
Abstract
Musculoskeletal sonography is being widely used for evaluation of structures within the carpal tunnel. While some anatomical variants, such as bifurcated median nerves and persistent median arteries, have been well documented, limited literature describes the sonographic appearance of aberrant muscle bellies within the carpal tunnel. Multiple examples of the sonographic appearance of flexor digitorum superficialis and lumbrical muscle bellies extending into the carpal tunnel are provided. Techniques for static image acquisition and analysis are discussed, and the use of dynamic imaging to confirm which specific muscle belly is involved is described. Knowledge of the potential presence of muscle bellies in these images and ability to identify these structures is vital to avoid misclassification or misdiagnosis as abnormal pathology. The case examples are situated among current published evidence regarding how such anomalies may be related to the development of pathologies, such as carpal tunnel syndrome.
Musculoskeletal sonographic imaging is commonly used to evaluate the carpal tunnel and diagnose pathologies in this region, such as carpal tunnel syndrome, a condition caused by compression of the median nerve at the wrist. The carpal tunnel is a space created at the wrist by the transverse carpal ligament and the two rows of carpal bones, with nine tendons and the median nerve passing through it. The transverse carpal ligament, also referred to as the flexor retinaculum, attaches to the pisiform and the hook of hamate on the medial (i.e., ulnar) side and to the scaphoid and the trapezium on the lateral (i.e., radial) side of the wrist. Immediately deep to the flexor retinaculum is the median nerve, which sits superficial to nine flexor tendons. These tendons include a row of four flexor digitorum superficialis tendons and a deeper row of four flexor digitorum profundus tendons, one of each going to the index, middle, ring, and small fingers. A ninth tendon, the flexor pollicis longus, passes through the carpal tunnel superficially and on the lateral (i.e., radial) side as it travels distally to attach to the thumb. The sonographic appearance of the typical carpal tunnel and its structures is provided in Figure 1.
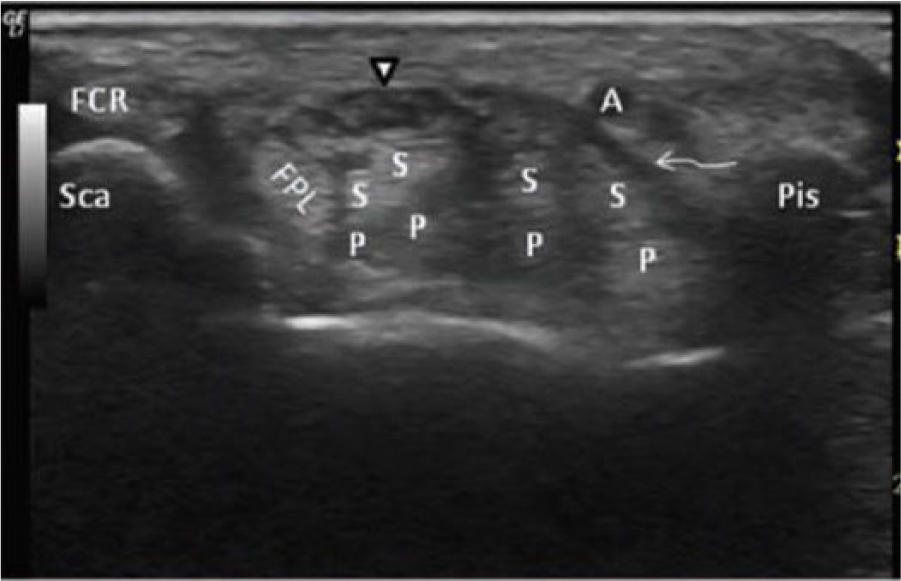
This image demonstrates the sonographic evaluation of the carpal tunnel at the level of the scaphoid (Sca) and pisiform (Pis) in the transverse view. The median nerve (arrowhead) is positioned posterior to the transverse carpal ligament (curved arrow) and anterior to the flexor pollicis longus (FPL), flexor digitorum superficialis (S), and profundus (P) tendons. The flexor carpi radialis (FCR) tendon lies lateral and the ulnar artery (A) is positioned medially in Guyon’s canal. (Image reprinted courtesy of the Journal of Diagnostic Medical Sonography from Evans et al. 33 )
Two types of anatomic variations within the carpal tunnel are commonly discussed in the literature: bifurcated median nerves and persistent median arteries. Under typical circumstances, the median nerve passes through the carpal tunnel as a single nerve and bifurcates in the palm, becoming individual sensory and motor nerve branches. A bifurcated median nerve, commonly referred to as a bifid nerve, indicates that the nerve divides into two separate portions proximal to the carpal tunnel.1–4 A persistent median artery is an embryological remnant that results in a median artery traveling down the central, anterior forearm from the elbow into the carpal tunnel, in contrast to the typical presentation that is without the presence of a large artery in this region.1–4 It has been reported that bifid median nerves and persistent median arteries exist in approximately 8.6% to 9.4% and 1.2% to 23% of the population, respectively.2,5,6
An anatomical variant that has been less documented is the presence of aberrant muscle bellies within the carpal tunnel. Typically, only tendons and the median nerve will appear within a cross-sectional image of the carpal tunnel when evaluating the hand at rest; however, in some individuals, echogenic muscle bellies will be present in the tunnel along with these other structures. These aberrant structures most often present as elongated, hypertrophic bellies of normal muscles that extend into the carpal tunnel, primarily the lumbrical muscles or the flexor digitorum superficialis of the index finger. 6 In rare cases, these aberrant structures are not just elongated, hypertrophic muscles but extra, anomalous muscles that have developed in addition to those normally present.7,8
Knowledge of the presence of aberrant muscle bellies and the ability to identify these structures when conducting sonographic imaging is vital to avoid misclassification or misdiagnosis as abnormal pathology. Furthermore, understanding the relationship of these extended muscle bellies to their surrounding structures, especially the median nerve, is important as a means to evaluate their association with pathologies, such as acute median nerve entrapment and carpal tunnel syndrome. The aim of this case study report is to exemplify the appearance of aberrant muscle bellies within the carpal tunnel using musculoskeletal sonography so that they can be easily recognized in clinical practice. Multiple examples of the sonographic appearance of the flexor digitorum superficialis and lumbrical muscle bellies extending into the carpal tunnel are provided, techniques for static image acquisition and analysis are discussed, and the use of dynamic imaging to confirm which specific muscle belly is involved is described. The case examples are situated among current published evidence regarding how such anomalies may be related to the development of pathologies, such as carpal tunnel syndrome.
Case Report
Cases presented here were identified from among individuals enrolled in a multicohort, longitudinal study investigating morphological changes of the median nerve in healthy participants using musculoskeletal sonography. The study was approved by the university’s institutional review board, and all participants provided informed consent. The bilateral upper extremities of all participants in the study were evaluated using an established protocol investigating the median nerve in the forearm and carpal tunnel. 9 Participants were seated facing the examiner with their supinated forearm and neutrally positioned wrist resting on a table. The sonographic evaluation was performed by either a registered musculoskeletal sonographer (RMSKS) or a registered diagnostic medical sonographer (RDMS) using a Logiq-e sonography machine with a 12-MHz linear array transducer (GE Healthcare, Milwaukee, Wisconsin). Spatial compounding (i.e., cross-beam technology) was used and gain was adjusted to optimize image quality for each individual.
A comprehensive evaluation of the anterior forearm and wrist was conducted for purposes of the study; however, only those portions of the imaging protocol relevant to this case report are described here. First, static images of the carpal tunnel in the transverse plane were acquired at the level of the pisiform while the participant’s hand was held in a relaxed position. Once placed in the correct anatomic location, the transducer was adjusted to obtain an angle of insonation that optimized the median nerve and as many other structures within the carpal tunnel as possible. Next, dynamic cine clips were obtained while participants made a fist. Beginning with the fingers fully extended, participants were asked to slowly flex their fingers until the fingertips touched the palm to make a relaxed fist (i.e., participants were asked not to squeeze the fingers together). After holding the relaxed fist for one second, the participants then slowly extended the fingers, returning to a relaxed open-hand position.
During image analysis, two types of elongated, hypertrophic aberrant muscles in the carpal tunnel were identified in the static images, long flexor muscle bellies and lumbrical muscle bellies. Long flexor muscle bellies consist of either the flexor digitorum superficialis or flexor digitorum profundus tendons of the fingers or the flexor pollicis longus of the thumb. Usually, these muscles are found in the proximal three-fourths of the volar forearm, with the musculotendinous junction occurring prior to the entrance of the carpal tunnel. Similarly, lumbrical muscles are usually located distal to the carpal tunnel. Lumbrical muscles, one for each finger, are intrinsic muscles of the hand that originate from one of the four flexor digitorum profundus tendons and insert on the dorsal hood of the associated finger. Because of their position, lumbrical muscles flex the metacarpophalangeal joints (i.e., knuckles) and extend interphalangeal joints (i.e., finger joints) at the same time (Figure 2). These muscles allow for fine motor activity and precise movements of individual fingers that otherwise could not as easily occur due to the shared muscle fibers of the long flexor and extensor muscles of the digits. When the hand is held in a relaxed position, it is not typical to observe muscle bellies of either the long flexor or lumbrical muscles in an image of the carpal tunnel at the level of the pisiform.

A hand in the “lumbrical plus” position due to active engagement of the lumbrical muscles of the fingers, which lead to simultaneous flexion of the metacarpophalangeal joints (i.e., knuckles) and extension of the interphalangeal joints (i.e., fingers).
While not typical, when aberrant muscle bellies are identified or suspected in a resting carpal tunnel image, dynamic cine clips can be used to confirm the structures as a muscle and to identify the specific muscle(s) involved. As the digits of the hand are flexed to make a fist, the long flexor muscles contract (i.e., shorten), causing the muscle bellies and musculotendinous junction to retract proximally toward the muscle origin at the medial elbow. Conversely, when the digits of the hand are extended, the long flexor muscles relax and become elongated, causing the bellies of the digital flexor tendons to travel distally. In some cases, the flexor muscle belly is so large that it enters the carpal tunnel while the hand is relaxed yet will still exit the carpal tunnel when the fingers are flexed. This movement into and out of the tunnel can be visualized with dynamic imaging. It should also be noted that active hyperextension of the fingers will place a stretch on the flexor tendons, pulling those tendons and the musculotendinous junction distally. This hyperextension of the fingers may increase the chance of visualizing flexor muscle bellies within the carpal tunnel that may not be seen when the fingers are in a relaxed position.
Similar to the flexors, lumbrical muscles typically reside fully within the palm and do not appear within the carpal tunnel while the hand is at rest. As the fingers are flexed, the lumbrical muscles are pulled proximally due to their attachment to the proximally sliding flexor tendons. Eventually, when the fingers become fully flexed, the lumbricals will enter the distal carpal tunnel in nearly all individuals.10,11 Like the long flexor aberrant muscle bellies, in individuals with well-developed, elongated lumbricals or with shorter palm lengths, lumbrical muscles may be found in the carpal tunnel when the hand and fingers are in a resting position. While these lumbricals may be pulled distally out of the carpal tunnel with hyperextension of the fingers, it is easier to confirm a suspected lumbrical by moving the fingers into full flexion. During this motion, the lumbrical muscle bellies will increase in size, becoming more echogenic with increased resolution of a well-defined, outer connective tissue sheath.
Three study participants with aberrant muscle bellies identified in the carpal tunnel on the static images were selected for presentation in this report. First, two hypoechoic, circular structures were noted within the carpal tunnel of a healthy, asymptomatic 27-year-old man (Figure 3A). At first impression, the hypoechoic and uniform nature of these structures may be identified as blood vessels, an interpretation that can be ruled out using Doppler imaging. Similarly, these structures could be identified as a cyst, lipoma, or other mass, each of which could be further evaluated and potentially eliminated using Doppler techniques combined with application of pressure to determine if the structure is vascular, solid, or malleable. In contrast, the nonpathological identification of these hypoechoic structures as muscle bellies can be best confirmed through dynamic movement of the fingers. In this case, as the participant flexed the fingers to make a fist, these two structures were observed to shrink in a uniform manner and eventually disappeared (Figure 3B). When the hand was opened, the two structures reappeared in a uniform and consistent manner, confirming the fact that the structures were muscle bellies of the flexor digitorum superficialis.
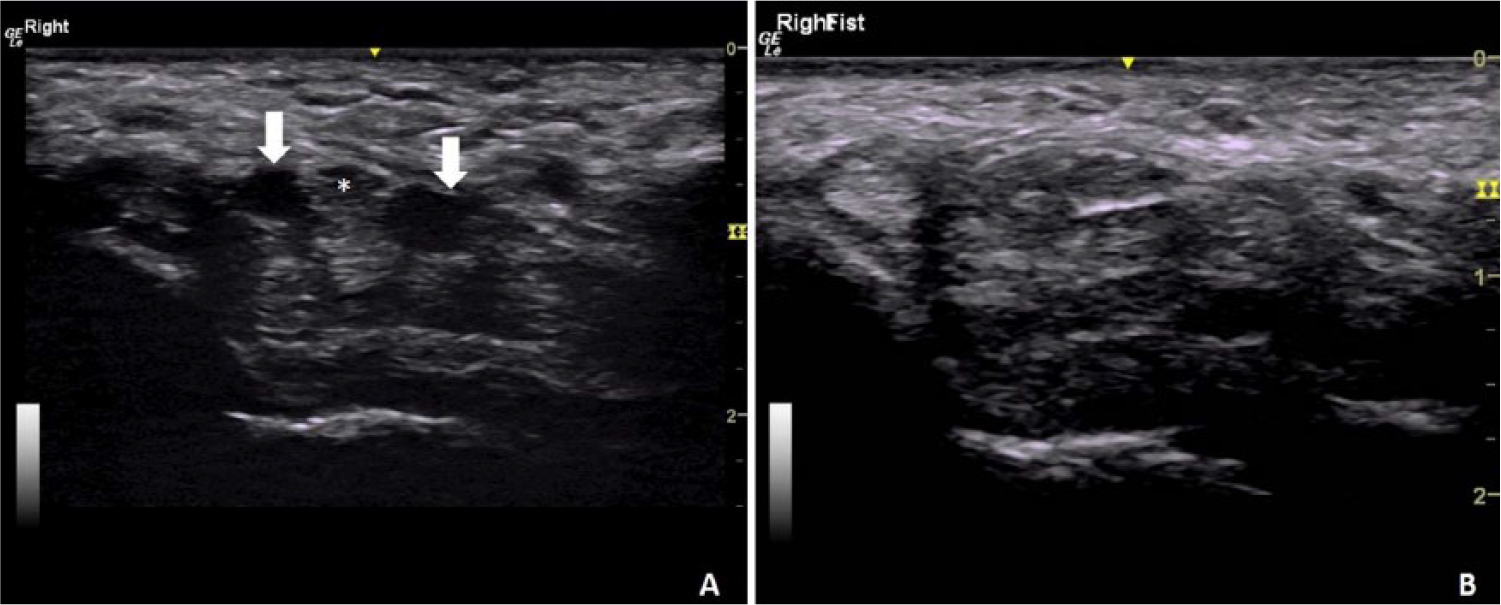
Two long flexor muscle bellies (white arrows) are present in the right carpal tunnel on either side of the median nerve (asterisk) while the hand and fingers were relaxed (A). As the participant flexed his fingers to make a fist, the flexor muscle bellies retracted proximally out of the carpal tunnel, resulting in an image with no evidence of muscle bellies at full flexion (B).
In a second case, a healthy, asymptomatic 24-year-old woman had multiple hypoechoic structures noted both when her hand was relaxed (Figure 4A) and with full finger flexion (Figure 4C). As with the first case, the presence of a long flexor muscle belly was confirmed when the hypoechoic structure immediately deep to the median nerve shrunk and disappeared as the participant made a fist. This disappearance was caused by the long flexor muscle belly retracting proximally out of the carpal tunnel (Figure 4B). The same hypoechoic structure presented itself again once the participant extended her fingers (Figure 4D). While this muscle belly was retracting from the carpal tunnel, a new set of hypoechoic structures appeared within the tunnel deep to the flexor superficialis tendons and superficial to the flexor profundus tendons (Figure 4C). The appearance and disappearance of these structures in the reverse of the flexor tendon muscle confirmed that these were lumbrical muscle bellies.
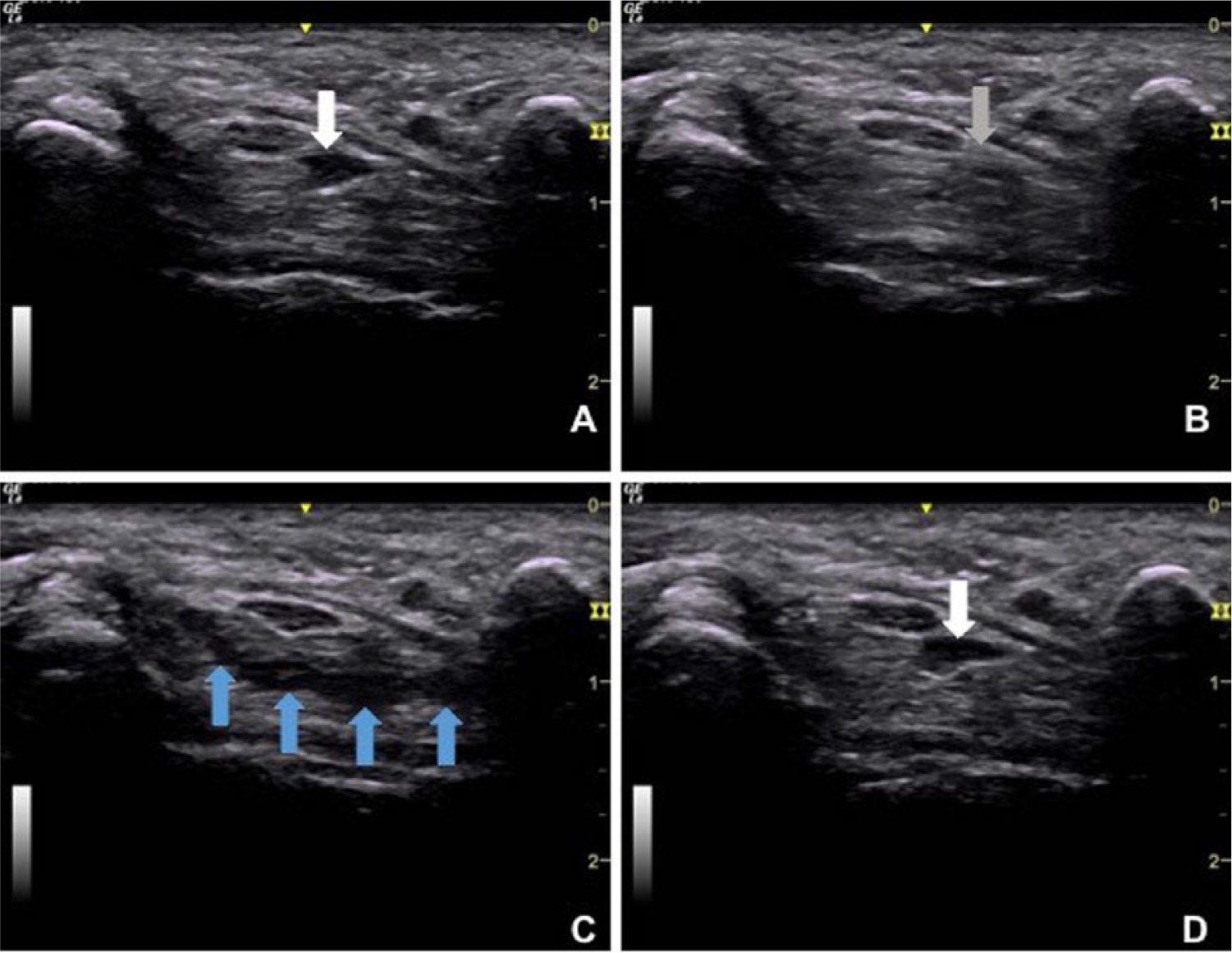
Serial images of the left carpal tunnel at the level of the pisiform. The participant was asked to open her hand with extended fingers (A), slowly flex her fingers to make a fist (B), hold the fist position for one second (C), and extend the fingers once again (D). As the participant makes a fist, the long flexor muscle belly (white arrow in A) retracts proximally into the forearm and is replaced by the flexor tendon (gray arrow in B). When the fingers are fully flexed, the lumbricals enter the carpal tunnel (blue arrows in C). Once the fingers return to extension, the long flexor muscle belly is seen in the tunnel once again (white arrow in D).
Finally, in the third case, a healthy, asymptomatic 35-year-old woman had a persistent lumbrical muscle belly within the carpal tunnel, even with the hand at rest (Figure 5A). In this case, identifying the aberrant structure that was present at rest as a flexor muscle belly was ruled out because the structure did not disappear with flexion of the fingers; it instead grew larger in a uniform manner and became more echogenic as the participant moved her fingers into full flexion. This consistent, uniform emergence of this structure confirmed its identification as a lumbrical muscle rather than a flexor muscle. In addition to this muscle, the lumbricals of the other fingers became apparent within the carpal tunnel once the participant had made a full fist (Figure 5B). Across all three cases, isolated flexion and extension movements of the individual fingers could have been used to specifically identify which of the four fingers (i.e., index, middle, ring, or small finger) the individual flexor or lumbrical muscles were attached to at their distal ends.
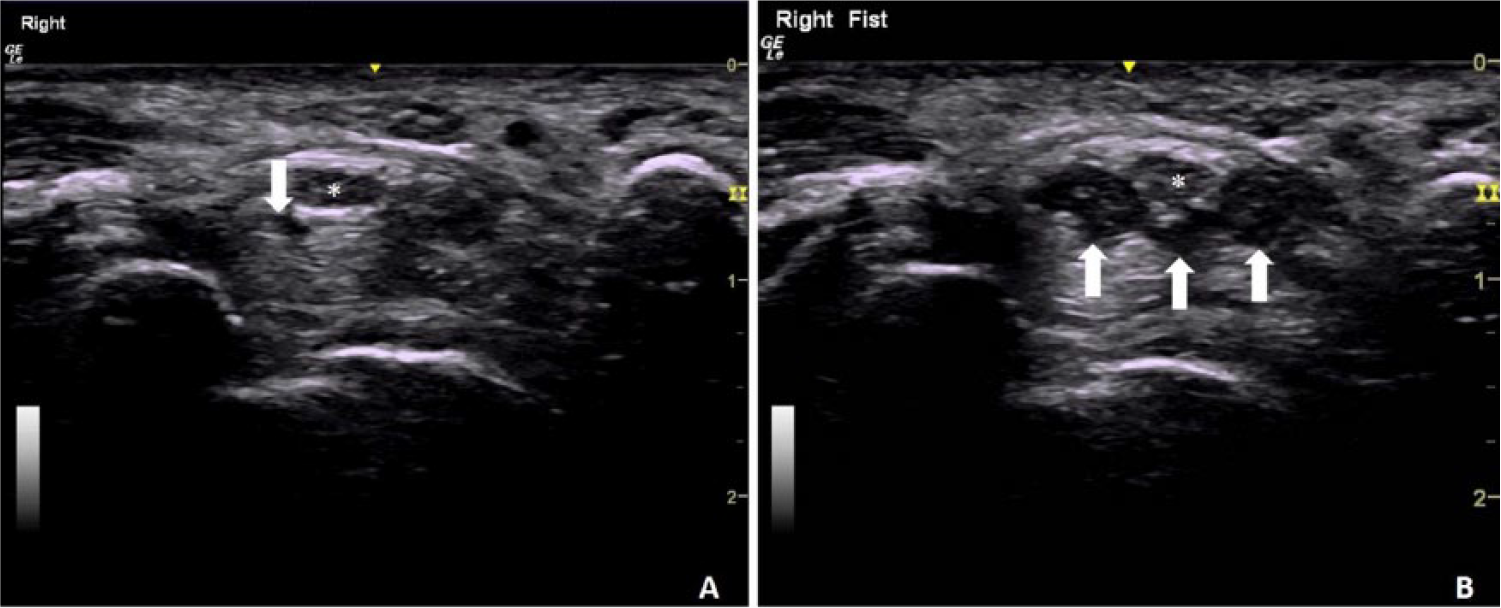
A small portion of a lumbrical muscle (white arrow) is present in the carpal tunnel next to the median nerve (asterisk) when the participant’s fingers are relaxed in partial extension (A). Identification of this structure as a lumbrical muscle is confirmed as this structure becomes enlarged along with additional muscles (white arrows) as the participant makes a fist (B).
Discussion
This case study report provides a description of various aberrant muscles within the carpal tunnel and information regarding how to accurately identify and confirm the sonographic appearance of each different muscle. It is important that sonographers are aware of these potential anatomic variants to properly identify these structures and avoid mistaking them for pathology. Potential differential diagnoses for aberrant muscle belly include the presence of a persistent artery or enlarged vein, lipoma or other mass, or a cyst or other inflammation around the tendons in the carpal tunnel. Doppler imaging, compression, and dynamic imaging can be used to differentiate these potential structures and pathologies. Proper identification as a nonpathologic aberrant muscle belly can most easily be confirmed with dynamic imaging, as finger flexion and extension will cause muscle excursion in and out of the carpal tunnel. In addition, investigation of the structure in the longitudinal plane will show elongated fibers that are continuous with the more proximal or distal muscle in the forearm or hand. Isolated finger movements or providing resistance against individual finger flexion during dynamic imaging can assist in identifying to which specific finger the muscle is attached.
While these anomalies should not be mistaken for pathology, the contribution of aberrant muscle bellies in relation to other pathologies should be considered. Specifically, case reports suggesting a link between aberrant flexor or lumbrical muscle bellies and carpal tunnel syndrome have been reported in the literature for more than 50 years.12–21 The continuous presence of muscle belly in the carpal tunnel even while the hand is at rest may compromise the available space within the tunnel. This loss of space may compress the median nerve, which can lead to the development of carpal tunnel syndrome.21,22 Although individuals with aberrant muscle bellies may be at increased risk for developing carpal tunnel syndrome, prospective or large-scale studies have not been conducted to establish any causative link.
In addition to carpal tunnel syndrome, another disorder in which aberrant muscle belly may be a contributing mechanism is trigger wrist.23–25 In rare cases, trigger wrist secondary to aberrant muscle may even present with carpal tunnel syndrome.24,26 Clinical presentations of trigger wrist include painful clicking, snapping, or catching sensation around the carpal tunnel during finger or wrist motion; in severe cases, wrist and finger motion may be limited by a triggering or locking of the joints. 27 The presence of aberrant muscle bellies within the carpal tunnel may cause compression within the tunnel space and impede tendon gliding of the wrist and fingers. In some severe cases, the anomalous muscle can heavily impede muscle and tendon excursion, limiting functional hand use and requiring surgical intervention. 28
Although evidence indicating a relationship between aberrant muscle bellies and pathology exists, the exact prevalence of these anomalous muscles within the carpal tunnel is unknown.11,21 Proper identification of aberrant muscle bellies in the carpal tunnel is an important first step to understanding their prevalence in the population. When evaluating the presence of aberrant muscle, it is important to note the positioning of the digits, as hyperextension of the metacarpophalangeal joints will likely cause the distal ends of the long flexor muscles to travel into the tunnel. Because the hand is rarely, if at all, used with the fingers in full extension or hyperextended, identification of aberrant muscles within the carpal tunnel in these positions has limited value. In contrast, understanding the prevalence of elongated or hypertrophic muscle belly in the carpal tunnel when the hand and fingers are relaxed or in various phases of finger flexion may be useful for furthering the evaluation of risk and development of median nerve pathologies at the wrist. Identifying individuals with these anomalies and observing the dynamic relationship between the aberrant muscle bellies and other structures within the tunnel can illuminate how these structures may contribute to the development of pathology. Knowledge of individual positions or movements that cause compression on the nerve can be used to establish preventative techniques to reduce risk of pathology development.
In addition to prevention, proper identification of these anatomical variants may be useful for informing interventions to individualize treatment methods that avoid complications and promote positive outcomes. For example, sonography-guided percutaneous carpal tunnel release requires careful delineation of anatomical structures along with continuous sonographic monitoring to successfully perform this minimally invasive surgical procedure. 29 Identification of aberrant muscles within the carpal tunnel will be important to avoid surgical complications, as it has been reported that muscle fibers may cross the line of incision in surgical carpal tunnel decompression in as many as 50% of patients. 30 When sonography is used to identify an anomalous or aberrant muscle as the likely cause of carpal tunnel syndrome, surgery to release the transverse carpal ligament can also include excision of the muscle belly to ensure full recovery and avoid remission. 31 In addition to surgical interventions, sonography may also be used to inform conservative treatment. For example, patients with carpal tunnel syndrome caused by incursion of aberrant lumbricals may require an orthotic that blocks metacarpophalangeal flexion rather than the standard wrist cockup splint that does not block the lumbricals from entering the carpal tunnel. 32
Conclusion
Aberrant muscle bellies in the carpal tunnel region may exist in healthy individuals and may or may not be related to pathology or symptoms. Learning to correctly differentiate aberrant muscles in the carpal tunnel space from other structures and pathologies, such as cysts and lipomas, is vital to ensure patients are not misdiagnosed. Moreover, using sonography to advance understanding of these structures in relation to the median nerve can assist in evaluating a potential contribution to the development of median nerve pathologies, as well as inform interventions for prevention and treatment of carpal tunnel syndrome.
Footnotes
Acknowledgements
We thank Jennifer Mitchell for her help in image acquisition and identification to support the development of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health (NIOSH) (grant R01 OH010665). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.