
Abstract
The objective was to evaluate the distribution of the cross-sectional area (CSA) and flattening ratio (FR) of the median nerve (MN) in asymptomatic academic dentists using ultrasonography (US). Fifty academic dentists underwent US of the MN in transverse section at the pisiform bone level and the CSA (mm2) and FR were measured bilaterally. A CSA of <10 mm2 was considered normal. Paired t-test showed no statistical significance between either hand for CSA and FR (P> .05). Two independent t-tests showed significant statistical differences (P= .023) between males and females in the right dominant hand for CSA. Linear correlation analysis showed no significant correlation between CSA and FR for number of years of experience or number of working hours per day in either hand (P>.05). The CSA was abnormal in the right dominant hand in 20 (40%) of the subjects. These male academic dentists were at increased risk of having an enlarged MN without symptoms.
Introduction
Carpal tunnel syndrome (CTS) is the most common nerve entrapment syndrome, which mainly involves the compression of the median nerve (MN) as it passes through the carpal tunnel at the wrist. The frequency of CTS is 1-2% in the general population. 1 Patients usually complain of pain, numbness, and tingling in the hand, which occurs as a result of vascular and neural problems.
Female gender, pregnancy, obesity, rheumatoid arthritis, diabetes mellitus, thyroid diseases, and occupation type are the most common risk factors associated with the development of CTS.2–4 Dental personnel, including dentists, dental hygienists, and dental assistants, reportedly have a high prevalence of upper-extremity musculoskeletal disorders, and are at risk of developing CTS because they are more exposed to repetitive wrist work and work-related issues.5–9
Researchers have investigated several diagnostic techniques and criteria to confirm CTS. These include Tinel’s nerve percussion test, Phalen’s sign, wrist flexion test, reverse Phalen test, tourniquet test, tethered MN stress test, carpal compression test, and finally, nerve conduction test (NC), which is the gold standard examination. 10 A combination of clinical symptoms and electric conductance have been suggested as the most effective approach. 11 However, these methods offer only evaluation of peripheral nerve function and provide no data on the nerve morphology or the possible visible patho-morphology of the surrounding structures and tissues.10–11
Several articles have reported the usefulness of ultrasonography (US) with high-frequency linear array transducers in the diagnosis of CTS due to its wide availability, dynamic approach, mobility, rapid performance, noninvasiveness, and relatively low cost.12–22 However, the accuracy of US depends on the skill and precision of the sonographer. These findings are similar to the magnetic resonance imaging (MRI) findings, but MRI is less comfortable for the patient, more expensive, and less available than sonography. 14 Buchberger et al. 12 described the sonographic features of CTS, including the cross-sectional area (CSA) and flattening ratio (FR) of the MN as it passes through the carpal tunnel. Review of seven studies in the literature concluded that a reliable diagnosis could be made using the increase in the CSA of the MN at the level of the pisiform bone, although it was felt that sonography would probably not replace NC studies and would only serve as an additional test. 16 However, previous prospective studies15, 22 and a recent study by Azami et al. 23 showed that sonography was as accurate as NC studies in the diagnosis of CTS. The CSA at the entrance of the carpal tunnel seems to have the highest diagnostic sensitivity and specificity for CTS.12,14 In healthy controls, the mean±SD CSA of the MN at this level has been found to be between 7.0±1.0 mm2 and 10.2±2.5 mm2.14,17 Areas of 10.0-13.0 mm2 have been reported in patients with mild symptoms due to idiopathic CTS, 13.0-15.0 mm2 represented symptoms of moderate CTS, and areas >15.0 mm2 were found in patients with severe idiopathic CTS. 18
There appears to be no data available in the most relevant literature on ultrasonography using high-resolution imaging of the MN in academic dentists, despite the risk they run of developing CTS. The main aim of this study was to evaluate the CSA and FR of the MN and estimate the prevalence of an enlarged MN in academic dentists at our dentistry institute. Also, a correlation was sought between CSA, FR, the number of years of experience, and workload per day for academic dentists.
Subjects and Methods
Subjects
Sonographic evaluation of the MN was performed in 100 wrists of 50 (25 female and 25 male) randomly selected academic dentists working at a dentistry school during the period from September 2017 to April 2018. Study subjects were faculty members of that institution.
The volunteer dentists were initially asked by the research assistant to complete a questionnaire to collect the following information: sex, age, weight, height, years of working experience in dentistry, workload/day and presence of any symptoms such as pain, numbness or tingling in the hand or fingers. Inclusion criteria included healthy female and male academic dentists without symptoms of CTS, apart from fatigue due to workload. Volunteers who were pregnant; had a workload per day of less than 5 hours; work experience of less than 5 years; or who had any systemic disorders such as diabetes mellitus, connective tissue or musculoskeletal disorders, kidney or thyroid abnormalities that could affect peripheral nerves, were excluded. The Health Sciences Center Ethics Committee, Faculty of Medicine, Kuwait University, approved the study. A signed consent form was obtained from each volunteer prior to the study.
Sonographic Measurement
The sonographer was blinded to the dentist data, which was gathered through a questionnaire by the research assistant prior to the sonographic examination. Academic dentist volunteers were seated comfortably on a chair, and their forearm was rested on the examination table in a supinated position. The wrist was placed in neutral alignment and the fingers in normal resting position with mild flexion. A 6-15 MHz linear array transducer (GE VolusonTM E8 Model, GE Healthcare, Austria) was positioned perpendicular to the long axis of the forearm. Ultrasound was set at a custom preset for musculoskeletal sonography. A sufficient amount of gel was used to increase transmission of ultrasound and care was taken to keep the pressure on the skin to a minimum in order to avoid artificial deformation of the MN or the surrounding anatomic structures under examination (Figure 1).
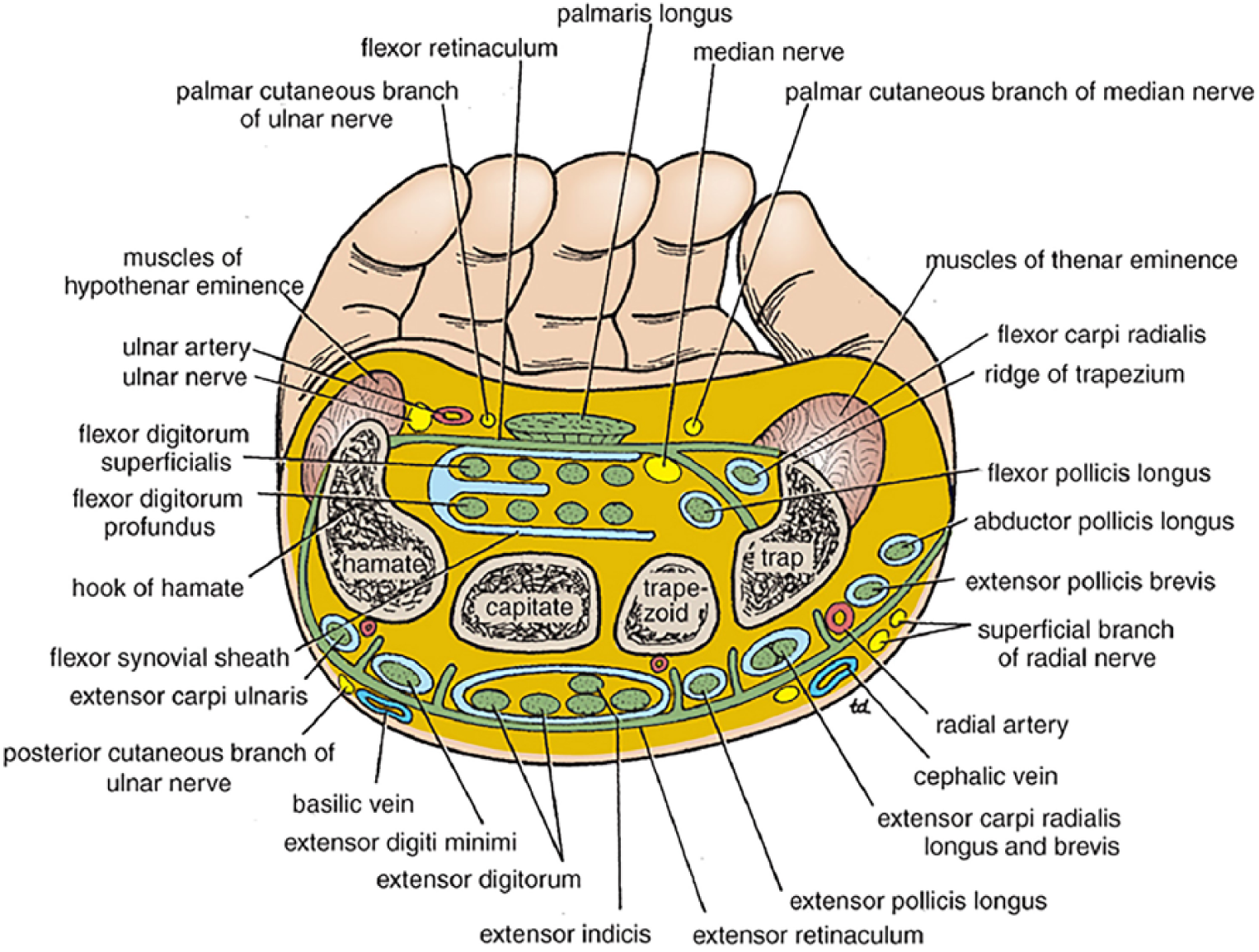
Cross-section diagram of the wrist at the carpal tunnel level showing the relation of the median nerve to the surrounding anatomical structures (permission from Wolters Kluwer Health/ Lippincott Williams & Wilkins 2008, Clinical Anatomy by Regions Book for Richard S. Snell, 8th Edition).
The following MN dimensions were measured bilaterally at the pisiform bone level of carpal tunnel in transverse section (Figure 2. A-D): CSA in square millimeters and longer diameter (LD) and shorter diameter (SD) in millimeters. The flattening ratio (FR) was calculated by the following formula: FR=LD/SD. All measurements were made using the highest frequency setting of the transducer and on “zoomed”-magnified images with electronic ellipse function and/or caliper selection tool of the nerve outline just within the hyperechoic epineurium. All images were saved on the machine’s hard drive memory. All measurements were taken three times for each median nerve. Mean values of CSA, SD, and LD were recorded. A CSA of <10 mm2 was considered normal; a CSA of 10.0-15.0 mm2 was considered mild to moderate CTS; and a CSA >15.0 mm2 was considered severe CTS.16–17 All sonographic measurements were performed by one sonographer with more than 15 years of experience in the field of musculoskeletal ultrasonographic imaging.
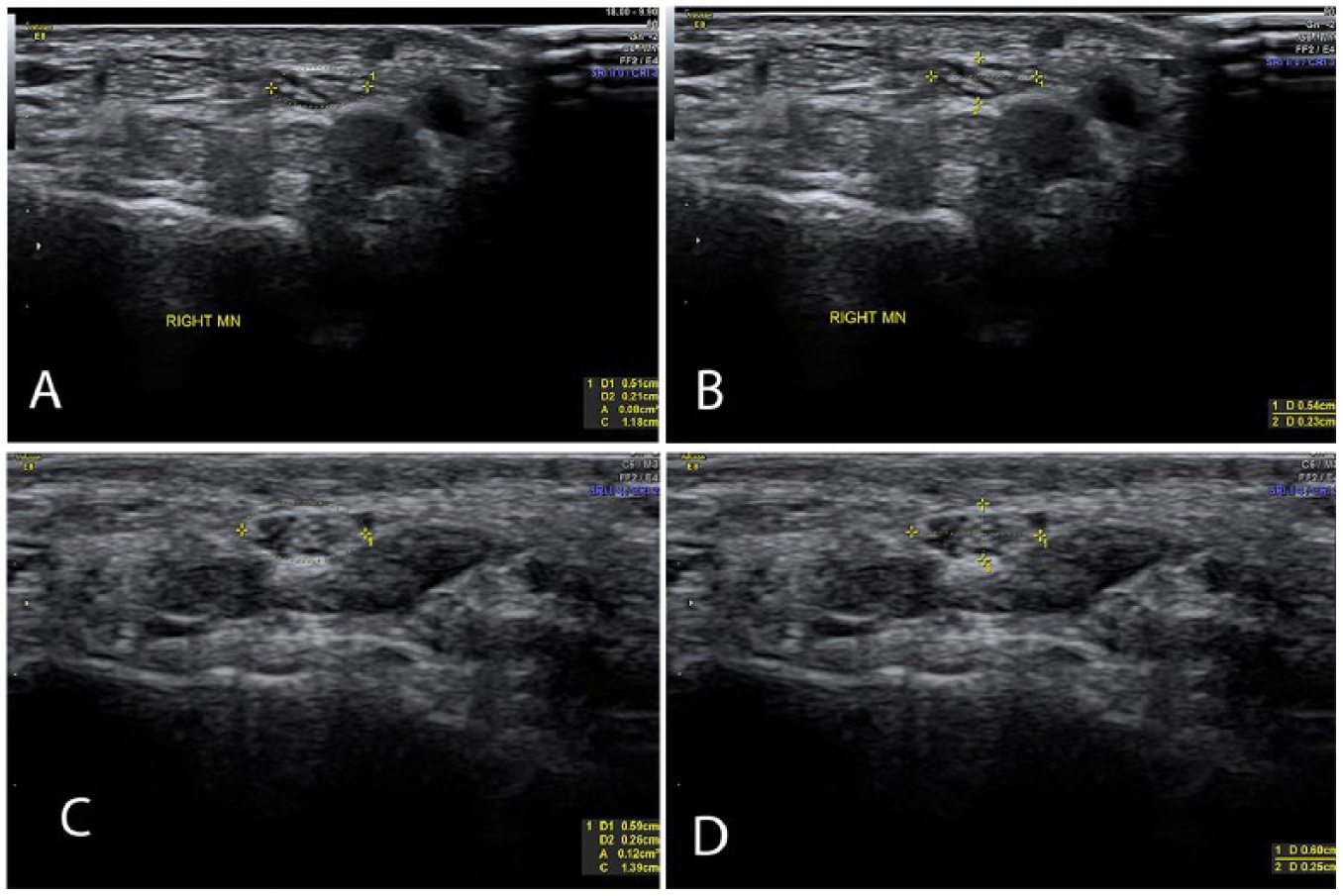
(A) Transverse sonographic images of a normal median nerve (outlined) at level of carpal tunnel in one of the male academic dentists in whom the CSA is 0.08 cm2 (8 mm2); (B) the longer diameter =0.54 cm (5.4 mm), the shorter diameter 0.23 cm (2.3 mm), and FR=5.4/2.3=2.3; (C) Transverse sonographic image of an abnormal median nerve (outlined) at level of carpal tunnel in another male academic dentist in whom the CSA is 0.12 cm2 (12 mm2); and (D) the longer diameter =0.60 cm (6 mm), the shorter diameter 0.25 cm (2.5 mm), and FR=6/2.5=2.4. (Note a continuous trace just within the hyperechoic boundary of the nerve).
Statistical Analysis
The data was entered into Excel 2013. All statistical analyses were carried out using Statistical Package for the Social Sciences (SPSS) version 25 for Windows (SPSS Inc., Chicago, IL, USA). Paired t-test was used to determine statistical significance in MN dimensions (CSA and FR) between the dominant and nondominant hand. Two independent t-tests were performed to test for gender variability between the dominant and nondominant hand for CSA and FR. Linear correlation analysis was used to determine the possible association between age, height, number of years of experience, and number of working hours per day for CSA and FR on the MN in the dominant and nondominant hands. A P value <0.05 was considered significant.
Results
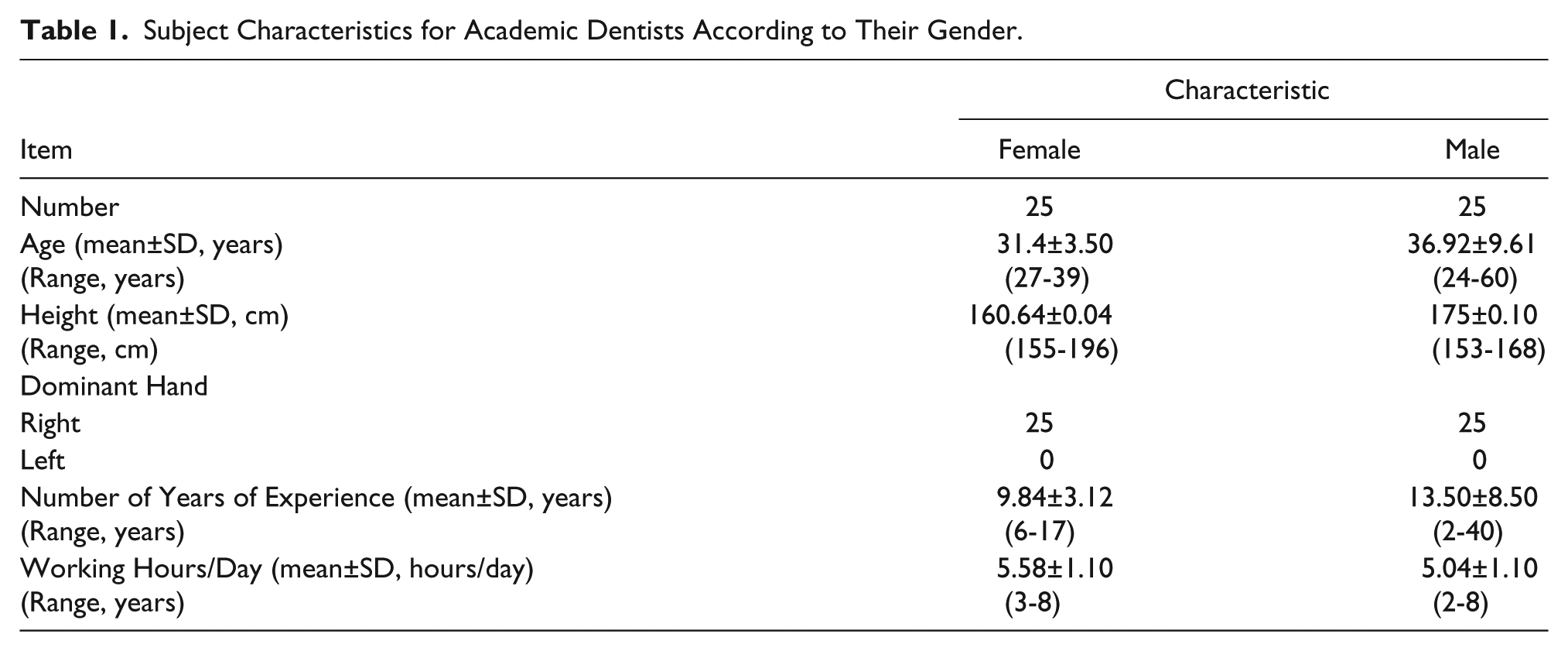
There were 25 females and 25 males. Their mean±SD (range) for age, height, number of years of experience, and working hours per day are summarized in Table 1. The right hand was dominant in all subjects. Related neurological symptoms, such as pain, tingling, and numbness, were absent in all subjects apart from discomfort in their dominant hand due to daily workload.
Subject Characteristics
The mean±SD (range) median nerve CSA and FR for the right dominant hand and left nondominant hand are summarized in Table 2. Paired t test between right dominant and left nondominant hand in each dentist showed no statistical significance for CSA and FR (P> .05). The two independent t tests showed a statistically significant difference (P=.023) of mean CSA measures between the right dominant hands of males (10.6±3.96 mm2) and females (8.6±1.60 mm2). This is demonstrated in Table 2. Linear correlation analysis showed no significant correlation between CSA and FR for right dominant hand or left nondominant hand for age, height, number of years of experience, or number of working hours per day.
Mean±SD (Range) for the Median Nerve Cross-sectional Area, Longer Diameter, Shorter Diameter, and Flattening Ratio for Both Hands for All Academic Dentists.
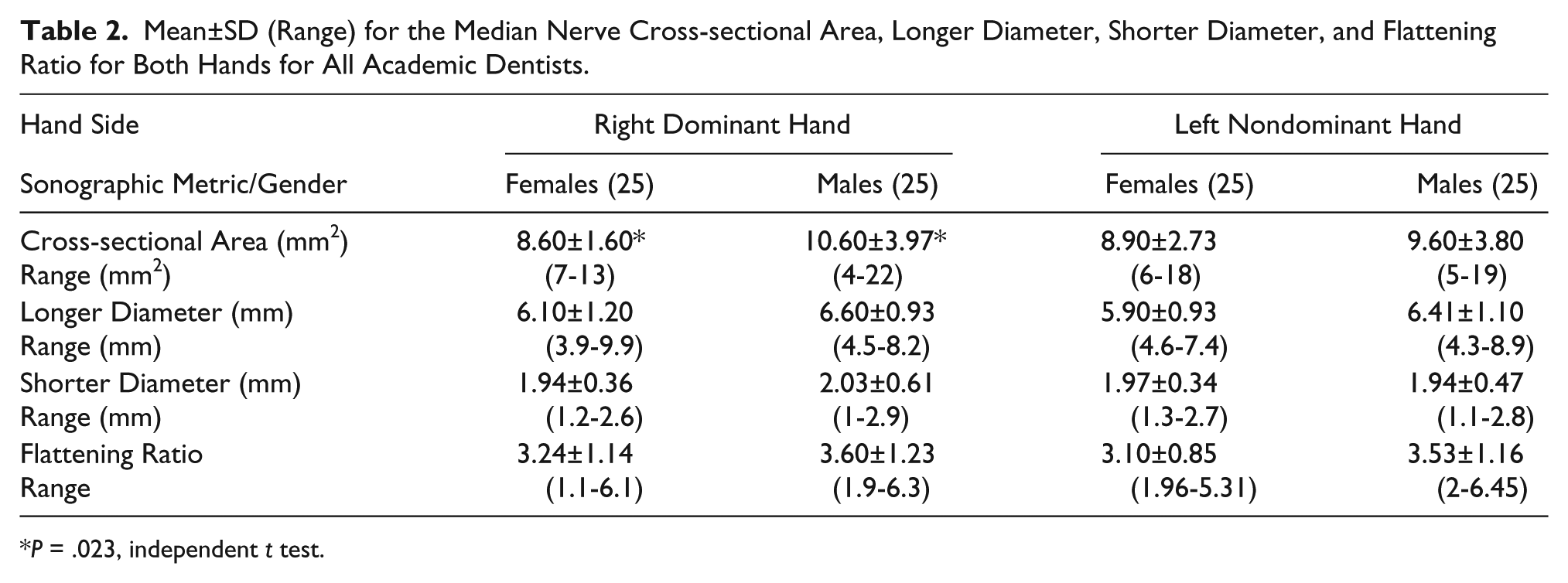
P = .023, independent t test.
The CSA was abnormal (>10 mm2) in the right dominant hand in 20 (40%) of the subjects. Interestingly, these results were comparable to the left nondominant hand, for which CSA was abnormal in 19 (38%) of the subjects. The CSA of individuals was considered abnormal, in roughly the same amount, in dominant and nondominant hands. These abnormalities were consistent in different individuals. The number of hands (%) and the degree of CTS severity according to CSA values are summarized in Table 3.
The Number of Hands and Percentage (%) According to Their Level of Cross-sectional Area, Degree of Carpal Tunnel Syndrome, and Gender in Right Dominant and Left Nondominant Hands in All Academic Dentists.
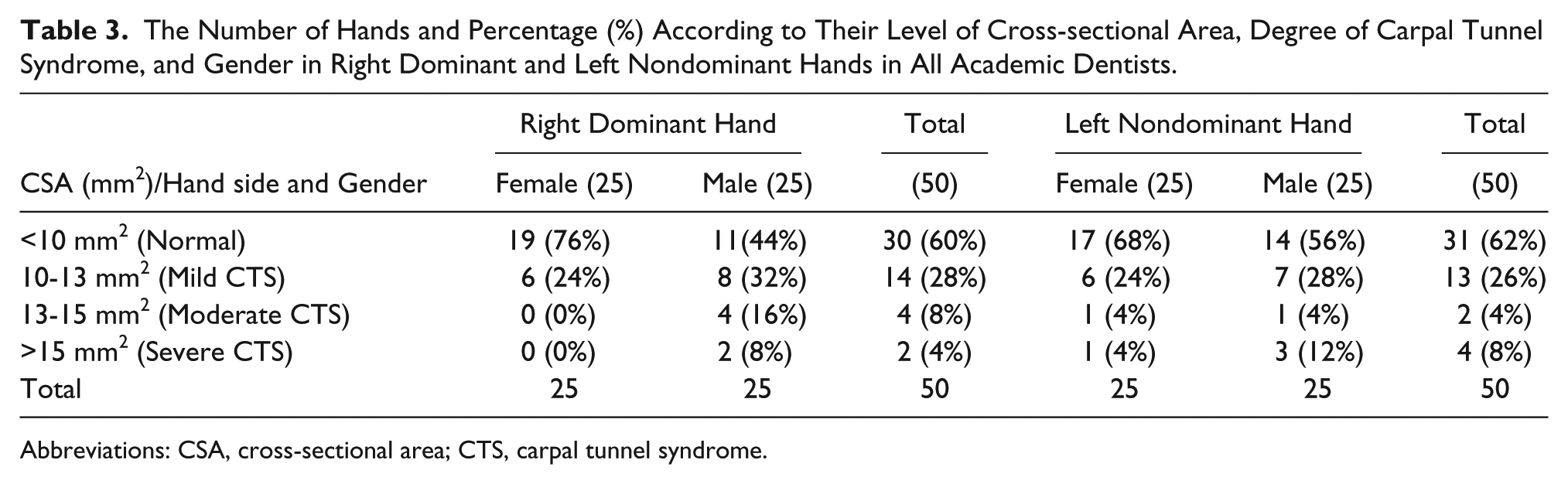
Abbreviations: CSA, cross-sectional area; CTS, carpal tunnel syndrome.
Discussion
The present study was initiated to evaluate the MN, CSA, and FR and to estimate the prevalence of an enlarged MN in academic dental practitioners at a dentistry institute. Also, correlations were sought between the CSA and FR of the MN and the number of years of experience and working load per day for all volunteers, as there was no data available in the literature on the use of high-resolution US of the median nerve in academic dentists.
Dentists are at risk of developing CTS symptoms and other musculoskeletal disorders because they work in a field that requires fine technical hand skills, in a confined area in patients’ oral cavity, and prolonged use of vibratory instruments held tightly in a pinch-like grip.24–25
In the present study, high-resolution US was used because of its availability, dynamic approach, mobility, rapid performance, noninvasiveness, relatively low cost, and reproduciblity.12, 20 One sonographer with more than 15 years of experience performed the sonographic measurement. Also, the mean values of three measurements for each MN – CSA, SD, and LD – were taken to increase the intra-rater reliability and confirm that the sonographer had consistent measures.
The CSA of the median nerve was used in our study as Buchberger et al. described, 12 which relies on the increased CSA of the median nerve at the level of the carpal tunnel for reliable diagnosis of CTS. However, NC testing was not performed in this study because it was not available. This work relied upon the fact that previous prospective studies15, 22 as well as the most recent study by Azani et al. 23 showed that US was as accurate as NC studies in the diagnosis of CTS. In addition, this research relied on CSA dimensions as described by others using high-resolution US, where a CSA of <10 mm2 was considered normal and a CSA of >10 mm2 was considered abnormal, indicating different degrees of severity of CTS.14, 17–18
The results in all 50 volunteer academic dentists showed that 40% and 38% had CSA >10 mm2 in the dominant right hand and nondominant left hand, respectively (Table 3). The CSA of individuals was considered abnormal in roughly the same amount of dominant and nondominant hands. These abnormalities were consistent in different individuals. If the CSA of the MN is enlarged in the left and right hands of the same individuals, then it is possible that the CSA values in these individuals are larger than those considered typical or healthy.
The abnormal percentage in this study was much lower than the results that were observed in the study by Prasad et al., 9 in which the prevalence was 86%. However, the present study results were higher than those found by Borhan Haghighi et al., 8 in which the prevalence was 18.5%. This could be attributed to a small sample size in this group in comparison to the sample size used in the two studies just cited. In the study by Prasad et al. 9 the higher prevalence is attributed to the fact that dental practitioners in their study group treated more patients with less resting time and without properly following ergonomic guidelines. However, in the present study and in the study by Borhan Haghighi et al. 8 dentist practitioners are more aware about the risk factors arising from the profession and follow prophylactic prevention.
In addition, there was a statistical difference between genders: academic male dentists possess a higher CSA and were at a higher risk than females secondary to age, height, and number of years of experience. This gender difference was attributed to the finding in some studies that normal values might be different in men and women; or it may be that males just typically have a larger MN CSA compared to females. 26 Based on the findings in this study – that there was no correlation between the years of experience and the CSA or FR of the MN – it seems as though none of the attributes of age, height, and number of years of experience lead to differences in CSA or FR. Therefore, these findings were in line with some recent reports on the issue, 27 which claim that the association between dentist work and CTS (marked by compression of the MN and, thus, probable change in its CSA or even more likely in its FR) is, at the very least, controversial. 28
Enlargement of the MN without symptoms in some individuals may indicate that they simply have larger CSA values than those considered typical or healthy. There are some research studies that talk about enlarged nerves in asymptomatic individuals, 17 preclinical CTS, 29 and false-positive findings using sonography. 30 It may be that US is not an appropriate test for these individuals, as there may be false-positive tests of CTS in this sample.
The present study was limited by the small sample size and similar working conditions of the many volunteer dentists who were included. Also, the volunteer academic dentists did not represent the general dentistry population. Another limitation was that the measurement technique used to measure the nerve was the electronic ellipse function, which could have overestimated or underestimated the CSA for nerves that were not ovoid in shape. The use of direct trace around the inner hyperechoic border of the nerve would create more precise measures.
A long-term prospective study with a larger sample size, using high resolution US, MRI, and NC, is needed to explore the relationship between age, gender, the number of years of experience, and the number of working hours/day with the CSA and FR in dental practitioners and their associates. This study will have a clinical value in early recognition of CTS and lead to more effective management. In addition, similar studies could be carried out on high-risk professionals such as surgeons, radiographers, and sonographers, coupled with education regarding ergonomic risk factors, as an effective preventive measure.
Conclusion
Male academic dentists may have a higher CSA of the MN and may be at increased risk of developing CTS without apparent symptoms than academic female dentists. Early recognition of an enlarged CSA of the MN by US among dentists can lead to more effective management and better education regarding ergonomic risk factors, which can be an effective preventive measure.
Footnotes
Acknowledgements
The authors would like to thank the College of Dentistry-Health Sciences Center, Kuwait University for their help and support. Sincere thanks go to the academic dental practitioners for their participation in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.