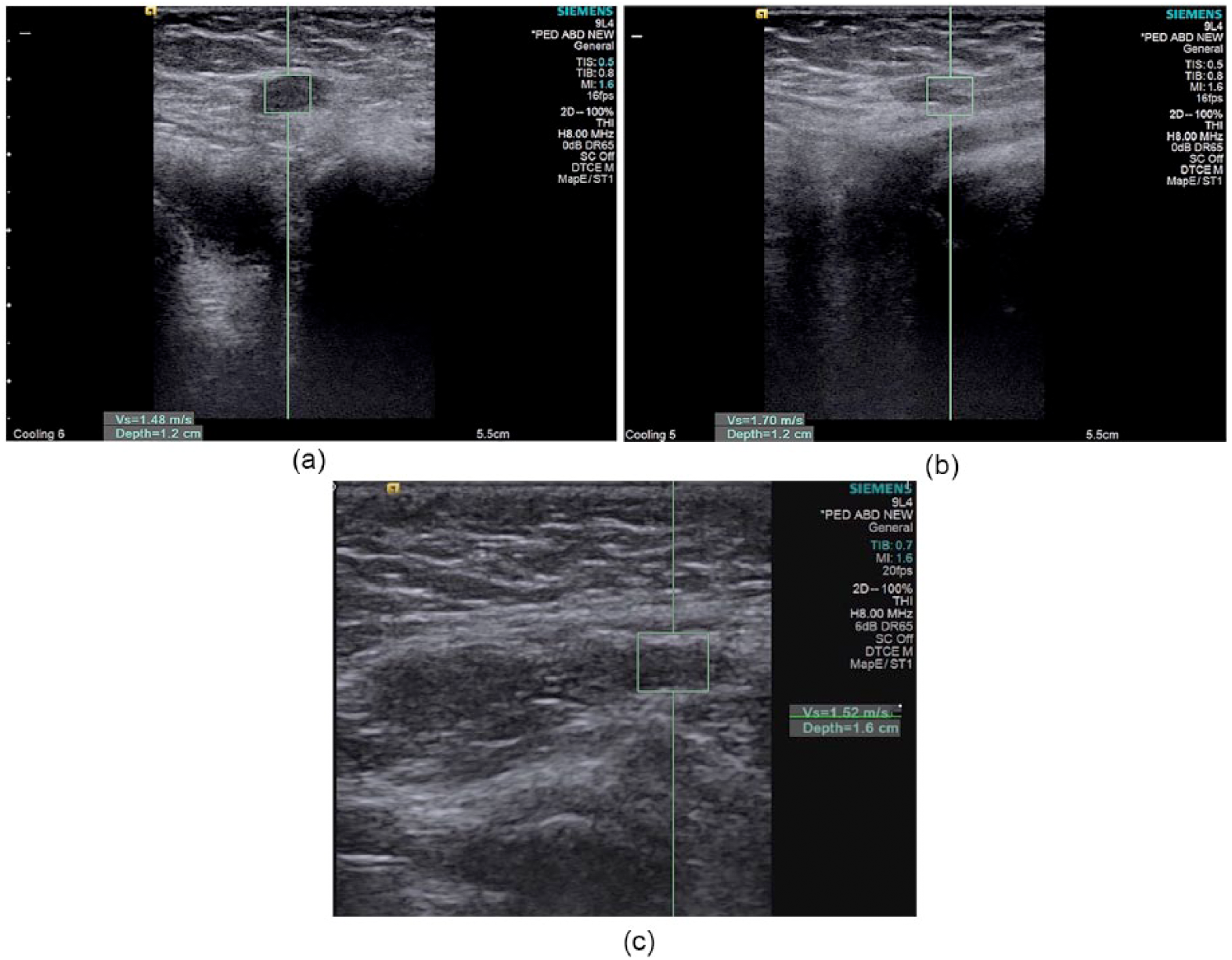
Point shear-wave elastography of an undescended testicle located at the inguinal canal location in an eleven-month-old boy. (a) Virtual touch quantification (VTQ) shows the shear-wave value of 1.48 m/s when the region of interest was placed within testes at a depth of 1.2 cm. (b) VTQ images of the spermatic cord in the same patient. The shear-wave value was 1.70 m/s when the region of interest was placed within the spermatic cord at 1.2 cm. (c) The shear wave value was 1.52 m/s when the region of interest was placed within the spermatic cord with the VTQ technique at a depth of 1.6 cm.
After VTQ squaring was determined, the patients underwent VTIQ. After replacement of the ROIs, the appropriate quality mapping was obtained, and measurements were made by the quantitative method (VTIQ). A color map was obtained by quality mapping to assess tissue stiffness. In this measurement technique, 10 distinct points with different ROI placements were measured and recorded. SWV values were quantitatively measured in meters/second, within the ROIs, and ranged from 0.5 to 10 m/s. This process took an additional 5 minutes (Figures 1–3).
Statistical Analysis
The statistical package program SPPS (version 20.0; SPSS, Inc., an IBM Company, Chicago, Illinois) was used to evaluate the data. The variables were the mean ± standard deviation and percentile and frequency values. In addition, the homogeneity of variances from the preconditions of the parametric tests was assessed using the Levene test. The assumption of normality was checked using the Shapiro-Wilk test. A one-way analysis of variance (ANOVA) was determined for three or more group comparisons. The Bonferroni-Dunn test was used for Kruskal-Wallis and multiple comparison tests when not provided by the Tukey honestly significant difference (HSD) test from multiple comparison tests. The difference between the two methods obtained by the comparison study was examined using the Bland-Altman method. Statistical significance was defined as P < .05 and P < .01.
Results
Study Descriptive Results
Table 1 shows the p-SWE evaluation for the VTQ and VTIQ techniques by age groupings. Table 2 shows the p-SWE evaluation for the VTQ and VTIQ techniques by testicular location. The number of participants assessed in each group is indicated by n.
Tissue Stiffness Results Based on the Age Groups for the VTQ and VTIQ Technique.
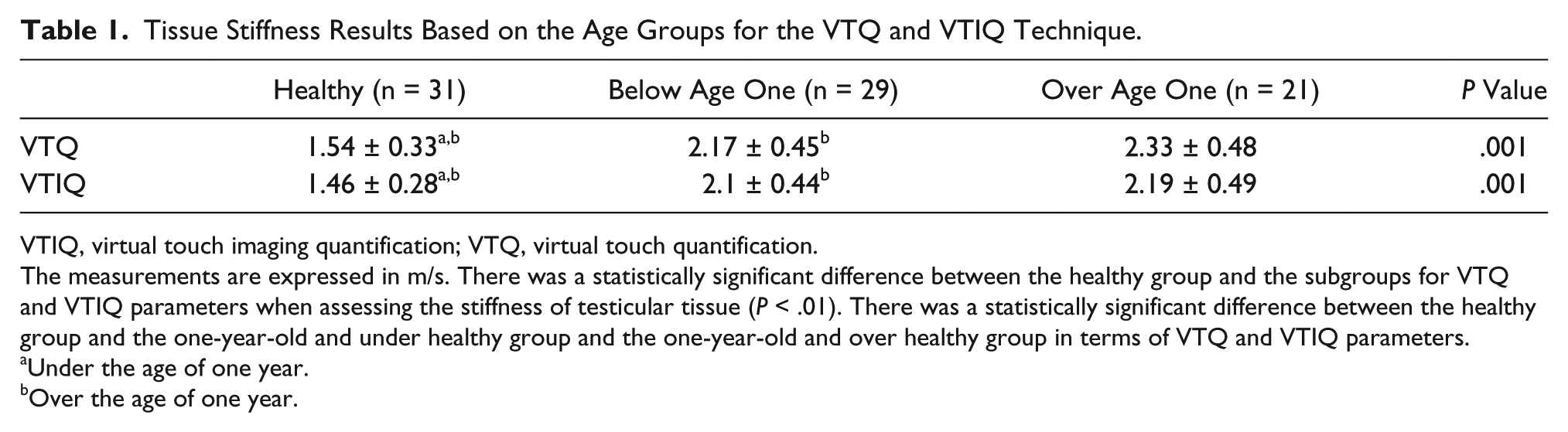
VTIQ, virtual touch imaging quantification; VTQ, virtual touch quantification.
The measurements are expressed in m/s. There was a statistically significant difference between the healthy group and the subgroups for VTQ and VTIQ parameters when assessing the stiffness of testicular tissue (P < .01). There was a statistically significant difference between the healthy group and the one-year-old and under healthy group and the one-year-old and over healthy group in terms of VTQ and VTIQ parameters.
Under the age of one year.
Over the age of one year.
Tissue Stiffness Results Based on the Localization of Groups for the VTQ and VTIQ Technique.
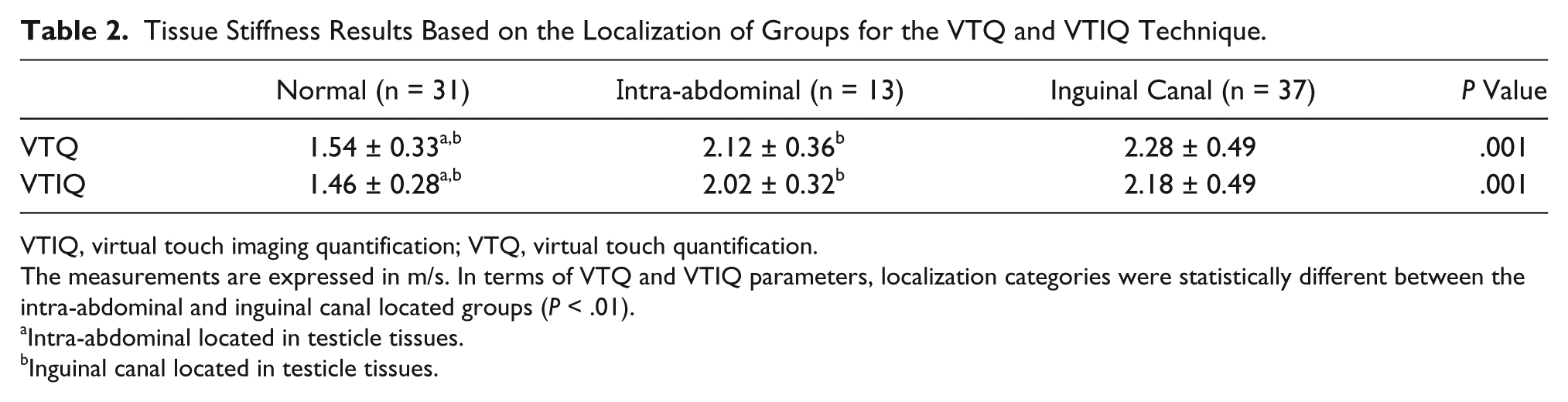
VTIQ, virtual touch imaging quantification; VTQ, virtual touch quantification.
The measurements are expressed in m/s. In terms of VTQ and VTIQ parameters, localization categories were statistically different between the intra-abdominal and inguinal canal located groups (P < .01).
Intra-abdominal located in testicle tissues.
Inguinal canal located in testicle tissues.
Determination of p-SWE Values in Comparison to the VTQ and VTIQ Techniques by Location and Age
There was a statistically significant difference between the healthy subgroups of age one and above in terms of the VTQ and VTIQ parameters (P < .01). There was a statistically significant difference between the healthy group and one-year-old, healthy group, one-year-old and one-year-old and over in terms of the VTQ and VTIQ parameters.
In terms of the VTQ and VTIQ parameters, the localization categories were statistically different between intra-abdominal, inguinal canal, and scrotal (normal) groups (P < .01). There was also a statistically significant difference in terms of the VTQ and VTIQ parameters.
Bland-Altman Distribution According to Age
Although the VTQ-VTIQ methods for patients aged one year and under showed more similar results in the Bland-Altman graph, the VTIQ method for patients over one year was better than the VTQ methods for patients over one year. Since the VTQ-VTIQ absolute value was used in the Bland-Altman graph, the VTIQ method for patients over one year was preferred. In contrast, in the one year and under age group, the results were not clear. In the one year and under age group, the Bland-Altman plots did not show a regular distribution (Table 3, Figure 4).
Standard Deviation of the Results of the Bland-Altman Plots Based on Age Group.

VTIQ, virtual touch imaging quantification; VTQ, virtual touch quantification.
The groups were divided by age: over and under one year old. n describes the patient numbers.
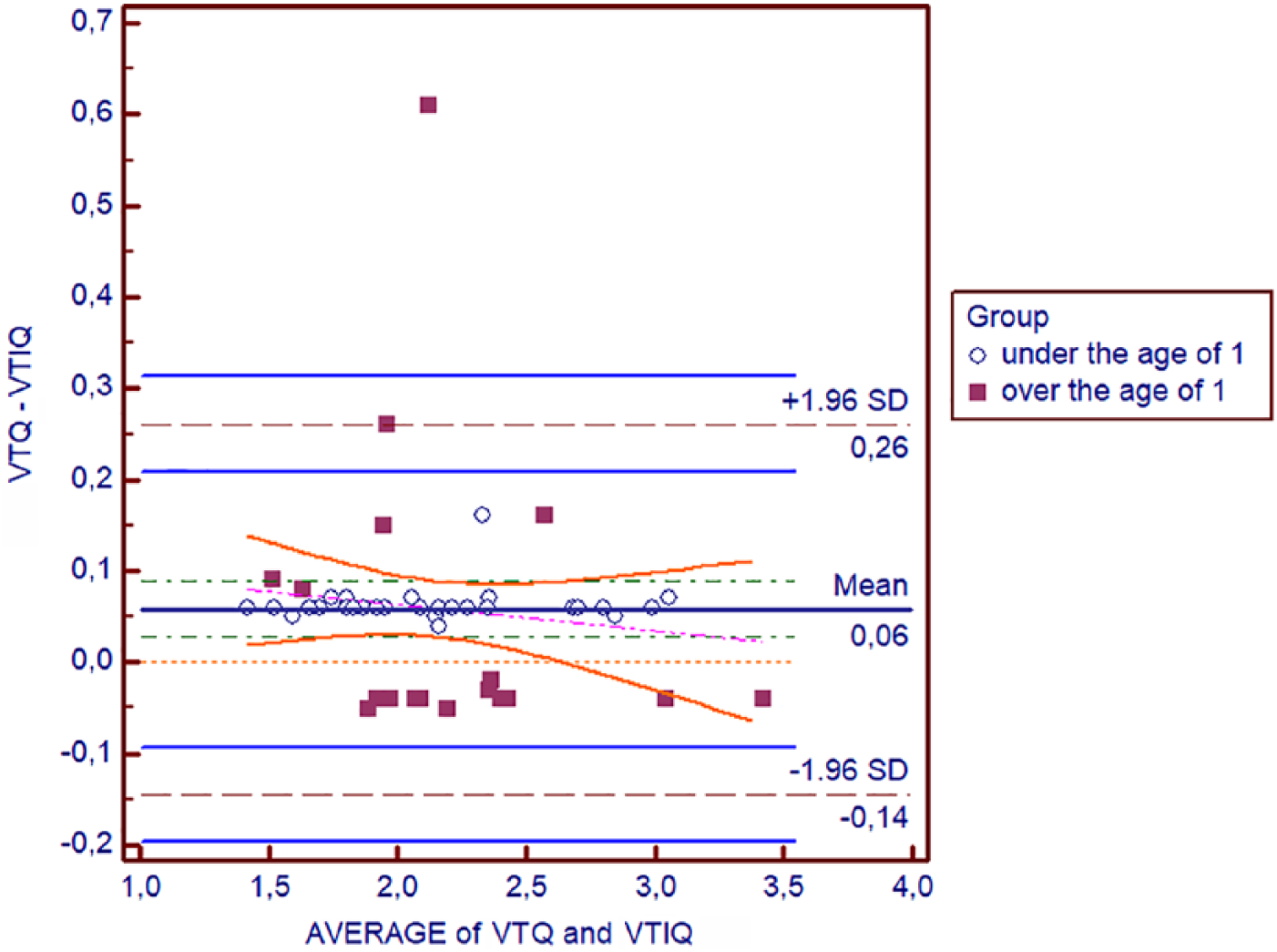
Bland-Altman statistics for the virtual touch quantification (VTQ) and virtual touch imaging quantification (VTIQ) for the groups over and under one year. This figure illustrates the data provided in Table 3.
Bland-Altman Distribution According to Graphical Localization
Although the VTQ-VTIQ methods in the intra-abdominal group showed similar results in the Bland-Altman graph, the difference between the VTQ-VTIQ methods in the inguinal canal group was striking. A significantly more scattered image emerged for the inguinal canal group. Thus, the inguinal canal group was more disperse than the intra-abdominal group. The VTIQ method produced superior results for the localization of the inguinal canal. Since the VTQ-VTIQ absolute value was used in the Bland-Altman chart, the VTIQ method is preferred for inguinal canal localization. These methods can be used interchangeably for intra-abdominal localization (Table 4, Figure 5).
Standard Deviation of the Results of the Bland-Altman Plots Based on Localization.
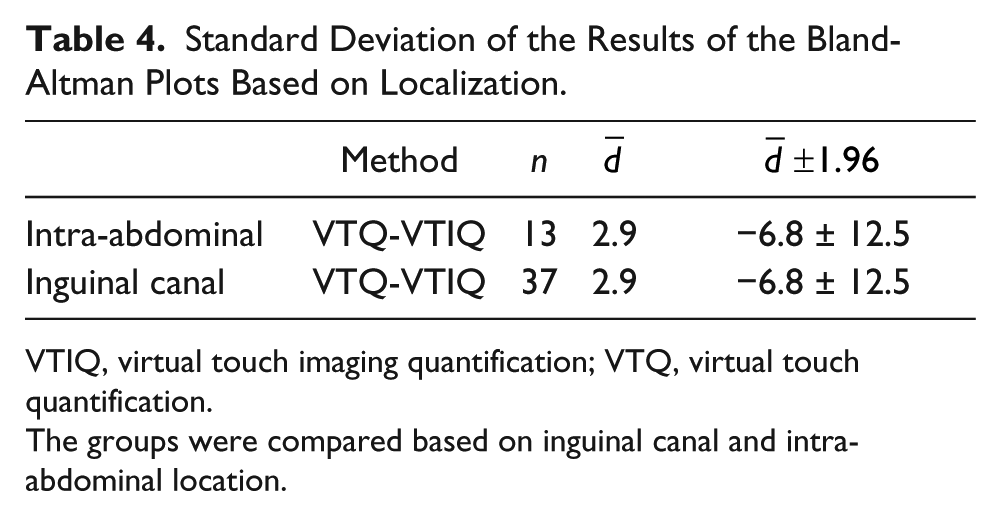
VTIQ, virtual touch imaging quantification; VTQ, virtual touch quantification.
The groups were compared based on inguinal canal and intra-abdominal location.
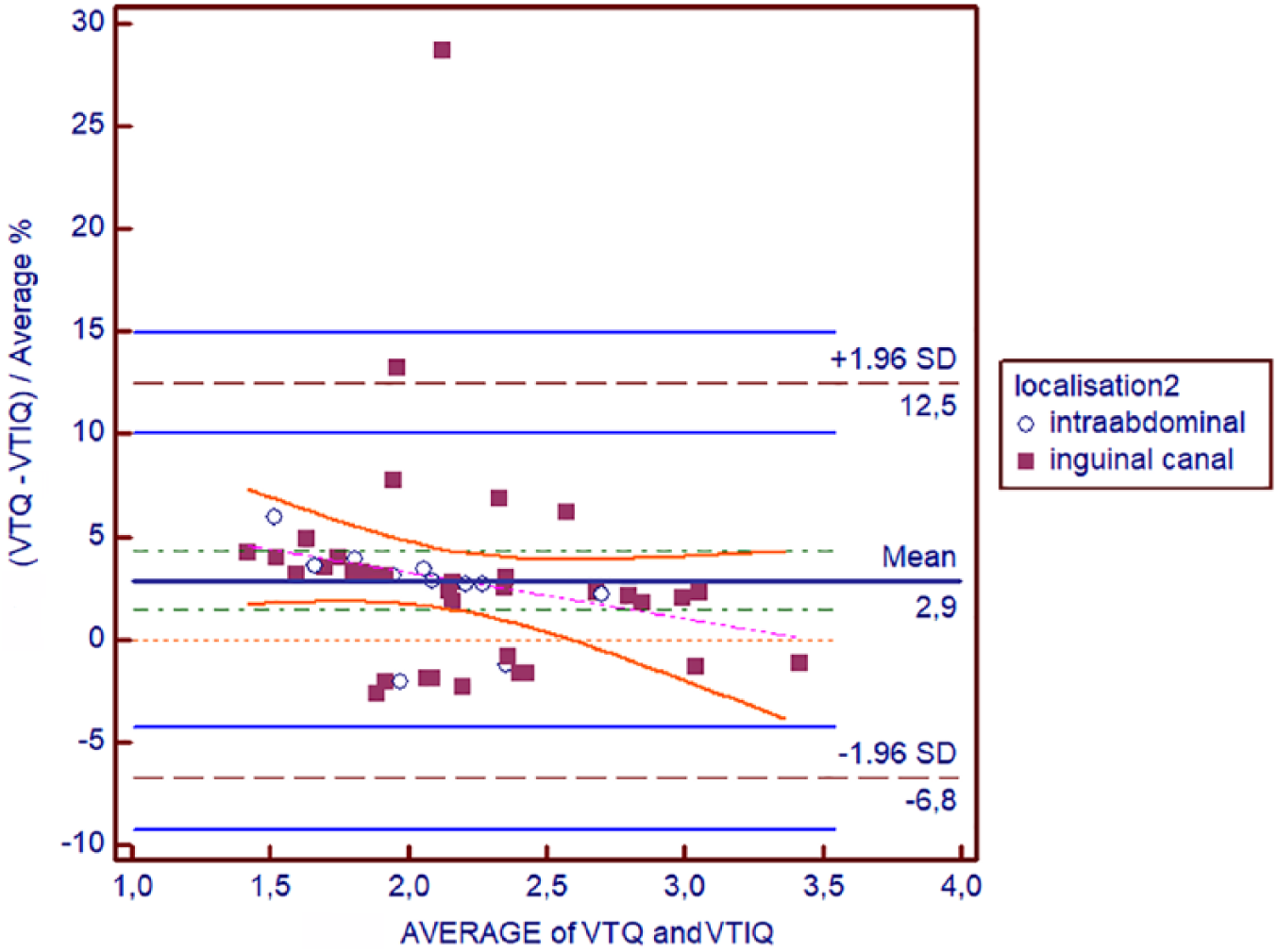
Bland-Altman statistics for the virtual touch quantification (VTQ) and virtual touch imaging quantification (VTIQ) for the groups based on inguinal canal and intra-abdominally located testes. This figure illustrates the data provided in Table 4.
Discussion
The clinical significance of VTQ and VTIQ in the available literature on the topic of undescended testicular tissue in pediatric patients has not been discussed previously. The aim of this study was to refine the different sonoelastographic techniques used for detecting pediatric undescended testicles based on location (intra-abdominal and inguinal) and age. It is accepted that higher levels of stiffness in undescended testes lead to sexual dysfunction. 3 In this case, understanding the pathophysiology of increased stiffness in the pediatric age group serves a specific key role. VTQ and VTIQ are two essential techniques for p-SWE imaging. In the present study, the VTIQ technique gave clearer results for inguinal canal localizations. For patients over the age of one, the results of the VTIQ technique were more obvious, based on the Bland-Altman plots.
According to the Bland-Altman plots, the results for inguinal canal localizations and patients over the age of one were also clearer. Changes in the testicular tissue begin in the embryonic stage and become more obvious over the age of one, which could explain why the findings relate to age—they demonstrate a tissue-stiffness relationship. Regarding sonographic physics, it is very difficult to observe or obtain clear results from deeper structures based on reflected echoes. Therefore, superficial tissue assessments (of the inguinal canal, for example) could easily explain the lower success rates of the intra-abdominal p-SWE results.
Limitations
There are some limitations to this study, such as the convenient sample of patients with threats to internal and external validity. In this study, the correlation of endocrinological functions with laboratory parameters and their relationship to tissue stiffness was not evaluated in the preoperative group of patients. The evaluation and effects of endocrinological therapy should be evaluated, and this may lead to further areas of research. 12
In the postpubertal period, tubular hyaline membrane thickening has been observed. 12 In some studies, the germinal cell pool was reduced by 40% in the first two years for infants with undescended testes.13,14 The undescended testicular tissue and the spermatic cord both had higher tissue stiffness than normal healthy volunteers. 12 Undescended testes with increased stiffness indicate a higher chance of future infertility or malignant transformation and require early fixation, especially for patients under the age of one. This issue should be investigated with larger cohort groups.
Conclusion
Both VTQ and VTIQ techniques provided a means to measure tissue stiffness in undescended pediatric age group patients. In addition, the p-SWE with VTIQ technique may be the most effective technique for detecting tissue stiffness located in the inguinal canal and for patients over the age of one. Furthermore, studies with larger cohort groups are essential to identify the appropriateness of the research in the pediatric age group.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.