
Abstract
It is important to include splenic implants in the differential diagnosis of patients with a history of splenic trauma. Autotransplanted splenic implants may have a sonographic appearance similar to that of pathologies such as lymphadenopathy or carcinomatosis.
This is the first known case to discuss a pregnant patient with a history of autologous autotransplanted splenic tissue, which was discovered on sonography and confirmed during the patient’s cesearean section.
Introduction
In abdominal trauma, the majority of splenic injuries are managed with a non-operative approach. However, those requiring emergent intervention may undergo a spleen-conserving technique such as a partial splenectomy or splenorrhapy. Because the spleen plays a crucial role in the immunologic function of the body, autologous autotransplantation of the spleen is a surgical option for maintaining viable splenic tissue. With autotransplantation, portions of the spleen can be implanted into the greater omentum. In patients who have a history of abdominal trauma and splenic surgery, reimplantation of the splenic tissue may not be known to subsequent care providers. The following case describes a pregnant patient with a remote history of abdominal trauma, for whom sonography identified masses in the omentum. This case highlights the importance of considering splenic implants or autotransplanted splenic implants in the differential diagnoses of incidental abdominal masses imaged during pregnancy.
Case Report
A 34-year-old G2P1001 presented to the labor and delivery unit at 29 weeks gestation with sudden onset of cough and shortness of breath. On initial presentation, she had no evidence of fever but had tachycardia to 107 beats per minute, a respiratory rate of 28, and an oxygen saturation of 85%. A radiograph showed bilateral alveolar infiltrates and an area that was a concern for hemorrhage. Because of the acute onset and continued decompensation, a pulmonary embolus was suspected. A computed tomogram (CT) of the chest was performed and this documented bilateral infiltrates consistent with pneumonia, without evidence of pulmonary embolus or hemorrhage. The patient was admitted and treated for pneumonia with the antibiotics ceftriaxone and azithromycin.
When reviewing the patient’s past medical history, her providers were informed that she had a history of a motor vehicle accident that took place 15 years prior to the current pregnancy. This hospitalization required multiple abdominal surgeries, including splenectomy, small bowel resection complicated by short gut syndrome, and a craniectomy that resulted in chronic headaches requiring prolonged benzodiazepine and narcotic use. Because the surgeries had occurred 15 years previously, records of her surgical history were initially unavailable from the outside institution where the procedures had been performed. She also had a history of alcohol abuse and chronic pancreatitis prior to her pregnancy.
During her pregnancy, she had poor weight gain, with an admission weight of 95 pounds and a BMI of 17. During the hospitalization for pneumonia, the patient had observed hematemesis; therefore, based on her history of alcohol abuse, an analysis of her complete blood counts (CBC) and liver enzymes was completed. The CBC demonstrated anemia with a hemoglobin of 9.8 g/dL and normal liver enzyme levels. An abdominal sonogram was ordered due to concern for liver cirrhosis. A Philips Epic Logic 7 ultrasound system with a C 5-1 MHz curved array transducer was utilized. The sonogram revealed an absent spleen and coarse-appearing liver with a heterogeneous echotexture, consistent with cirrhosis. Multiple solid masses were noted superior to the umbilicus with the largest measuring 35 x 28 x 16 mm (Figure 1.A). The masses appeared to have a central hilum and color Doppler imaging showed internal vascularity (Figure 1.B). Given the clinical picture and the sonographic findings, the differential diagnoses included lymphadenopathy, neoplasm, omental infarction, omental hematoma, and fibrotic tuberculosis peritonitis.
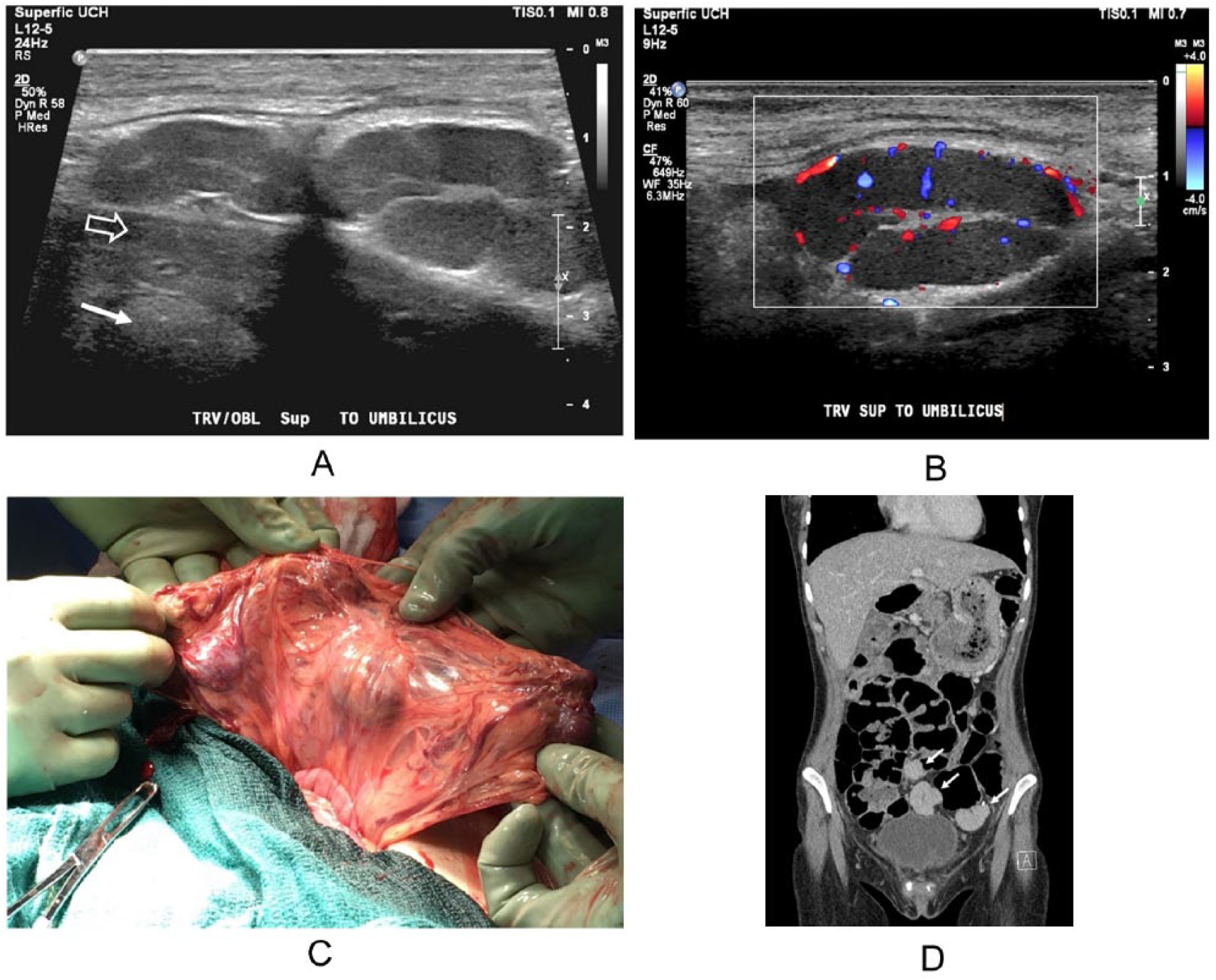
(A) Transverse sonographic image of the autotransplanted splenic implants sitting just anterior to the uterine wall (open arrow) and placenta (closed arrow). (B) Transverse sonographic image demonstrating color Doppler flow of the autotransplanted splenic implants. (C) The autotransplanted splenic implants seen during the cesarean section. (D) A CT image, post-cesarean section, showing three of the autotransplanted splenic implants (white arrows).
Several hours following the sonogram of her liver, the patient started having severe and painful contractions indicative of preterm labor, a common complication from pneumonia in pregnancy. Fetal assessment with non-stress testing demonstrated heart-rate decelerations and minimal variability. Despite conservative measures with hydration and oxygen therapy, the heart rate did not improve and indicated fetal acidosis, which prompted the decision to move toward delivery by cesarean section. During the cesarean section, multiple round, solid, dark masses were identified in the omentum, consistent with the sonographic findings (Figure 1.C). A general surgeon was consulted during the procedure to see if the masses required biopsy or excision; however, the implants were identified as splenic tissue. This was later confirmed after obtaining the operative report from 2002, which showed that the patient had undergone a splenic autotransplantation with implants placed in the omentum.
Postoperatively, the patient continued to require oxygen, with increased need for supplemental therapy on postoperative day (POD) 2. A CT demonstrated pulmonary edema and a pulmonary embolus. She was treated with Lasix and anticoagulation, which improved her functional status. She was discharged to home on POD 7.
Three days after discharge, the patient presented to the emergency department for abdominal pain at the area of her cesarean section incision. A CT scan was ordered for evaluation of an intra-abdominal abscess, and it revealed a post-operative cesarean scar hematoma. The splenic implants were also identified (Figure 1.D). She was discharged from the emergency department after the pain was managed with morphine, and the remainder of her post-operative course was uncomplicated.
Discussion
The spleen is an intraperitoneal organ located in the left upper quadrant. The length of the spleen is typically between 9 and 12 cm, but it may vary with body habitus and age. Ectopic splenic tissue may also be found in the abdomen or thorax, 1 and when this occurs, the spleen is classified as either an accessory spleen or splenosis. Accessory spleens are formed during embryonic development and are typically found in the splenic hilum but they can also be found rarely in the pelvis. Splenosis can be secondary to trauma or to a surgical splenectomy with autologous autoimplantation. 2 The patient in this case was one of several individuals who had had a splenic autologous autotransplantion performed in the same hospital. 3 The most frequent technique of splenic autologous autotransplantation in humans consists of implanting sections of viable splenic tissue into the greater omentum. 4 It has been shown that grafting the spleen into the omentum results in better splenic regeneration and subsequent immunologic function. 4 Newer methods have been described that use a single implant in the omentum to reduce the risk of implant torsion, ischemia, or abscess formation. 5 The goal of splenic autotransplantation, regardless of surgical technique, is to preserve the immunologic role of the spleen. 4 Splenic autotransplantation may occasionally be encountered in clinical practice, where clinicians and radiologists often find the diagnosis of this condition challenging. 6 Abdominal sonography and other imaging modalities such as CT and magnetic resonance imaging (MRI) do not provide a confirmatory diagnosis of abdominal splenosis. 7 Splenic tissue is best evaluated with nuclear scintigraphy using Technetium-99m heat damaged erythrocytes or Indium 111-labeled platelets. 8 Although this is the best modality to confirm splenosis, it is not a viable option in pregnancy because of the radiation exposure. Ferumoxide MRI is another tool that can be used in diagnosing splenosis, as this is a superparamagnetic MRI contrast medium consisting of small molecules of iron oxide that have an affinity for reticuloendothelial tissues. In this testing, there is a signal loss on T2 sequences of MRI imaging when looking at the nodules. 9 The US Food and Drug Administration lists this contrast agent as Pregnancy Category C because Ferumoxide has not been adequately studied in pregnancy, and thus limits the ability to use this modality for diagnosing splenic tissue. 10
There is little literature on the sonographic appearance of autologous autotransplanted splenic implants. Sonographic findings are not specific, but may show round or oval soft-tissue masses within the abdomen. 11 Accessory splenic tissue, splenosis, and autotransplanted splenic tissue have the same sonographic echotexture as a native spleen. They appear as a homogenenous echotexture and are slightly more echogenic than the liver and kidney. 1 Contrast-enhanced sonography is also useful in differentiating intraabdominal splenic tissue from other masses. A “zebra pattern” may be seen in the parenchymal phase and should display persistent late-phase enhancement. 1 Although ultrasound contrast agents may give some insight into the diagnosis, these agents are currently not approved in pregnancy as their safety is unknown. 12
The mean size of accessory spleens has been shown to be 14.7 mm in diameter. 13 The size of autologous autotransplanted splenic tissue is more variable than that of accessory spleens and is based on the surgical technique. Due to splenic shrinkage of up to 50% after autotransplantation, surgically implanted splenic tissue has been reported to vary in size from 1 x 1 x 0.2 cm to large slices of 3 x 4 x 12 cm. 14
When an intra-abdominal mass is incidentally identified, the diagnosis may be difficult due to a broad range of differential diagnoses. Many of the diagnoses include tumors, infections, and malignancy. Masses in the abdomen may be confused with numerous conditions such as metastatic disease, abdominal lymphoma, carcinomatosis, multifocal endometriosis or reactive adenopathy. 8 The autotransplanted splenic implants described in this case closely resembled lymphadenopathy due to the appearance of a central hilum.
This case is unique because of an inability to use other imaging modalities to assess the masses due to safety concerns in pregnancy. Additionally, the location of implants in the omentum would make biopsy of the masses difficult secondary to an obstructing uterus and fetus late in the second and third trimesters. Due to the risk of malignancy, previous authors have recommended the excision of all incidental adnexal masses during cesarean delivery, particularly those larger than 5 cm. 15 Because splenic implants are not a pathologic process and are potentially beneficial to the patient’s immunologic function, it is important to recognize and consider implants in the differential diagnosis of abdominal masses with sonography. The hallmark in correctly diagnosing ectopic splenic tissue is awareness of its existence and a history of splenic injury or surgery. Furthermore, when asymptomatic splenic nodules are encountered, excision is not recommended. 16
The incidental finding of splenosis after splenic trauma and accessory spleens is well-described. It appears that this is the first published case of autologous autotransplanted splenic tissue discovered incidentally in a pregnant patient.
Conclusion
This unique case highlights the importance of including accessory spleens or autotransplanted splenic implants in the differential diagnosis when sonography identifies abdominal masses, especially in patients with a history of abdominal surgery for trauma. Accessory spleens or autotransplanted splenic implants should also be a consideration when incidental adnexal or abdominal masses are found during cesarean section. Sonography, among other imaging modalities, can help further characterize abdominal or adnexal masses; however, a patient history of splenic trauma is key to identifying ectopic splenic tissue.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.