
Abstract
Sonographic evaluation is the gold standard in diagnosing of testicular microlithiasis, the nature of which has raised controversy in opinions regarding its premalignant or benign tendency. Testicular microlithiasis is often an incidental finding on sonographic examination with indications for other disease processes, and it may or may not require additional follow-up. This pathology has raised equal interest among domestic and foreign researchers, and studies have been performed on both adult and pediatric populations, yet there is no standard recommendation for follow-up care of testicular microlithiasis. Isolated testicular microlithiasis and that with additional risk factors may require different approaches to testing and care. In this publication, a case study is reviewed and two approaches to follow-up care of testicular microlithiasis based on the associated risk factors or a lack of thereof are discussed.
Testicular microlithiasis (TML) is a well-known yet poorly understood pathology. It was first described sonographically in 1987. 1 Due to its unknown etiology, differences in the studied population, and its low incidence range of 0.6% to 5.6%,2,3 this condition remains challenging to understand and to establish its benign or premalignant character. In the late 20th century, TML was considered to have a strong correlation with the development of testicular neoplasia and testicular germ cell tumors in particular. 4 This resulted in an increased number of follow-up examinations and testing. 4 Due to high-resolution imaging, the frequency of TML detection has increased. This, along with a series of retrospective studies conducted in the 2000s, has changed the current view on TML. Additional risk factors are considered when establishing a follow-up regimen for a patient with TML, especially if discovered as an incidental finding. 5
Case Study
A 9-year-old Hispanic male presented to the sonography department for evaluation of a suspected undescended right testicle, a testicular pathology known as cryptorchidism. The patient’s history was unavailable, and it is unclear why his condition remained untreated.
A linear array transducer with a center frequency of 12 MHz was used on Logiq E9 equipment by GE Healthcare (Chicago, IL) to perform the scrotum examination. Upon the evaluation, the undescended right testicle and epididymis were visualized in the right inguinal canal (Figure 1A,B). The right testicle measured 1.3 × 1.1 × 2.0 cm for a total volume of 2.0 mL. The left testicle was visualized in the scrotum measuring 1.2 × 1.2 × 1.9 cm with the volume of 1.9 mL (Figure 2A,B). (Volume measurements were calculated using L × W × H × 0.71 formula. 6 ) There were no hydrocele, varicocele, or other focal lesions observed. However, diffuse, highly echogenic, nonshadowing, punctuate foci were present bilaterally. The sonographer’s impression stated these findings. The radiologist’s report concluded that an undescended right testicle was located in the right inguinal canal. The left testicle was normally located within the scrotum, but extensive bilateral TML was noted.
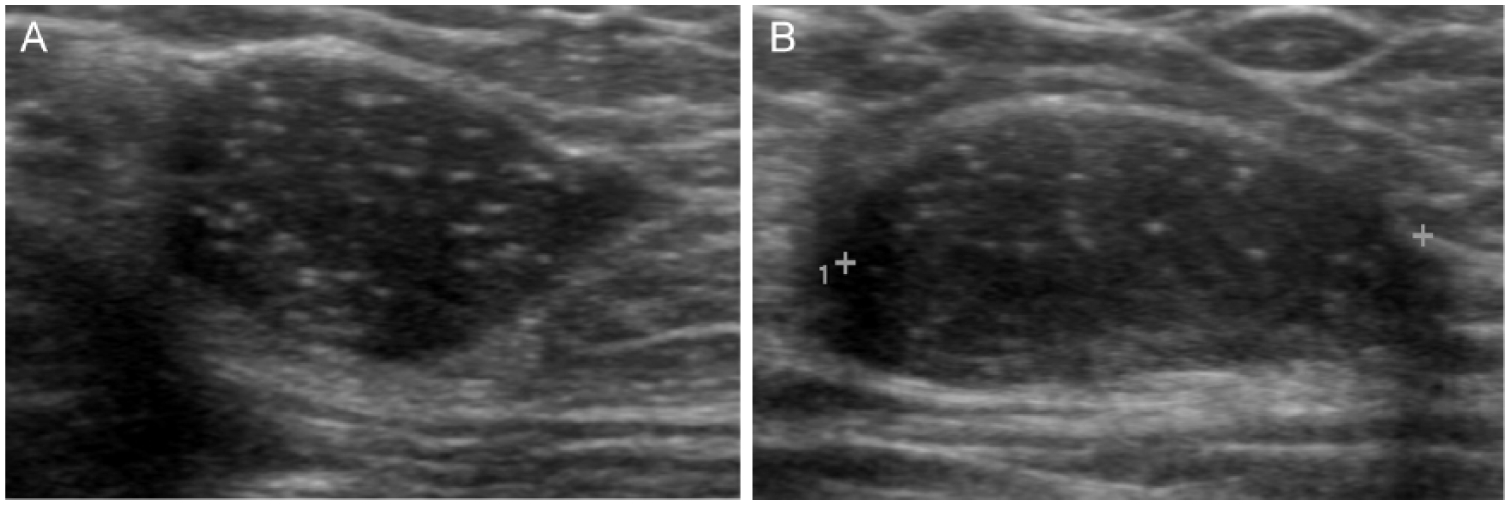
(A) Undescended right testicle, inguinal canal, transverse plane. (B) Undescended right testicle, inguinal canal, sagittal plane.
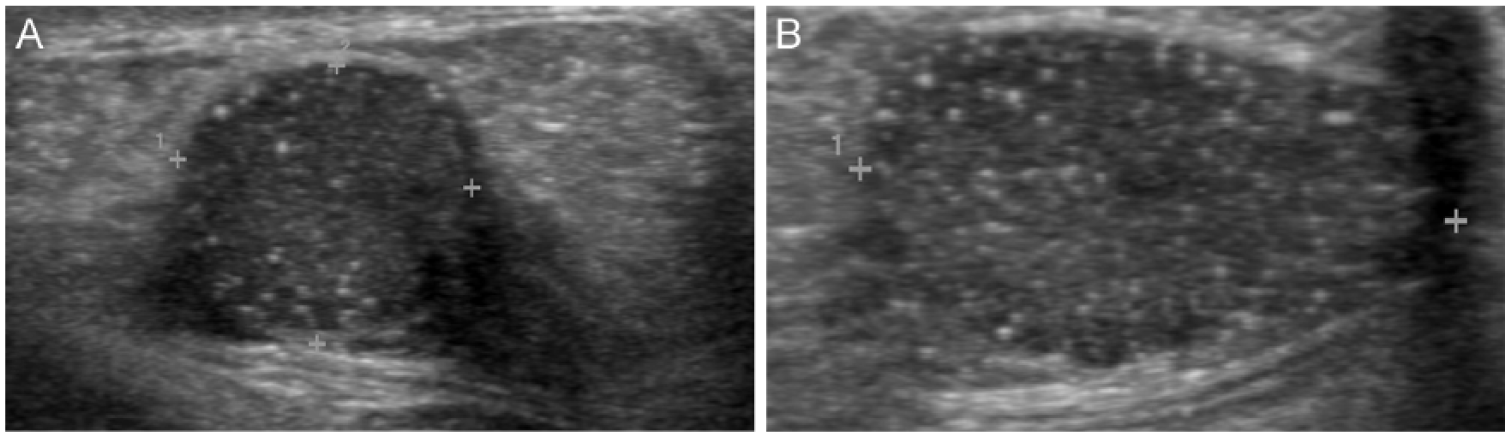
(A) Descended left testicle, scrotum, transverse plane. (B) Descended left testicle, scrotum, sagittal plane.
The patient was referred to a pediatric facility for further follow-up and treatment, but no further information on his outcomes was available.
Discussion
Testicular microlithiasis is a condition in which microcalcifications composed of hydroxyapatite are located within the lumen of spermatic, or seminiferous, tubules. 7 Seminiferous tubules are a major structural component of a testis, where meiosis takes place, producing male gametes (spermatozoa). Hydroxyapatite is a complex phosphate of calcium that occurs as a mineral and is the chief structural element of a vertebrate bone. In their structure, these microcalcifications resemble the crystal mesh of uricoliths.
The knowledge about TML has been evolving with the advancement of diagnostic technologies. An important milestone in the field of sonography was marked in 1987, when the first sonographic description of TML was introduced by Doherty et al. 1 The interest in TML increased, and through numerous studies in 1990s, TML had been viewed as a precursor and a predisposing factor for testicular germ cell tumors (TGCTs). Early studies associated TML with the development of TGCT in up to 31% of patients. 8 However, in the past decade, additional studies have changed an insight on isolated TML, which in itself is now considered a benign abnormality. It also has been shown to be more prevalent in such ethnic groups as African Americans and Hispanics, with 14% and 8.5% incidence, respectively, but who usually, differently from white men, show a lower incidence of testicular cancer. 3 In a retrospective study of 2266 cases over a period of 11 years by Volokhina et al., 9 87 patients presented with TML (incidence of 3.8%), and 1 had concurrent TGCT. The rest of the 86 patients with isolated TML were followed over a period of 4 years with no TGCT development. Cooper et al. 10 had collected data for over 9 years (2003–2012), in which he studied 3370 boys. Eighty-three patients had TML (incidence of 2%). Six patients with TML were found to have concurrent tumors. Five of six had other premalignant conditions (cryptorchidism in three cases and Peutz-Jeghers syndrome in two cases).
Etiology and Pathogenesis
Understanding the anatomy of a seminiferous tubule is important to understanding the pathological process behind TML. A seminiferous tubule is lined with epithelial cells and contains the basement membrane, sperm cells that differentiate into gametes, Sertoli cells, and the lumen. Sertoli cells are fewer than sperm cells, but their role cannot be underestimated. They provide structural support and nourishment to sperm-producing cells. In addition, Sertoli cells participate in the process of phagocytosis, removing the debris formed during spermatogenesis. It is believed that the dysfunction of Sertoli cells is at the core of TML formation. Accumulation of cellular debris in the tubular lumina occurs, followed by deposition of glycoprotein, which eventually results in dystrophic calcification at its core with concentric rings of glycoproteins surrounding the core of a microlith. 11 In this way, microliths present as laminated calcifications.
However, there is another theory of TML pathogenesis. According to this theory, microcalcifications are located within the testicular stroma in the earliest stages of embryogenesis of the gonads, thereby making it a congenital pathology. According to some authors, there is a genetic predisposition to TML associated with gene mutation.12,13 Furthermore, studies were performed on mice, and the presence of lithiasis in atrophic testes of mice might lead to the pathogenesis explanation of human TML. 14
Signs, Symptoms, and Degrees of Organ Involvement
The diagnosis of TML is not clinical but is usually established following sonographic examination. TML is asymptomatic. It causes no discomfort or pain, does not change the shape of a testis, and is not palpable. Diagnosis of TML is confirmed when a concentration of five or more microliths is seen in a field of view. These calcifications can be diffusely scattered throughout the testis or present as a cluster in a certain area. The latter, however, is a more worrisome finding as it may be signaling the development of carcinoma in situ due to cellular dysfunction in that particular area. 15 Fewer than five calcifications per field of view are termed limited TML. Microcalcifications may be present in one or both testes. Bilateral TML is more common.
Imaging
With the development of high-resolution diagnostic medical sonography (DMS), earlier and more frequent identification of various testicular lesions became available. According to the American Institute of Ultrasound in Medicine (AIUM), 16 indications for DMS scrotal evaluation include scrotal pain; palpable inguinal, intrascrotal, or testicular masses; scrotal asymmetry or enlargement; potential intrascrotal hernias; evaluation of varicoceles; male infertility; follow-up of prior indeterminate findings; localization of nonpalpable testes; detection of occult primary tumors in patients with metastatic germ cell tumors or unexplained retroperitoneal adenopathy; follow-up of patients with prior primary testicular neoplasms, leukemia, or lymphoma; abnormalities noted on other imaging studies (computed tomography, magnetic resonance imaging [MRI], positron emission tomography); and disorder of sexual development (i.e., cryptorchidism). Testicular microlithiasis is often identified as an incidental finding on such examinations.
Sonographic Appearance
Sonographically, microliths appear as tiny calcifications no larger than 3 mm, producing no posterior shadowing. There may be many or a few microliths visualized. If five or more are present on a single image, a diagnosis of TML of a classic type is confirmed. 10 The microliths are spherical or ovoid and are often found bilaterally. They can be diffusely spread throughout the testis or concentrated in one area. Usually, regardless of the number, TML does not produce a mass effect and causes no loss of testicular shape. Finally, microcalcifications are highly echogenic, giving resemblance of what is known in literature as a “starry night” or “snowstorm” pattern. 17
Image Optimization
It is necessary to have proper equipment settings for better visualization, especially in cases of limited TML, where calcifications are fewer than five. A sonographer should aim for a more homogeneous parenchymal imaging by reducing contrast and speckle. This can be achieved through the use of dynamic range increased settings, harmonic imaging, and the use of spatial and frequency compounding. A sonographer should take advantage of high-resolution imaging, using high-frequency linear array transducers of 12 to 15 MHz. The use of multiple focal zones provides equal beam focus distribution.
Treatment and Outcomes
Patients with TML can be divided into two groups: those with TML but without accompanying risk factors for testicular malignancy and others with TML and additional risk factors associated with testicular malignancy. Such classification is important in differentiating patient follow-up regimens and care. Prognosis is favorable for patients with isolated TML, and no treatment or imaging is required. However, treatment and prognosis in patients with TML and additional risk factors will depend on associated diagnoses. Presented risk factors8,18,19 can be divided into the following groups:
Testicular disorders, including cryptorchidism, testicular atrophy, or gonodal digenesis
Orchiopexy, a surgical procedure during which an undescended testicle is moved down into the scrotum; also, a surgery used to resolve testicular torsion
Syndromes including Down, McCune-Albright, Klinefelter, and Peutz-Jeghers
Fertility disorders such as partial or complete infertility
Germ cell tumor as part of the patient’s history or as history in a first-degree relative
Since it was not possible to follow the case discussed earlier, the following hypothesis can be based on the patient’s history and the current understanding of the topic. The common age of a patient’s presentation for evaluation of cryptorchidism is shortly after birth. The average recommended age for orchiopexy, the procedure used to descend a testicle into a scrotum, is 6 to 12 months of age, yet it can be performed later as soon as the diagnosis is made. 20 Possible reasons why this patient’s condition remained untreated include lack of access to medical care, nonpalpable undescended testicle, or acquired undescended (ascended) testicle as differential diagnoses.
Similar reports have been found in literature with successful treatment of cryptorchidism by orchidectomy, histological confirmation of the TML diagnosis, and a more stringent recommendation to follow-up care. 21 Since the patient in this case presented with cryptorchidism, which is a testicular disorder and a frequent risk factor, he should be undergoing a closer follow-up care with annual sonographic examinations and other testing and procedures as pertaining to his condition.
Similarities and Differences in the Follow-up Recommendations
Similarities and differences in the follow-up recommendations for a patient’s care depend on whether TML presents as an isolated entity or if it is accompanied with additional risk factors or associated diagnoses. In Europe and Australia, follow-up recommendations for asymptomatic patients with TML focus on the patient’s education and self-examination. Therefore, according to recently adopted European guidelines to scrotal imaging, sonographic follow-up is not advised in patients with isolated TML.15,22 Similarly, a recent US study by Keenan et al. 23 using a simulated cost-calculating algorithm concluded that sonographic surveillance is costly and nonefficient for such patients. Testicular self-examination is more efficient and thus recommended.
However, the follow-up recommendations for patients with TML and additional risk factors will vary from the recommendations for patients without risk factors. A closer and more detailed follow-up regimen is recommended. Laboratory values for tumor serum chemistry markers should be obtained. Imaging recommendations include annual surveillance with sonography as well as contrast MRI and contrast DMS for determination of hypervascular areas. Finally, interventional procedures such as a biopsy for testing or orchidectomy for tumor removal complete the list of care for patients with TML, who are at higher risk of developing testicular neoplasia. 15
Current Limitations to This Topic
Original research is often focused on either pediatric or adult populations, and therefore the correlation is unclear.
There is a lack of current original research on TML among an adult population.
The duration of the follow-up period varies by study and ranges from 1.5 to 11 years. Therefore, it is not clear which cutoff time to accept when determining the development of neoplasms. It is not clear what the accurate follow-up period is to detect testicular neoplasm development.
Conclusion
On an initial examination, especially with TML as an incidental finding, it is very important to exclude the presence of malignancy as well as to establish a baseline for future patients’ care. Sonography remains the gold standard in the diagnosing of TML, which is often an incidental finding. When evaluating a patient with TML, a sonographer should take into account the patient’s medical history and be aware of any risk factors pertaining to the case. The current thought is that TML in itself is not a risk factor for the development of testicular malignancy but may be associated with testicular neoplasms in patients with testicular disorders, certain syndromes, infertility, and a history of neoplasia. There are follow-up recommendations and guidelines for patients with TML established in Europe; however, there is not an established protocol in the United States. 24
Future research can focus on evaluating therapeutic outcomes and cost-effectiveness of the recently proposed follow-up guidelines in Europe. In addition, research in the field of genotyping and gene mutation as they relate to TML formation12,13 may determine or disprove a cause-effect relationship between TML and TGCT.
Footnotes
Acknowledgements
The author expresses her deep gratitude to El Centro College (Dallas, TX) Diagnostic Medical Sonography Program and Lynn Schluns, BS, RDMS, RVT, for her tireless revision of this work; Pam Crawford, RDMS, RVT, for her assistance in obtaining the case study; Ashley Berry, RDMS, RVT, for her mentorship; and Texas Health Resources Ultrasound Department (Dallas, TX) for their dedication to the field of sonography by helping turn students into a new generation of professionals.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.