
Abstract
Concern for patient safety and increased demands on health professionals have resulted in challenges for the clinical training of sonography students. The purpose of this study was to examine simulation use in Commission on Accreditation of Allied Health Education Programs (CAAHEP)–accredited sonography programs. A prospective cross-sectional study was conducted. Program directors were sent a survey that addressed the use of simulation and the perception of simulation’s educational value. Of the 230 sonography programs identified, 137 responded, for a response rate of 60%. Of the respondents, 75% indicated they used simulation and 89% reported that it was a good teaching tool. The programs indicated that 81% recorded a positive student experience using simulation. Simulation was rated most useful for improved anatomic identification (55%) and transducer manipulation (64%). Simulation is commonly used for educational training in CAAHEP-accredited sonography programs and is perceived as a positive tool to enhance education of students. More research is needed to establish best use and educational practice.
Students in the health care professions have routinely acquired training through didactic and clinical instruction. With increased demands on health care professionals in the clinical environment and more emphasis on patient safety, there is less opportunity for preceptors to clinically train students.1–3 Teaching sonography is particularly challenging as students must achieve cognitive, affective, and psychomotor knowledge and skills. Knowledge of anatomy, physiology, pathology, physics, and patient care techniques are all important; however, learning to perform and achieve proficiency in sonography has unique challenges. Sonography is an operator-dependent modality requiring a significant amount of effort, faculty time, and equipment, and it has a substantial learning curve. New simulation technology is now available and has enabled viable options to supplement students’ basic sonography training. While adoption of simulation is documented with regard to training pharmacists, 4 dentists, 4 nurses,4,5 physicians’ assistants, 6 medical students, physicians, 7 and allied health undergraduate level students,8–10 there is a gap in the literature on the topic of simulation use within sonography educational programs.
Simulation is not a new concept for training professionals. It has been used in aviation, spaceflight, nuclear power, and the military to provide enhanced training for high-risk environments where professionals must acquire unique skills that require precision and swift decision-making processes while performing life-or-death actions.11,12 Simulation-based training has been promoted by the Institute of Medicine as a means to increase patient safety and has been adopted by the medical community as a method for training novices.3,13,14
In a clinical training competition, medical students who received simulation training achieved significantly higher scores (P < .05) than those who trained using traditional educational methods. 15 In a pilot study of point-of-care sonography (PoCUS) training, a group of medical students with no prior experience were given a curriculum based on online didactic course materials and a high-fidelity cardiac simulator. They were to acquire and interpret echocardiographic shock images from the Acute Care Education Systems’s cardiac protocol. Participants were assessed with 72 simulated scenarios and were able to obtain 99.7% of the sonographic windows (574/576) and correctly analyzed 93% of the PoCUS examinations (67/72). 16 Simulation has been embraced as a training mechanism used by anesthesiology, emergency medicine, surgery, obstetrics, and gynecology residency training programs and aligns well with adult learning theory. Successful use of simulation has also been demonstrated for training cardiology fellows in transesophageal echocardiography. 17
Medical simulation provides a supportive environment in which students can actively learn teamwork, procedural skills, and make mistakes as well as practice clinical decision making without adverse effects to a patient. This may be due to the advanced simulation technology and training techniques.1,2,5,12 A study by Nelissen et al. 18 demonstrated a 38% reduction in the incidence of postpartum hemorrhage after simulation-based training, improving prevention and management of postpartum hemorrhage, thereby reducing the rate of maternal mortality.
Long-term outcomes of simulation training can be difficult to assess because of confounding variables of pursuant clinical practice. However, a number of studies have demonstrated evidence of long-term retention of skills.8,9,19 There are two categories of medical simulation. The first is team simulation, which allows a multidisciplinary group to practice drills with both situational awareness and knowledge. In this case, team interaction is a priority. The second category is technical simulation, which focuses on achieving proficiency or improvement with repetitive practice in a safe setting. 12 The present study investigated the use of technical simulation.
Types of Ultrasound Simulation
Simulation has been further divided into low fidelity and high fidelity. Low fidelity primarily is associated with task trainers and is used for procedural training. Adding a task trainer with an immersive environment can create a high-fidelity experience. 13 Sonography simulation can be divided into four types:
Homemade simulators can be created with everyday materials found in the grocery store (e.g., gelatin, turkey, olives). These are cost-effective but have limited shelf life because of rapid deterioration (Figure 1). These activities usually require faculty oversight. Assignments are sometimes given in combination with a simulator, as a student review activity. Creating these phantoms can also be useful in teaching the physics of ultrasound and for practicing sonography-guided procedural techniques.
Computer-based programs provide students with a username and password granting access to modules via website. These modules can include lessons on anatomy and transducer orientation (Figure 2). The program enables students to practice scanning by using a mock transducer or mouse and provides simulation and cognitive activities for the student to complete. The student receives feedback on the simulated scanning experience and content knowledge. Learning is generally considered to be self-directed. 11
Low-fidelity phantoms or task trainers are used in conjunction with ultrasound equipment and a transducer. The phantom (task trainer) is usually a specific body part; however, it is rarely an entire mannequin (Figure 3). The images generated are similar to human anatomy and can present as normal sonographic anatomy or pathology, much like a real patient (Figure 4). This type of simulation allows the student to practice using a functioning ultrasound system and provides an opportunity to focus on knobology, transducer manipulation, and image optimization. In this case, the student will receive expert feedback only if faculty members are present. The phantom may not be exceptionally lifelike, but sonographically, it does provide for images that are representative of human anatomy.
High-fidelity simulation uses a mannequin and/or mock transducer. The mannequin is embedded with electromagnetic markers that integrate with advanced computer software, attached to the system. Some platforms use computer-generated images, while others use images reconstructed from real sonograms or computed tomography. Some high-fidelity products also include a haptic device that provides the user with feedback on transducer pressure, angle manipulation, and orientation (Figure 5). All high-fidelity products provide users with some metric feedback allowing the user to gauge their success against a standard. In some cases, they have additional resources and learning activities available to the learner. The primary focus is learning scan planes, spatial orientation, optimal image acquisition, and identification of anatomy and pathology. 12 Case studies and libraries of pathology may be provided for the student as well.
Sonography simulation equipment is a useful learning tool that can accelerate acquisition of scanning skills. 12 It can also provide resources for students to learn how to scan in a low-risk and stress-free environment. 12 Students may practice at their own pace, repeating and refining certain views, instead of practicing on an actual patient.1,20,21 Simulation offers a safe environment for constructive feedback and independent training through trial and error. 5 Students can apply what they have learned in lecture to a setting that represents clinical reality and acquire the necessary skills to succeed. Gibbs 22 demonstrated that sonography students exposed to sonography simulators during their training reported greater confidence in their ability to identify images and structures. The students also demonstrated greater confidence in their scanning skills. 22 Student readiness for the clinical environment can be improved by using simulation activities.6,20,21 Programs using sonography simulation have the ability to enhance the learning experience of students by creating an interactive, learner-centered environment.10,22,23 The purpose of this study was to examine if simulation is being integrated into Commission on Accreditation of Allied Health Education Programs (CAAHEP)–accredited sonography programs and to identify factors that promote or deter adoption.
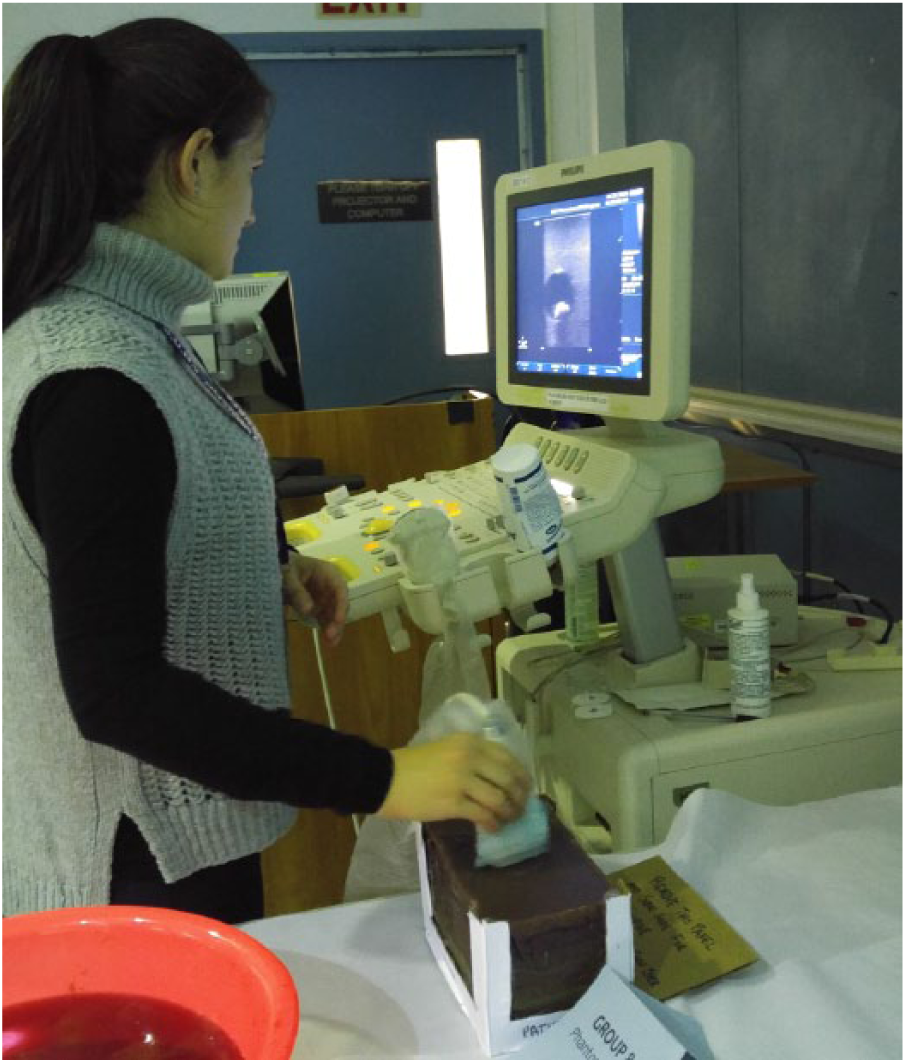
Student scanning a homemade phantom.
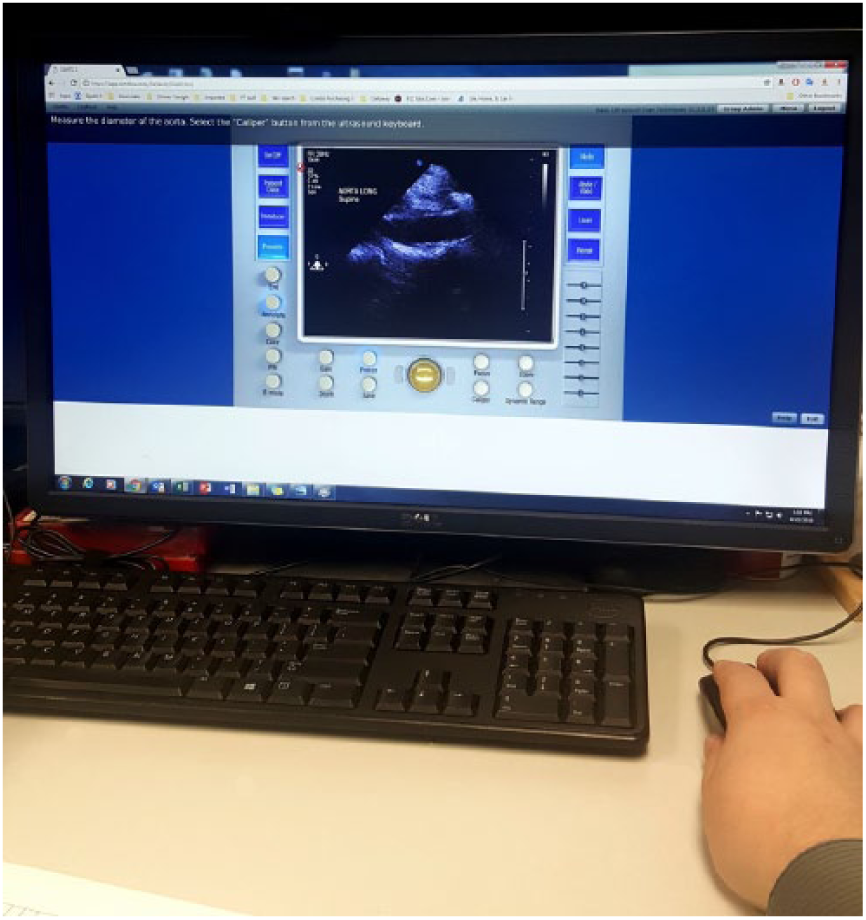
An example of a computer-based sonography simulation product.

Student scanning an obstetric fetal phantom (low fidelity) with a standard ultrasound system.
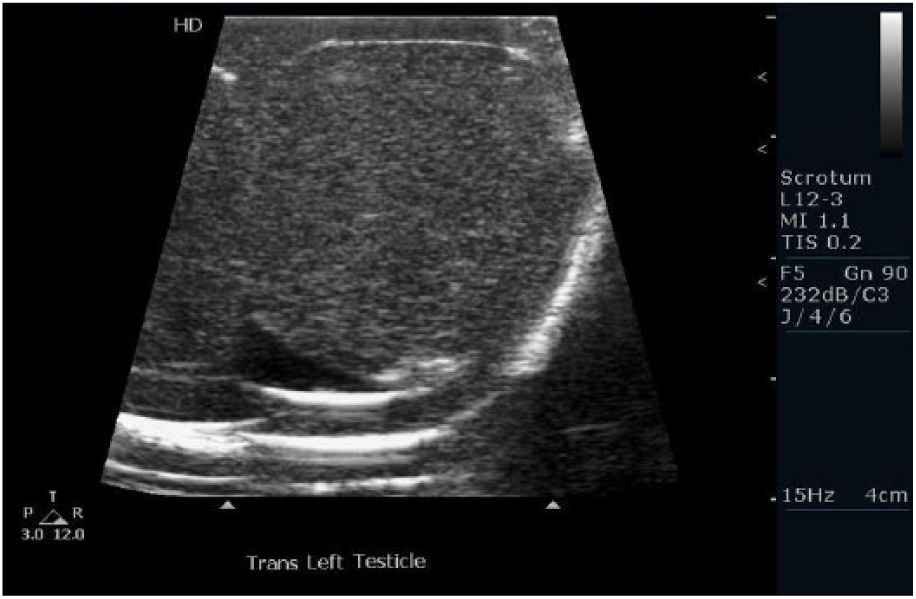
Image obtained from a commercially available testicular phantom.
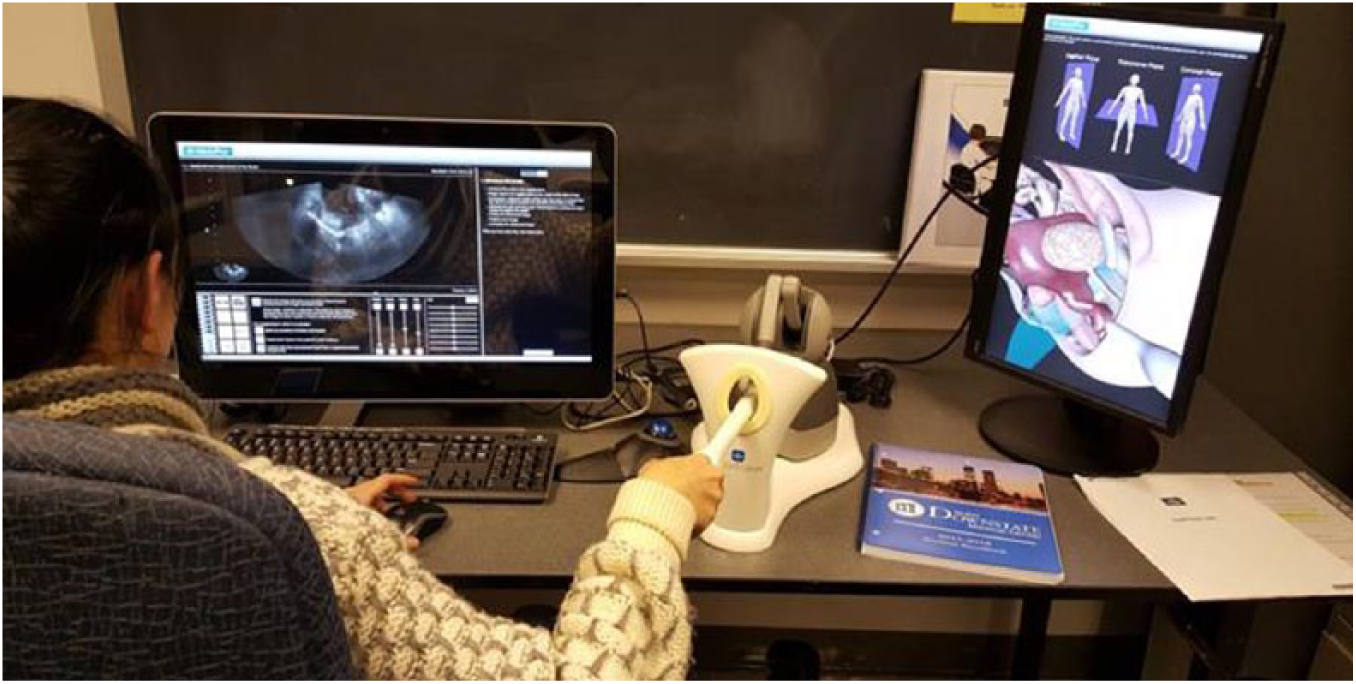
High-fidelity computer simulator with haptic device.
Materials and Methods
This study was reviewed by the State University of New York Downstate Medical Center Institutional Review Board and deemed exempt. CAAHEP-accredited sonography programs were identified using the online CAAHEP directory search tool, and program directors were invited via email to participate in this study. The email included a cover letter, information sheet, and unique, single-use link to a Qualtrics-generated questionnaire. Page logic and skip logic were used in the design, allowing respondents to bypass nonapplicable questions. The survey was open from February 10 to March 18, 2016. Invited participants received four reminders over the course of a month. Content addressed included questions about school type, availability of simulation, application, use, faculty participation, and perception of simulation as an educational tool. All responses were recorded as anonymous. Descriptive statistics and chi-square analysis were used to analyze the data as applicable.
Results
A total of 230 program directors were identified and invited to participate in the study. A 60% response rate was achieved, and 137 program directors responded to the survey (Table 1). Use of simulation equipment was reported by 75% of CAAHEP programs, with a margin of error of 5%, for teaching obstetrics, gynecology, abdominal, cardiac, vascular, and small-parts sonography (Figure 6). Eighty-nine percent of respondents described simulation as a useful teaching tool, and 81% reported that students expressed positive feedback after participation in simulation training. Respondents who expressed a negative view regarding the use of simulation (11%) indicated that they did not use simulation and they preferred students scan each other.
Demographics of Responding Sonography Programs.
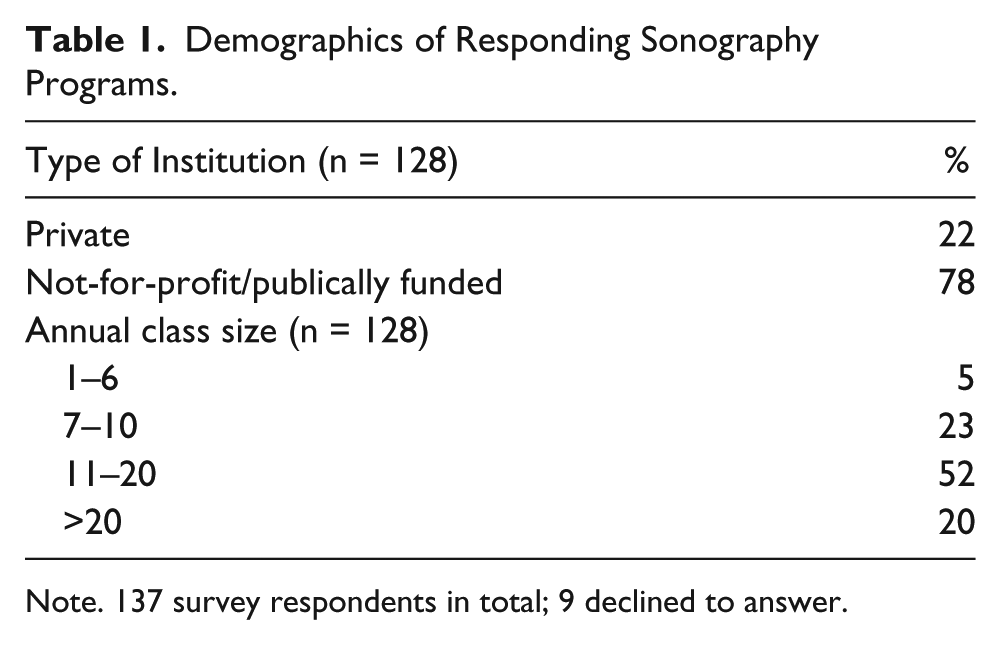
Note. 137 survey respondents in total; 9 declined to answer.
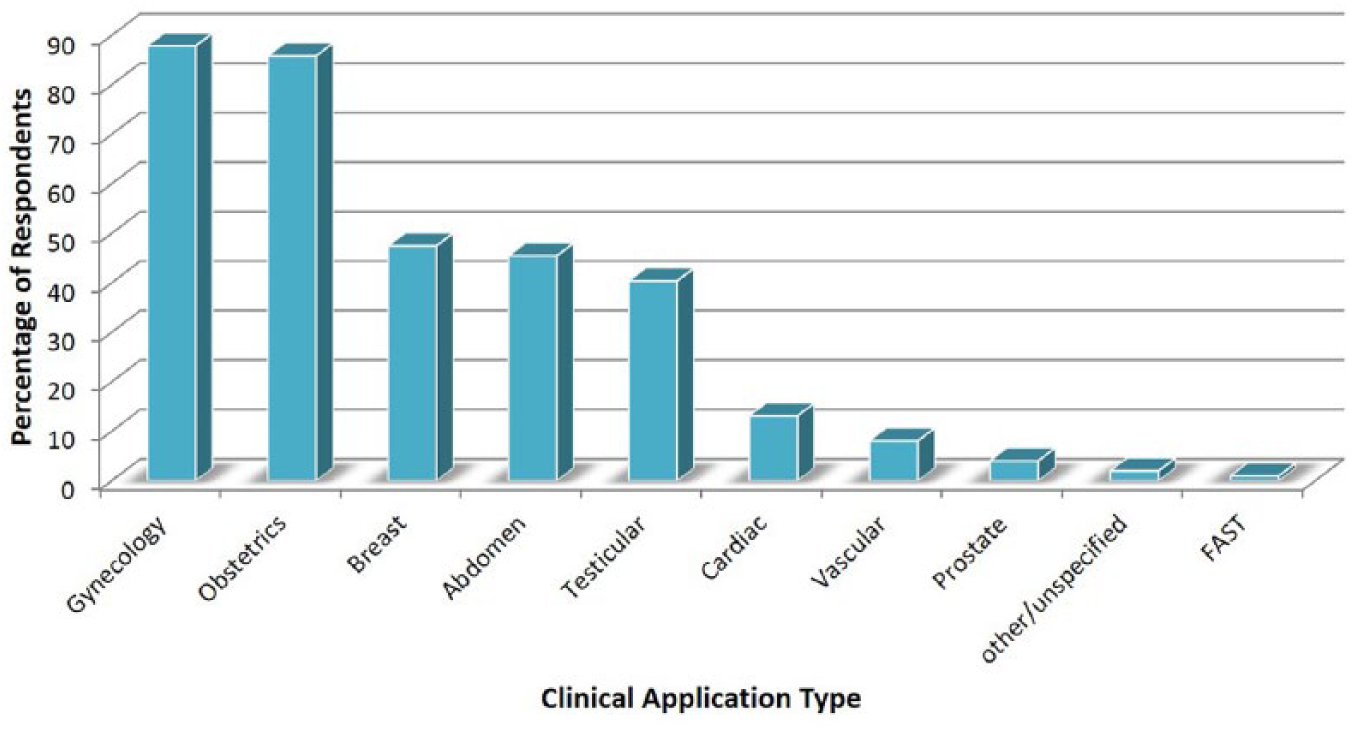
Simulation use by specialty.
Use of Simulation
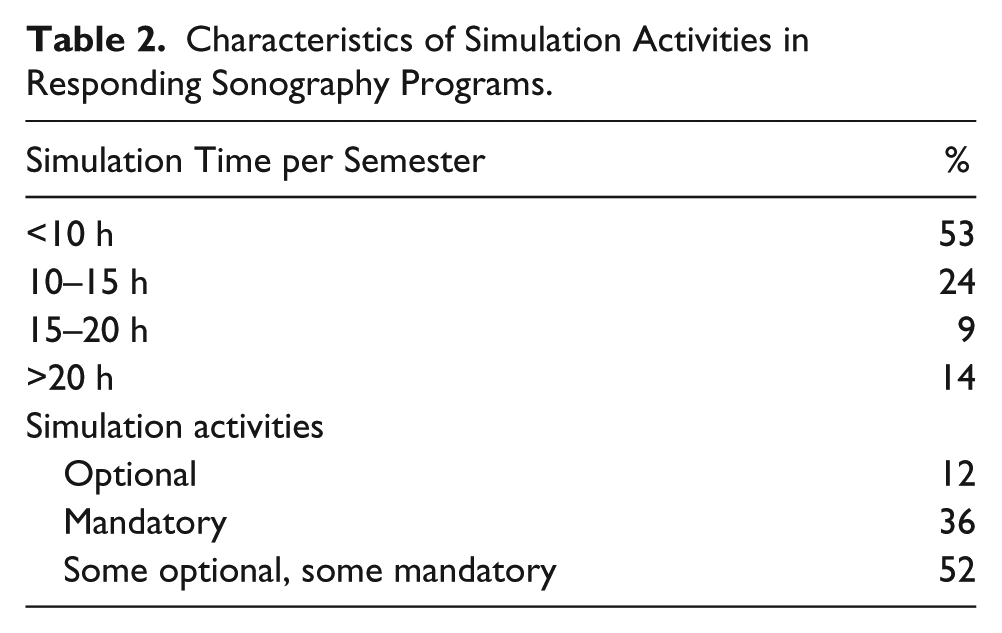
Program directors reported that simulation was used most often to teach anatomy (83%) as well as scanning protocols (66%), pathology (65%), scanning skills and muscle memory (46%). Twenty-four percent reported use of simulation for remediation. Simulation activities were most often a combination of optional and mandatory sessions (52%), with less than 10 allotted hours per student per semester (Table 2). Thirty-three percent of program directors indicated that students requested more time with the simulators. A variety of simulation equipment was available for use by sonography students (Figure 7). Students were allotted an average of 30 minutes to 1 hour for each session.
Characteristics of Simulation Activities in Responding Sonography Programs.
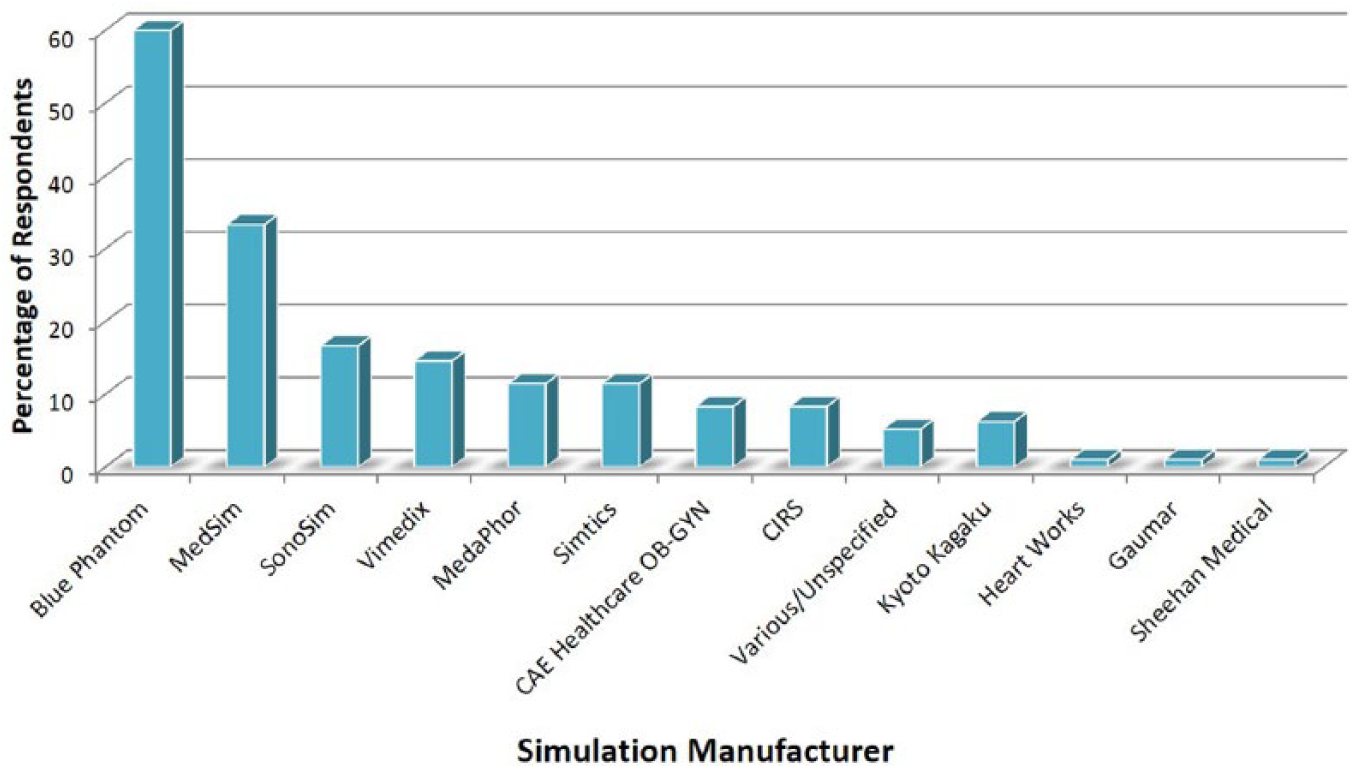
Simulation products reported by Commission on Accreditation of Allied Health Education Programs–accredited sonography programs.
Educational Applications
Simulation can be used for many specialty applications. Program directors identified its use for multiple specialties; obstetrics and gynecology simulators were reported with the highest frequency (Figure 6). Directors were asked if they were able to identify student improvement in transducer manipulation after simulation activities: 64% indicated yes, 32% were unable to determine, and 4% reported no. Fifty-five percent noted student improvement in identifying normal anatomic structures. Student performance after simulation was evaluated by 66% of programs; however, assessment tools were not reported by the programs nor provided by the researchers of this study.
Role of Faculty
Only 20% of programs provide faculty for low-fidelity phantom scanning workshops, and 30% provide faculty for high-fidelity simulation. Alternatively, 76% of respondents felt it was necessary to have an instructor during simulation training. Participants noted that training of faculty requires time and resources that may take away from primary teaching responsibilities. This may be an impediment to curriculum development and implementation.5, 12
Perception of Simulation and Impediments
Of the 25% of programs that responded that they did not have simulation, 74% indicated they want to acquire simulation and incorporate it into their future curriculum. Of the 34 programs that responded they were not using simulation, 68% noted the most significant reason for not using sonography simulation equipment was cost. If programs have simulation equipment, 88% believe participation in these activities should be mandatory for all students. Most indicated that hands-on simulation should not replace lecture or clinical time (77%). The chi-square statistic was used to measure whether a distribution of observed outcomes differs from the expected. The chi-square test was used to determine if there was an association between size of program (number of students) and likelihood of sonography simulation equipment being used. Statistical significance was set at P < .05 a priori. This association was found to be insignificant with a P value of .81. Private versus nonprofit status had no bearing on whether a school had simulation equipment with a P-value of .17.
Discussion
Educating sonography students is a complex process. Students may acquire their scanning skills in a school-based student laboratory, but students primarily acquire and hone these skills during their clinical internships. There is widespread diversity and lack of uniformity in terms of the types of patient population and pathologies that a student encounters during his or her clinical rotations. Practicing on real patients can also be fraught with possible unnecessary discomfort or risk to the patient.20,21 Simulation can provide educational opportunity to master psychomotor skills, even when patients and/or faculty are not available.
Advantages
Simulation provides a learner-centered environment, in contrast to learning sonography clinically, where the environment is patient centered.5,24 Students can ask faculty questions without concern for a patient’s reaction or possible pain and repeatedly practice their technique until mastered. Using simulation allows students to make mistakes and build confidence in their skills and knowledge without any adverse effects or embarrassment. 2 They can role-play scenarios and practice their affective skills. They can work on their scanning skills with deliberate practice until they feel confident in their abilities. 5 Students can also be exposed to pathology that they may not routinely find in certain patient populations.20,21
This study revealed that 75% of the 137 CAAHEP-accredited programs participating in the national survey incorporated sonography simulation technology into their general, vascular, or cardiac curriculum. Reported types of simulation included computer-based programs, task trainers in conjunction with sonography equipment, and high-fidelity mannequins, as well as computerized haptic simulation devices. Many program directors (40%) shared their experiences by contributing to open-ended questions. Most provided positive feedback describing their experience with using simulation as a means to introduce complex scanning techniques to the new student. They also used simulation for transvaginal and testicular sonograms, sensitive examinations for both student and patient alike.
Different types of simulation platforms can be used for different educational goals. Computer-based products (Figures 2 and 8) may provide basic knowledge and feedback on transducer orientation for beginning students, while other high-fidelity products may be equipped with a haptic device providing opportunity and immediate feedback to the student on their obstetric, gynecologic, and cardiac scanning capabilities (Figure 9). Computer-based simulation with mock transducers allows the student to acquire the knowledge and skills required for cardiac and obstetric scanning, with tailored feedback. Many simulation products include mannequins, embedded tracking devices, and/or self-directed educational content working in tandem to provide a high-fidelity scanning experience for the student (Figures 9 and 10). Workshops using task trainers coupled with sonography machines require faculty support for a most effective experience and allow students to practice scanning techniques while gaining experience with sonographic anatomy and image optimization. 23
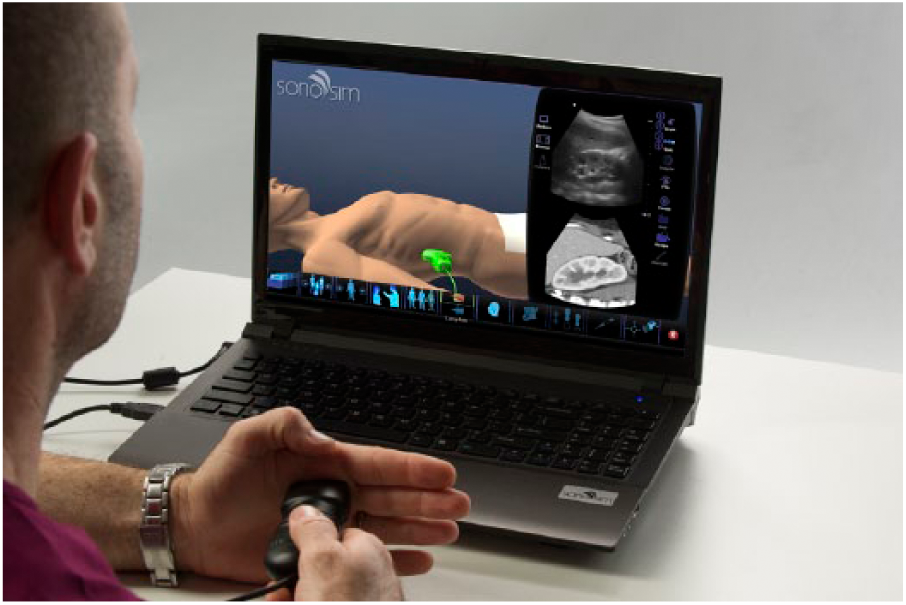
An example of a web-based simulation product with mock transducer.
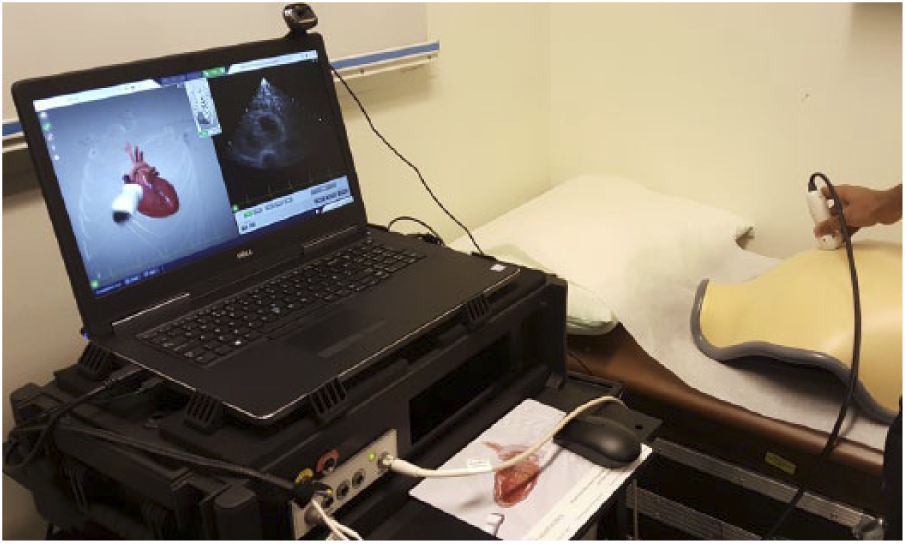
A cardiac simulator with a mock transducer and vest.
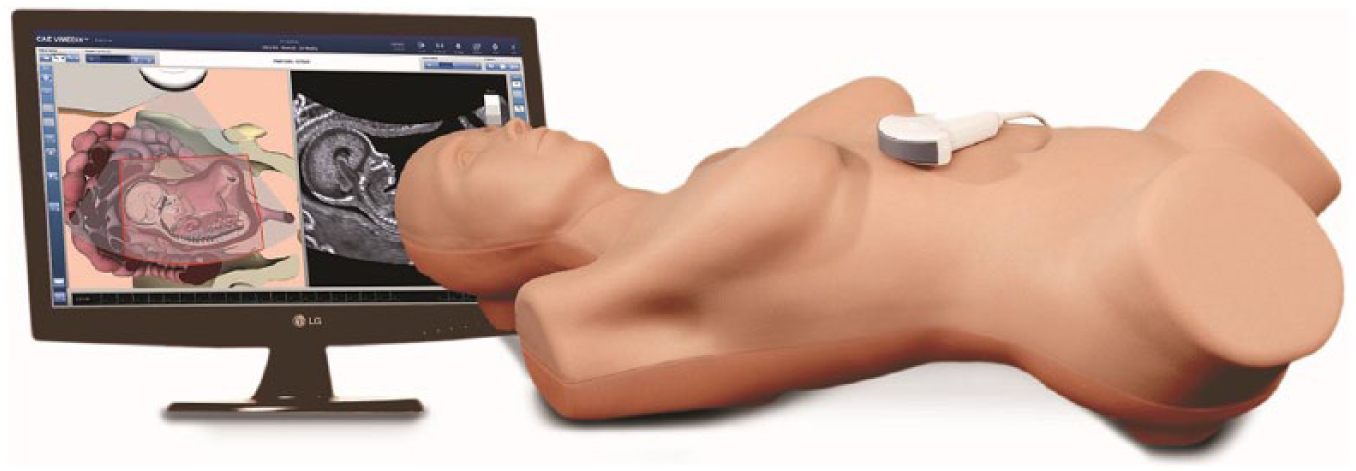
Obstetric and gynecology high-fidelity mannequin, mock transducer, simulator product (CAE Healthcare; used with permission).
Most program directors saw an improvement in identifying anatomic structures, and one-third reported that their students were able to better apply ultrasound physics because of simulation activities. Adult learners are receptive to this type of independent hands-on experiential learning, which provides problem-centered skills directly relevant to their future profession.1,5,13,21,25
CAAHEP-accredited sonography programs use simulation predominantly for obstetrics, gynecology, breast, and testicular sonography. This is potentially because of the type of equipment available and the challenges and sensitivity these types of sonograms require. Deliberate practice can decrease discomfort and unease that students may experience when performing these types of scans. 23 Students may have less clinical experience with breast, transvaginal, and testicular sonography because of patient consent; therefore, simulation provides students with a greater opportunity to practice. Patients may not be comfortable with an inexperienced student performing a sonogram on these areas. 21 Students using simulation equipment can practice transvaginal scanning prior to scanning a real patient, increasing confidence and skills, which translates into a more efficient and safer experience for patients.20,21
One variable to consider is the timing and implementation of these learning activities, as a preparation prior to clinical exposure, that improves student skills and facilitates concurrently learning in the clinical setting.12,20,22 Some students using simulation technology have found value in these activities prior to their clinical internship, because simulation provided the opportunity to acquire a higher level of readiness, comprehension, and skill in working with a patient.21,22 Concurrent practice with didactic sessions throughout education can also be particularly useful. Simulation can be used to assess levels of competency, with a more uniform testing environment for students,2,6 and it provides remediation for students receiving negative feedback from clinical preceptors.
Challenges and Limitations
It is well recognized that there are limitations to simulation technology, as simulators that exist today are not identical to live patients. Even high-fidelity simulation technology cannot replicate the experience of a difficult patient because of the attitudes of human interaction or challenging body habitus. They may not address challenges of fetal movement with obstetric scanning nor patient feedback or breathing pattern. Although simulation is useful for guiding students in acquisition of knowledge and skill, it is limited for teaching patient interactions and attitude. 21 Simulation is perceived as a valuable tool used for teaching students how to identify anatomy and pathology while providing the ability to practice and refine scanning techniques. It is not enough to just provide access to the simulation equipment. Programs must use foresight and create a curriculum with goal-oriented objectives and assignments to maximize learning opportunities.1,5 Resources are currently a challenge for many schools.5,12,26 Integrating simulation into a program requires funding, physical space to house equipment, faculty knowledgeable in teaching techniques, and various simulation products, as well as dedicated time to implement into an existing curriculum.12,20,26 Although most programs use some measure of simulation, CAAHEP currently does not accept simulation for establishing student competency.10,27,28 This may change in the future as nursing and medicine already recognize the value of using simulation exercises for continuing education. 5
Many clinicians and educators agree that simulation should not replace clinical experience, but simulation can still play a significant role in student readiness and deliberate practice for skill acquisition.1,2,5,6,12,14
Those surveyed program directors who expressed interest in incorporating simulators into their curriculum had a variety of reasons for not implementing. It is often very costly to purchase and maintain equipment, and many programs lack the budget for these recurring costs. School administrators may not see a value or benefit to simulation based on their lack of awareness of the technology and its capabilities. Some programs have outdated imaging equipment that is ineffective, lacks image quality, and is not the current standard of care. These reported barriers to simulation are similar to the findings of a national study assessing the use of simulation in educational programs for physician’s assistants. 6 It is interesting to note that insurance incentives are being provided to physician groups that participated in simulation training, with the understanding that this training improves patient safety. 20
Although most respondents of CAAHEP programs use simulation, 9% indicated they were not interested. Survey responses indicated that these programs relied on students scanning each other and clinical education for gaining the required skills to be a competent sonographer. It is possible that these students are at a disadvantage, given the greater stress during clinical rotations to obtain proficiency. This also has potential effects on the patient, clinical preceptors, as well as the student. 21
Limitations of the Study
This study evaluated acquisition and overall use of simulation. It did not provide an opportunity for participants to specify at what point in the curriculum simulation was used or which concentration(s) were programmatically accredited. It also did not capture the distinction between using low and high fidelity, in terms of the program’s differentiated use and application. The study assessed only the use of simulation technology and did not inquire about students scanning each other, as it was assumed that most programs practice this form of training. It would have been interesting to note whether those that did not integrate simulation technology into their curriculum required a greater number of clinical hours for their students. This study focused on feedback from program directors and did not investigate student satisfaction directly. No assessments of educational outcomes were addressed. This study did not investigate specific activities used in simulation training. It would be valuable to explore the actual activities that CAAHEP programs are using to evaluate the educational impact these opportunities provided.
Conclusion
This study illustrates for the first time a description of national simulation use in CAAHEP-accredited sonography programs across the United States. Most of the CAAHEP-accredited sonography programs incorporate simulation technology for many specialties, including obstetrics, gynecology, cardiac, breast, abdomen, testicular, vascular, and prostate. Simulation is integrated into the curriculum for anatomy, pathology, image acquisition, optimization, hand-eye coordination, and muscle memory, as well as feedback on techniques and deliberate practice of scanning skills.5,12 Simulation has become a commonly used tool for educating allied health and medical professionals.6,14,21
Factors that may prevent acquisition of sonography simulation include cost, maintenance, and the proper ratio of student to technology availability. There is also limited published evidence that simulation as a learning strategy provides a path to a more effective acquisition of technical skills that can justify an administrative purchase.2,6,12,26
Sonography simulation has repeatedly demonstrated opportunities for students to increase their knowledge, procedural skill, and confidence in sonography, which may provide better outcomes than traditional didactic education.4,12,21 Sonography simulation may be a valuable educational tool that should be used in conjunction with didactic and clinical education.1,2,4,12,14,21,23,29 While technologic advancements make simulation an attractive option, it is important to use appropriate instructional design when creating this type of curriculum.5,14,30 The Accreditation Council for Graduate Medical Education has recognized the positive attributes simulation provides and revised their guidelines to include simulation for anesthesia and surgical residency competencies.31,32 As simulation technology continues to evolve and clinical safety remains a priority, it will be interesting to see the effect simulation has on advanced sonography education, credentialing, and competency.
Now that it is evident many CAAHEP-accredited sonography programs have simulation equipment, it is time for increased dialogue about the use of simulation for student education. Future studies can explore the use and timing of integration of simulation into the curriculum, assessing specific clinical skills of student sonographers as compared with clinical training alone, as this has not been well documented. 21 Subsequent research should be conducted to identify and ascertain best practices for using sonography simulation.
Footnotes
Acknowledgements
The authors would like to acknowledge Camille Abadia, BS, RDMS, RDCS, Devorah Arastehmanesh, BS, RDMS, RDCS, Sally Mineh, BS, RDMS, RDCS, and Rebecca Orlinsky, BS, RDMS, RDCS, who assisted with data collection for this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.