
Abstract
Different types and locations of choroid plexus cysts (CPCs) have been described, including oversized and bilateral. It appears that the type, size, and number of CPCs are correlated with various degrees of aneuploidy risk. This report deals with the natural history and significance of CPCs filling only one choroid plexus. Multiple CPCs filling the entire choroid plexus were detected in 9 of 4211 consecutive second-trimester sonographic examinations. Karyotyping via amniocentesis or neonatal blood analysis was performed in all cases. CPCs in a single choroid plexus were associated with transient ventriculomegaly in five of nine fetuses. Resolution of CPCs took place between 25 and 33 weeks of pregnancy, with most resolving after the 30th week. Karyotyping revealed normal results in all cases. Favorable prognosis of newly described multiple CPCs in a single choroid plexus should be mentioned during patient counseling.
Choroid plexus cysts (CPCs) result from the entrapment of cerebrospinal fluid within tangled villi of the fetal ventricular system. 1 CPCs gain importance because of their probable association with fetal aneuploidy and particularly with trisomy 18. 2 Some reports have also associated CPCs with trisomy 21. 1 Despite numerous research efforts, a clear-cut management protocol for fetuses with isolated CPCs has not emerged. Although some authors strongly suggest an amniocentesis when CPCs are present, 3 others recommend karyotyping, but only when CPCs are associated with other structural anomalies. 4 Different types of CPCs have been described, including large sized, bilateral, and multiple, among other presentations.1–3 It appears that the type and especially the size of CPCs are correlated with chromosomal abnormalities.1–4 This report deals with the description, natural history, and prognostic significance of another kind of CPCs: multiple cysts filling a single choroid plexus. A computer-assisted PubMed search of this topic failed to find any description of this entity.
Materials and Methods
Multiple CPCs in a single choroid plexus were defined as two or more cysts in one choroid plexus and the normal appearance of a contralateral choroid plexus (Figure 1). Multiple CPCs were identified in 7 of 2917 consecutive second-trimester sonographic examinations performed between January 2015 and April 2018. The Institutional Review Board approved this retrospective review.

Demonstration of multiple choroid plexus cysts in a single choroid plexus.
Results
The age of the mothers, whose fetuses were diagnosed with multiple CPCs in a single choroid plexus, varied between 28 and 39 at the time of examination (mean, 34.6). The maternal body mass index was between 24 and 30 kg/m2 (mean, 27.4 kg/m2). The ranges, prevalences, and means of sonographic data were used for statistical analysis.
The number of CPCs was as follows: between two and three CPCs in a single choroid plexus in four fetuses, between four and five CPCs in two fetuses, and five CPCs in one fetus. The size of CPC varied from 0.8 mm to 4 mm (mean, 1.6 mm). Unilateral ventriculomegaly was the most common finding associated with multiple CPCs in a single choroid plexus (four of seven cases). Ventriculomegaly was detected within 1 to 2 weeks after the CPCs diagnosis (Figure 2). Patients with CPCs were subjected to sonographic examinations every 2 weeks for as long as abnormalities (CPCs, ventriculomegaly) were present. Ventriculomegaly resolved by the time of birth in all cases. Clinical characteristics of the fetuses affected by multiple CPCs in a single choroid plexus are presented in Table 1.

Mild ventriculomegaly associated with the appearance of choroid plexus cysts.
Natural History and Associated Anomalies in Fetuses With Multiple Choroid Plexus Cysts (CPCs) in a Single Choroid Plexus.
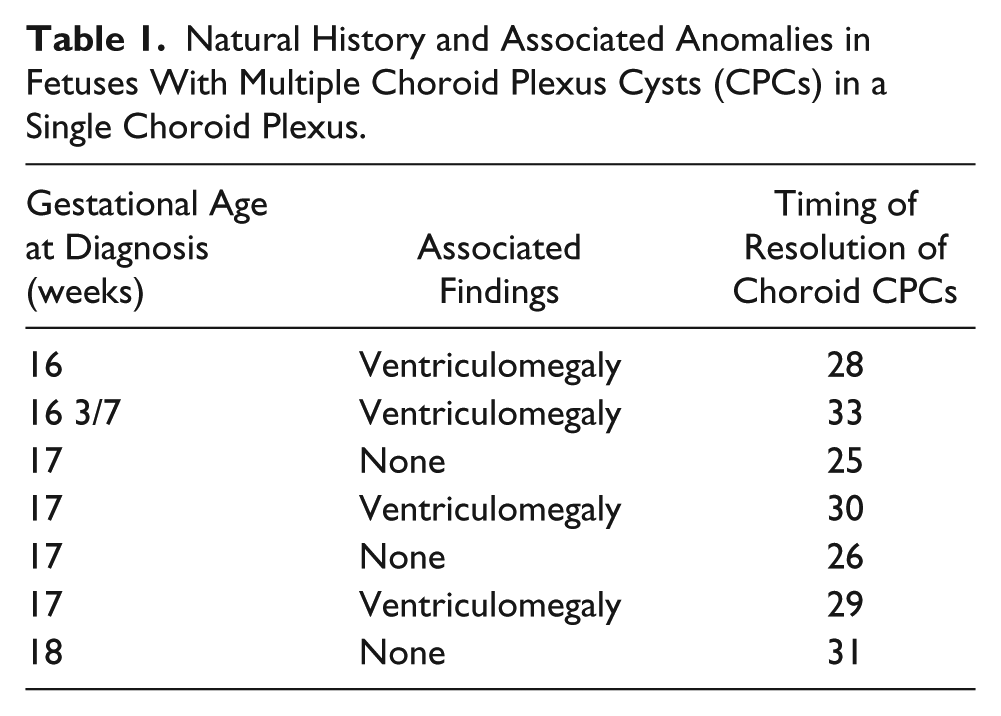
Karyotyping was performed with an amniocentesis in three of the cases and by testing neonatal blood in four cases. All fetuses and neonates were euploid.
Discussion
In the second trimester, CPCs are found in 1% to 3% of euploid fetuses and in 30% to 50% of those with trisomy 18.5–7 Whenever a CPC is detected, the patients’ genetic counseling includes the discussion of its significance and need for an amniocentesis.
Chromosomal abnormalities, specifically trisomy 18, should be ruled out if the CPCs are larger than 1 cm, bilateral, or irregular in shape. 3 In cases of a single CPC, abnormal karyotypes were detected in 3.59%; in cases of multiple CPCs in both choroid plexuses, they were detected in 3.93%. 3 The risk of trisomies was 2.05% (trisomy 18 in 1.54% and trisomy 21 in 0.26%) Each trisomy 18 occurred in cases of CPCs measuring more than 7 mm, and most cases of trisomy 18 (83.3%) were detected when a CPC was larger than 1 cm. Fernandez Alvarez et al. 7 performed a meta-analysis that included 22 original reports of various types of CPCs. Ten of these were prospective case series, 11 were retrospective case series, and 1 was a meta-analysis. These authors concluded that there is a statistically significant correlation between the presence of multiple CPCs in both choroid plexuses and chromosomal anomalies and congenital infections. There was a difference in the sensitivity, specificity, and negative and positive predictive values for different types of CPCs. The presence of bilateral CPCs irrespective of their number and size had the highest sensitivity and most negative predictive value for congenital infection or genetic disorders (88% and 94%, respectfully). Bilateral multiple CPCs had the highest likelihood for chromosomal anomalies. A unilateral single CPC had the lowest likelihood ratio for congenital infection. 2 A computer-assisted PubMed search failed to detect any description of multiple CPCs located in a single choroid plexus. It appears that multiple CPCs can contribute to an increased ventricular width, causing transient ventriculomegaly. We postulate that this may be caused by a blockage of foramina within the ventricular drainage system of the central nervous system, which can lead to the expansion of the ventricles, compressing the brain (the cranial cavity cannot expand to accommodate the increase in fluid volume). Resolution of CPCs is associated with resolution of ventriculomegaly. Similar findings were described by Pascual-Castroviejo et al. 8 in cases of multiple CPCs in both choroid plexuses. Multiple CPCs in a single choroid plexus seem to resolve at a later date compared with the other types of CPCs, which usually disappear by 26 to 28 weeks of gestation. 7
Conclusion
In this case series, multiple CPCs filling a single choroid plexus were not associated with abnormal fetal karyotype and therefore carry favorable prognosis. These data may be helpful when counseling patients with this unusual appearance of CPCs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.