
Abstract
Introduction:
While perceived as safe, diagnostic ultrasound has the potential to cause biological effects on the body tissues. The aim of this study was to evaluate knowledge, attitudes, and practices of Australasian sonographers on bioeffects and safety of ultrasound scanning.
Methods:
Focus groups were used to develop a questionnaire to explore knowledge, attitudes, and practices of ultrasound safety, which was then distributed to Australasian sonographers. Thematic (focus groups) and descriptive (questionnaires) analyses were undertaken.
Results:
A 37-item questionnaire addressed knowledge, attitudes, and practices of ultrasound safety. In 47 collected responses, sonographers demonstrated good familiarity of thermal index (TI) (79%), mechanical index (MI) (68%), and “as low as reasonably achievable” (ALARA) principle (85%). However, most sonographers could not accurately define TI (13%) and had poor knowledge of safety guidelines relating to TI (19%) and MI (14%). Over 30% were uncertain about their attitudes to ultrasound safety issues. While 52% always and 30% most of the time adhere to ALARA, 37% of sonographers reported never monitoring TI and MI.
Discussion:
While familiar with safety terms, knowledge of safety guidelines was lacking. Many sonographers were uncertain about their attitudes to the safety of scans, and safety practices involving monitoring for bioeffects were not a high priority.
Keywords
Introduction
Ultrasound does not expose patients to ionizing radiation and is perceived by many to be safe. 1 However, ultrasound does have the potential to cause biological effects (bioeffects) on the body’s tissues. 2 While studies conducted on humans have failed to provide evidence of ultrasound exposure causing tissue damage, evidence from more recent animal studies has demonstrated that ultrasound applied under similar conditions to those used in humans can cause adverse bioeffects. 3 Bioeffects are the mechanisms by which ultrasound may damage biological tissue and are divided into two groups: thermal effects and mechanical effects. 4
Thermal effects occur when ultrasound energy interacts with biological tissue. The resultant absorption and conversion of ultrasound energy to heat causes increased tissue temperatures.1,5 If the temperature rises above an optimal point, cell death may occur. 6 The thermal index (TI) measures the ratio of the output of acoustic power to the power needed to elevate the tissue temperature by 1°C. Three thermal indices are used: TIS for soft tissue, TIB for bone, and TIC for cranial bone.
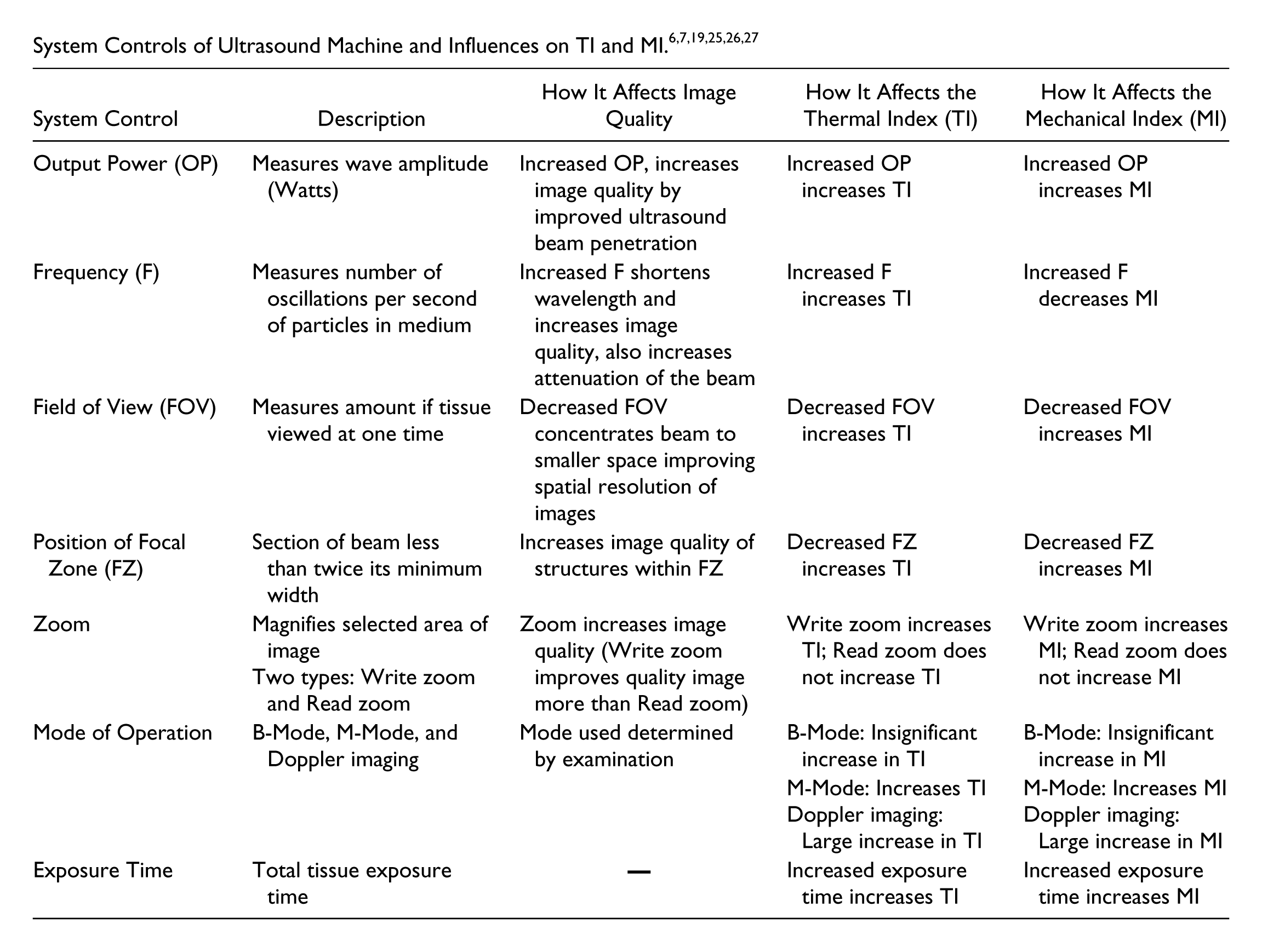
Mechanical effects may cause cavitation due to formation of gas bubbles within a liquid that then alter in size (expand, contract) in response to changes in pressure in the ultrasound wave. 7 The mechanical index (MI) provides an indication of the likelihood of mechanical effects occurring. Factors related to controls on the ultrasound machine affecting TI and MI can be seen in the Appendix.
The likelihood of a bioeffect occurring is directly related to the acoustic output delivered by the ultrasound machine; the upper limit possible from the machine is set by the manufacturer. 8 Regulation of safe upper limits of the acoustic output for different ultrasound examinations ranging from 94 mW/cm2 to 720 mW/cm2 was commenced by the Food and Drug Administration (FDA) in 1976. 9 With advances in ultrasound technology, manufacturers and users requested the removal of acoustic output limits; in 1992, the FDA removed all examination-specific limits and increased the upper limit to 720 mW/cm2 (Table 1) for all examinations except ophthalmic. 8
Maximum Acoustic Output Limits for Various Examinations in 1976 and 1992. 8
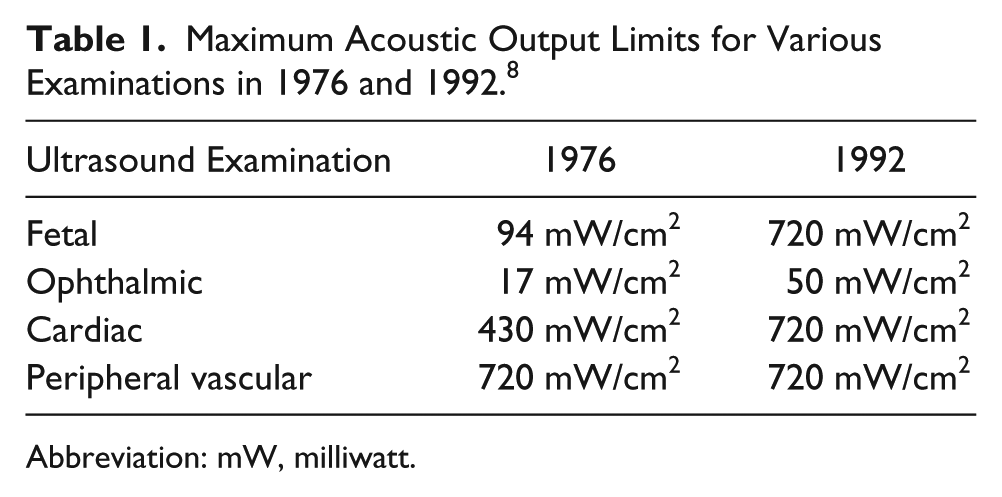
Abbreviation: mW, milliwatt.
As a condition of these increases, the American Institute of Ultrasound in Medicine (AIUM) and National Electric al Manufacturers Association (NEMA) introduced the Output Display Standard (ODS); the ODS states that all machines capable of producing these higher acoustic output levels must display on the machine an indication of the potential for ultrasound induced bioeffects to occur. 10 The two displayed indices are the TI and MI. Their location on the screen of a Phillips IU22 machine can be seen in Figure 1. With the TI and MI now displayed on the ultrasound machines, it is considered the responsibility of the practicing sonographer to monitor these indices during an ultrasound examination. 11

Typical ultrasound machine display screen. The numerical displays of the thermal and mechanical indices are seen within the red circle.
While ultrasound bioeffects are taught as part of the ultrasound curriculum in Australia, concerns have been raised about the current knowledge of sonographers relating to bioeffects, their attitudes toward these. and the practices of sonographers in monitoring the TI and MI during ultrasound examinations. 8
To investigate previous studies that have examined knowledge attitudes and practices related to ultrasound safety, a systematic scoping review of the published literature was undertaken (CINAHL, EMBASE, Medline, Scopus, PubMed, Cochrane, Google Scholar to June 19, 2016). Of the 10 primary studies found, all reported on knowledge, including knowledge of TI and MI, bioeffects, the “as low as reasonably achievable” (ALARA principle), and safety guidelines. Eight reported on practices, centered on monitoring of TI and MI, and only three addressed attitudes, related to safety aspects in obstetric ultrasound examinations (Table 2). There was one pre-post study and nine cross-sectional studies.
Studies Assessing Sonographers’/Ultrasound Users’ Knowledge, Attitudes, and Practices of Ultrasound Safety. a
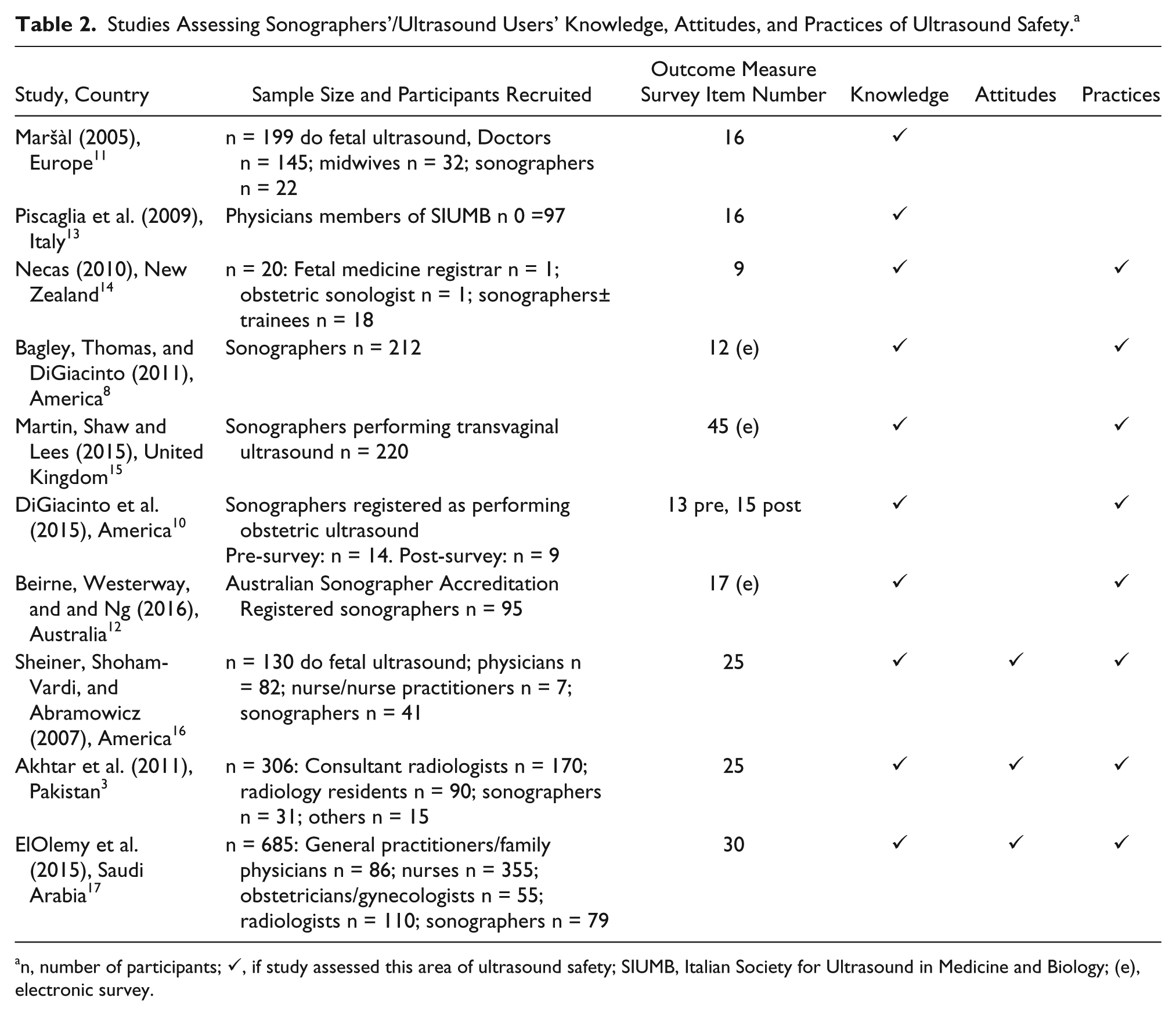
n, number of participants; ✓, if study assessed this area of ultrasound safety; SIUMB, Italian Society for Ultrasound in Medicine and Biology; (e), electronic survey.
Beirne et al. 12 was the only study conducted on Australian sonaographers; the majority of items assessed sonographers’ knowledge and practice mostly pertaining to obstetric examinations, and no items addressed attitudes to ultrasound safety. A greater understanding of Australasian sonographers’ knowledge, attitudes, and practices in regards to all ultrasound examinations is clearly needed to guide future education about safe application of ultrasound scanning.
The aim of this study was to investigate knowledge, attitudes, and practices of Australasian sonographers on the bioeffects and safety implications of ultrasound exposure.
Methods
Institutional ethics approval was granted prior to commencement of the study. A survey about knowledge, attitudes, and practice of ultrasound examinations was developed using two focus groups: four qualified, practicing sonographers with an average of 18.5 years of experience in one group and another with two student sonographers. Applying a qualitative descriptive approach, discussions relating to semi-structured questions about the safety of ultrasound exposure and broader safety issues were recorded, transcribed, and analyzed using thematic analysis to develop common themes. 18 The developed survey was built around three final themes with the items aiming to accurately capture sonographers’ knowledge, attitudes, and practices of ultrasound safety, thus providing face and content validity. A 30-item knowledge, attitudes, and practices survey (with an additional seven demographic items) was developed. No reliability testing of the survey was undertaken.
A cross-sectional study using the survey delivered electronically (Survey Monkey) and anonymously was then undertaken between October 2015 and April 2016. Participants were provided with an information sheet on the first page of the e-survey and informed that submission of the survey was an indication of consent. Recruitment was conducted through the Australasian Sonographers Association (ASA) and the Australasian Society of Ultrasound in Medicine (ASUM), who provided nonidentifiable links to the survey, which were also provided in newsletters and Facebook pages. Hard copies of the survey and information sheet were also taken to an ASUM workshop.
Statistical Analysis
Data were extracted directly from Survey Monkey into the SPSS 23 statistical package. Descriptive analysis was used to analyze the responses to the survey. This included counts and percentages for categorical variables and means and standard deviations for continuous variables.
Results
Participants
There were a total of 52 responses to the survey (43 electronic, 9 hard copy). Five responses were excluded (n = 4 no answers, n = 1 completed a second survey). Table 3 summarizes the demographic information of the 47 sonographers included in the analysis. There were 4 (9%) student sonographers, 6 (13%) sonographers with less than five years’ experience, 8 (17%) sonographers with 5 to 10 years of experience, and 29 (61%) sonographers with greater than 10 years of experience. Additionally, 10 (21%) participants identified themselves as tutor sonographers and 6 (13%) as university lecturers.
Demographic Information of Sonographers.
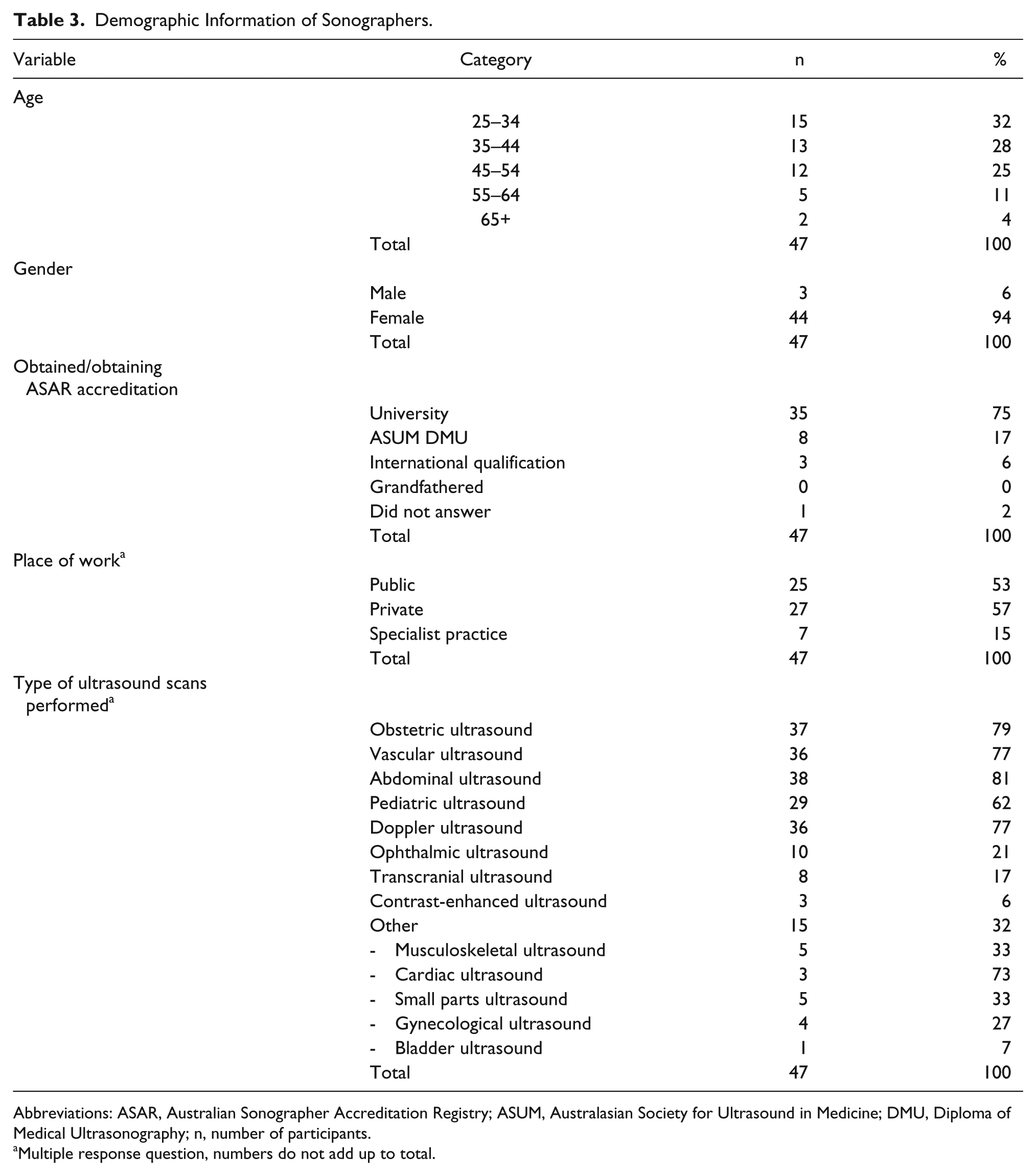
Abbreviations: ASAR, Australian Sonographer Accreditation Registry; ASUM, Australasian Society for Ultrasound in Medicine; DMU, Diploma of Medical Ultrasonography; n, number of participants.
Multiple response question, numbers do not add up to total.
Knowledge Items
Sonographers’ knowledge of ultrasound safety is shown in Tables 4 and 5. While most sonographers were familiar with and understood acronyms for TI and MI, fewer knew the three thermal indices, very few had a detailed understanding of the TI or knew the WFUMB recommendations for limits to TI and MI (Table 4). Furthermore, only 13% of sonographers correctly answered the open-ended item (Item 3) where sonographers were asked to define the meaning of TI. The majority of sonographers knew when to adhere to the ALARA principle and monitor TI and MI, but a relatively small percentage knew that the FDA changed the output power of ultrasound machine in 1992.
Sonographers’ Responses to Multiple Choice and Open-Ended Knowledge Items.
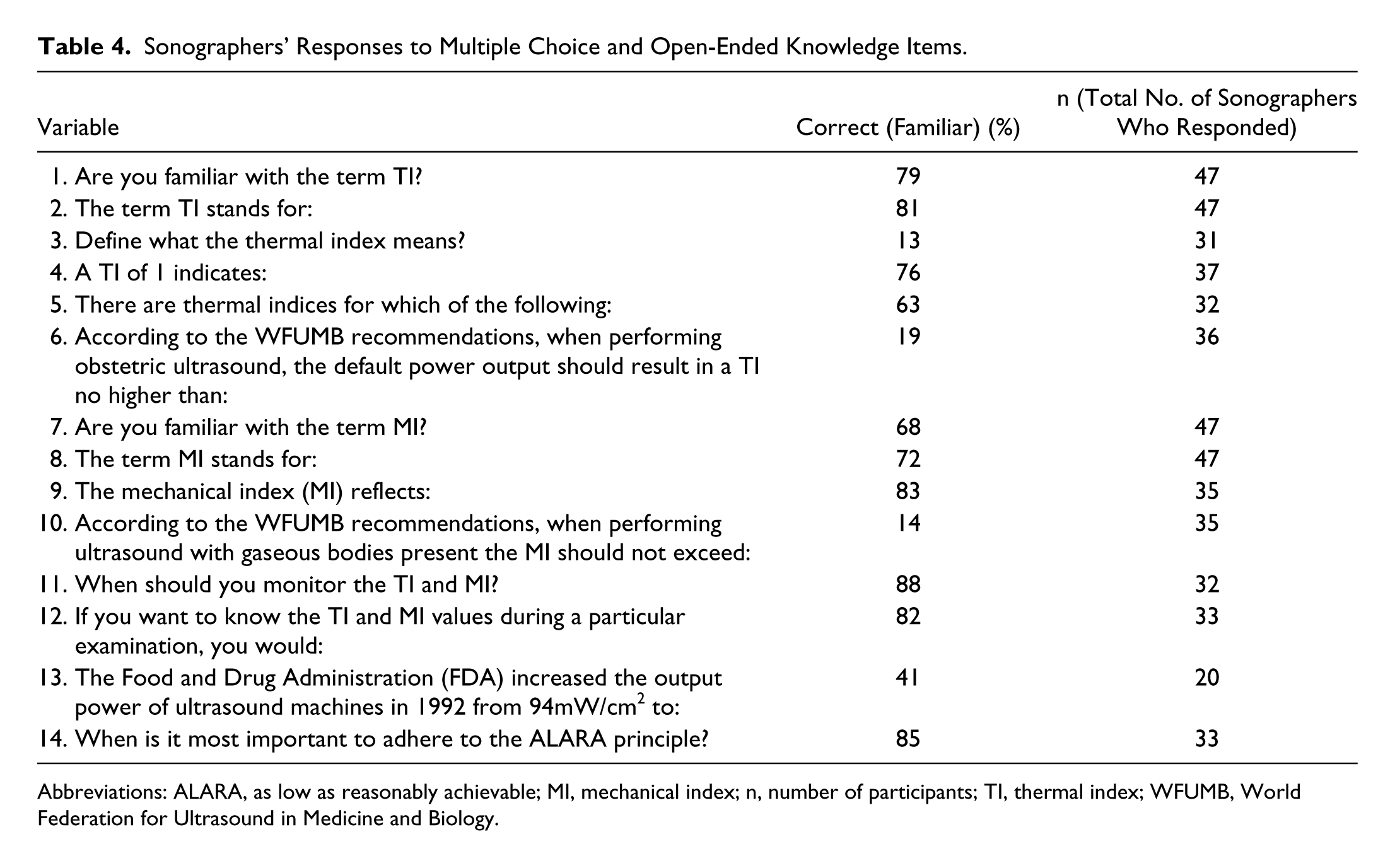
Abbreviations: ALARA, as low as reasonably achievable; MI, mechanical index; n, number of participants; TI, thermal index; WFUMB, World Federation for Ultrasound in Medicine and Biology.
Knowledge of Factors That Reduce TI and MI. a
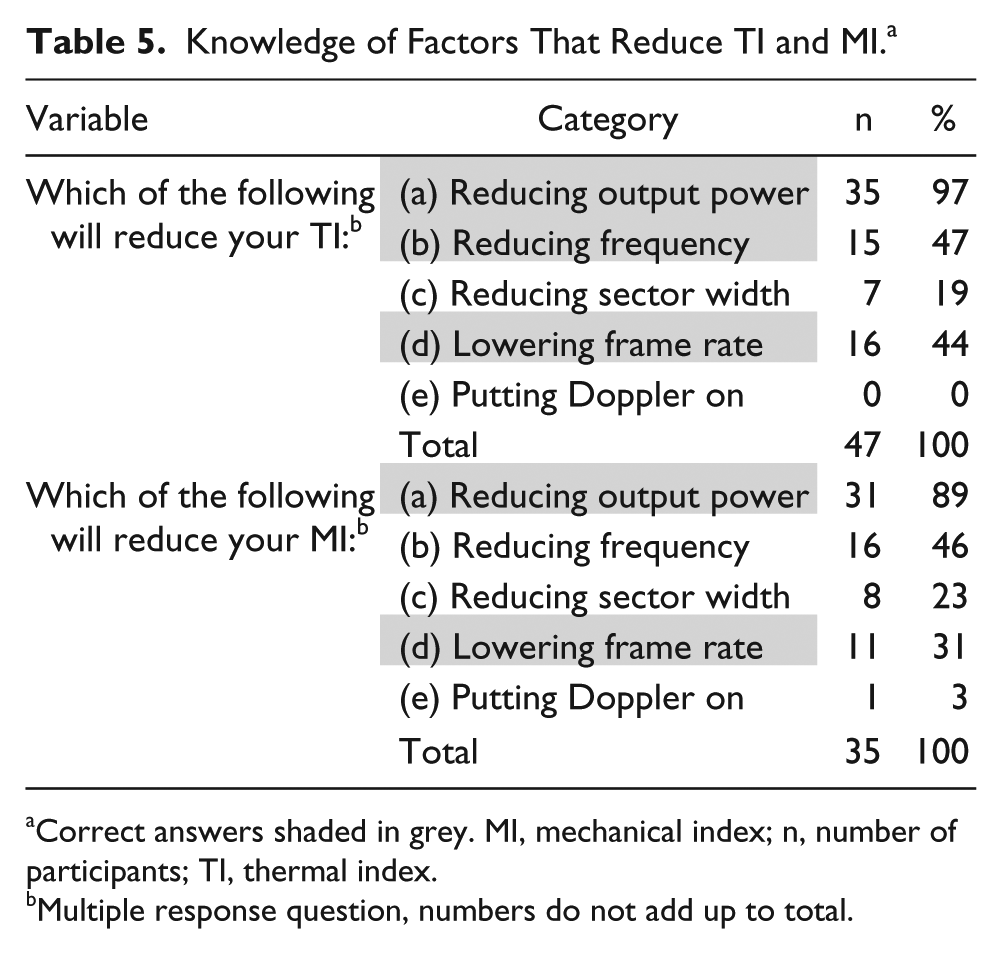
Correct answers shaded in grey. MI, mechanical index; n, number of participants; TI, thermal index.
Multiple response question, numbers do not add up to total.
Results in relation to sonographer’s knowledge of factors that reduce the TI and MI are shown in Table 5, with correct answers shaded in grey. Of the 36 sonographers who responded to the TI question, the three correct answers were given by 97%, 47%, and 44% of sonographers, respectively. For reducing MI, the correct answers were given by 89% and 31% of sonographers, respectively.
Attitudes Based Items
There were 16 (34%) sonographers who were “unsure” about their attitudes toward ultrasound safety for obstetric and nonobstetric patients (Figure 2). The concern was rated as appropriate by 43% of sonographers for nonobstetric ultrasound and by 28% for obstetric ultrasound. There were 10 (21%) sonographers who considered ultrasound safety concerns for obstetric patients to be moderately underrated.
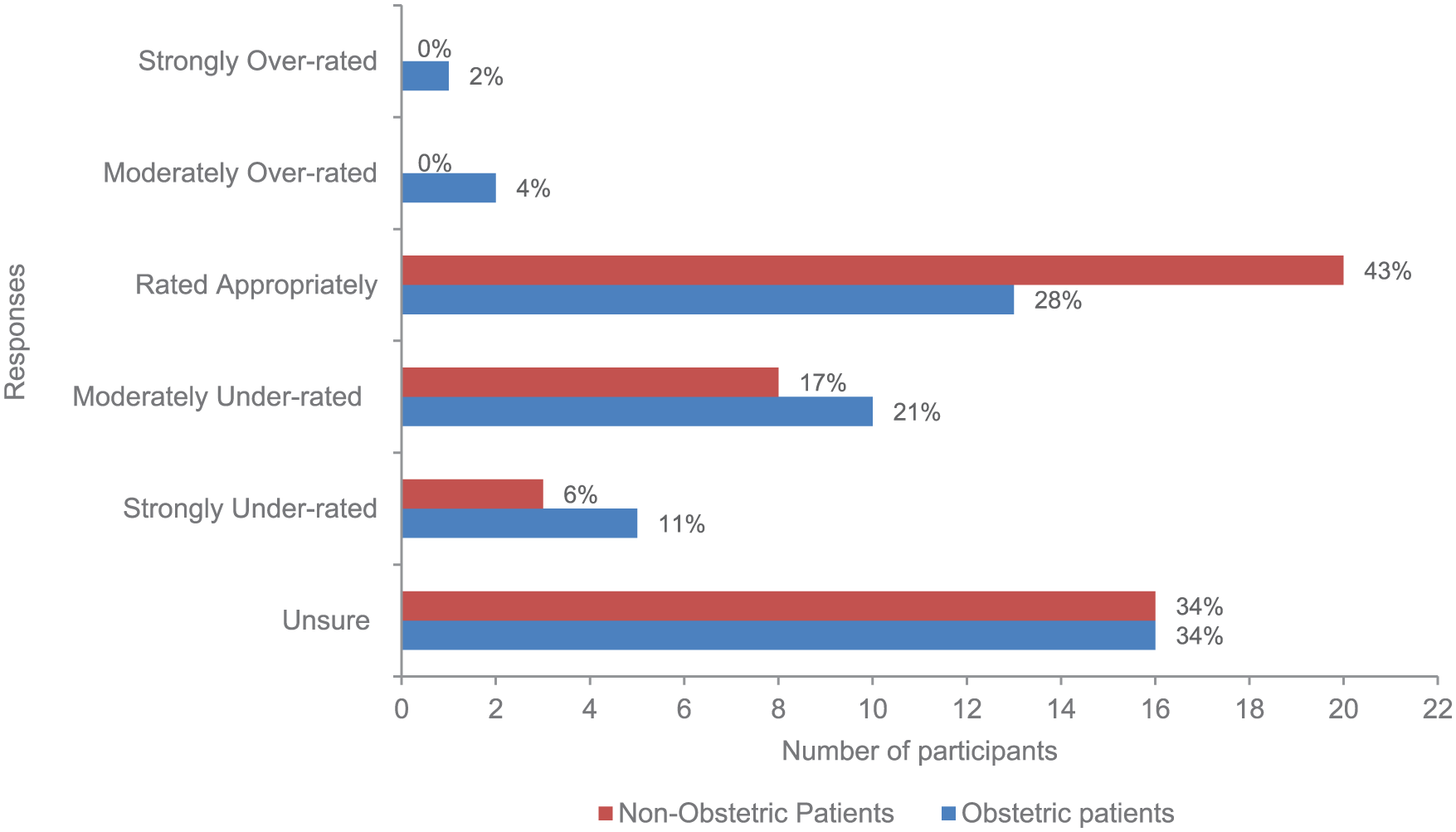
Sonographers’ attitudes toward ultrasound safety for obstetric and nonobstetric patients.
No sonographers believed the use of Doppler ultrasound in the first trimester is perfectly safe, with a similar spread between those believing it should only be used when medically indicated (34%) or for medical reasons (32%) and those who were unsure (34%). Sonographers’ attitudes toward use of Doppler ultrasound in early trimester scans for checking ductus and middle cerebral artery (MCA) were mixed: 9 sonographers (19%) believed that Doppler should be performed when requested by the doctor, 22 (47%) were unsure, and there was an even split of those who believed it should (17%) and should not be performed (17%) at all.
In relation to ultrasound safety equipment training, 19 (40%) sonographers believed and 4% did not believe that it was important to have up-to-date training on the thermal and mechanical effects when a new piece of ultrasound equipment is installed. When asked, 93% of sonographers reported no provision of training with new equipment. Regarding topics likely to be attended at conferences, 12 (25%) would choose an obstetrics presentation, 15 (32%) a musculoskeletal presentation, and 4 (9%) sonographers would choose a bioeffects presentation while 34% were unsure.
Practice Items
Sonographers’ adherence to ALARA and monitoring of TI and MI during examinations is seen in Figure 3. While 52% always adhere to ALARA, only 3% always and 37% never monitor TI and MI. Sonographers were also asked to indicate the examinations in which they monitor TI and MI. Most sonographers monitored the TI and MI during obstetric scans (40%), and the least monitor musculoskeletal (14%) and cardiac (10%) scans; monitoring of TI/MI for vascular, neonatal head, and abdomen were undertaken 29%, 25%, and 19%, respectively.
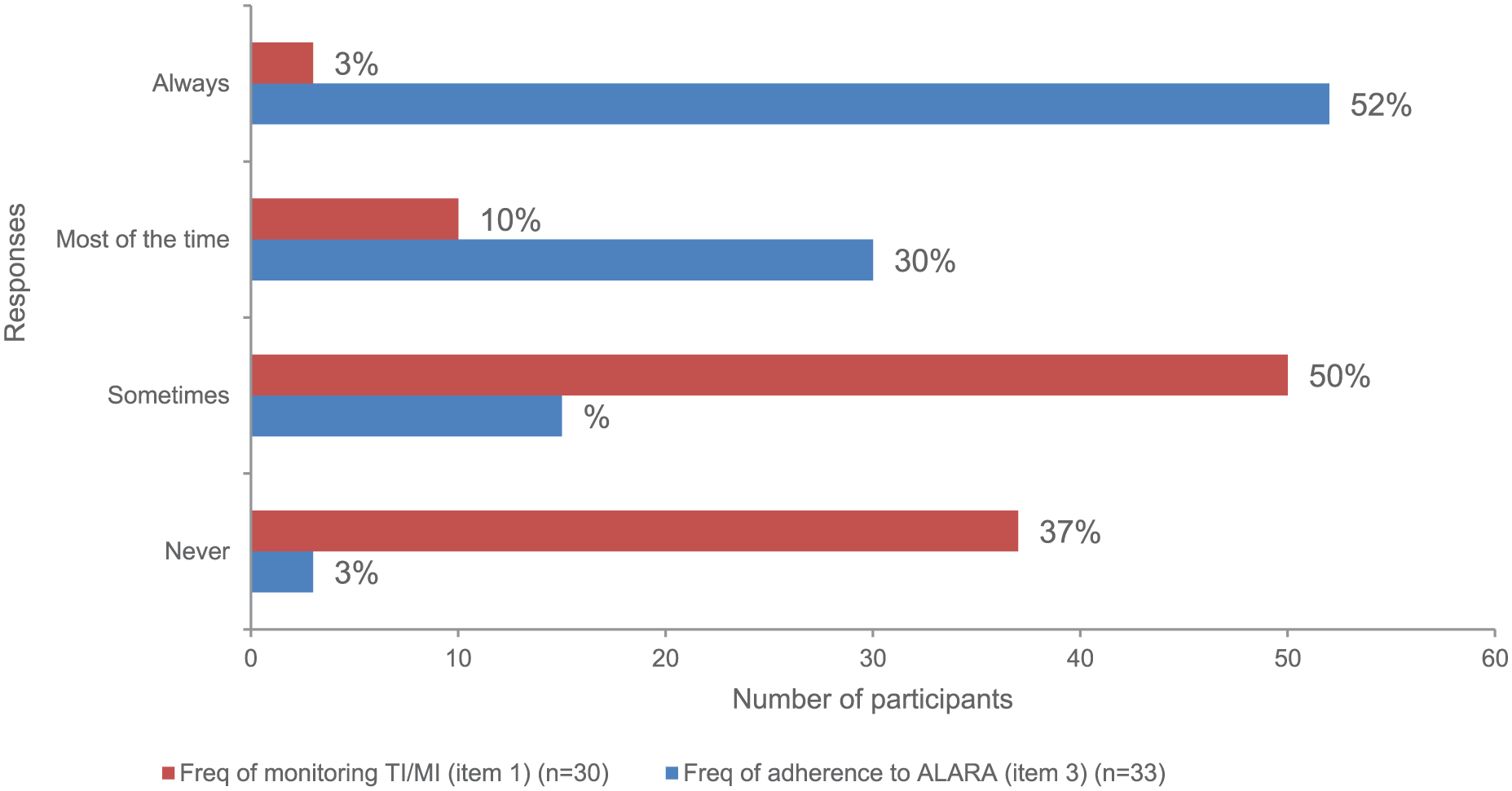
Frequency of monitoring TI/MI and of adherence to ALARA.
Sonographers were assessed on how they adhere to the ALARA principle; of the 29 who responded, 20 (43%) reduce the scan time as much as possible, 7 (15%) adjust the scan parameters to reduce the TI and MI, 1 sonographer constantly monitors TI and MI, and 1 sonographer checks the TI and MI levels on the preset.
Figure 4 shows how often sonographers perform Doppler examinations for obstetric scans in relation to a provided list; 17 (61%) performed Doppler ultrasound for the third and/or second trimester scans, with 11% never using Doppler and 11% only when requested.
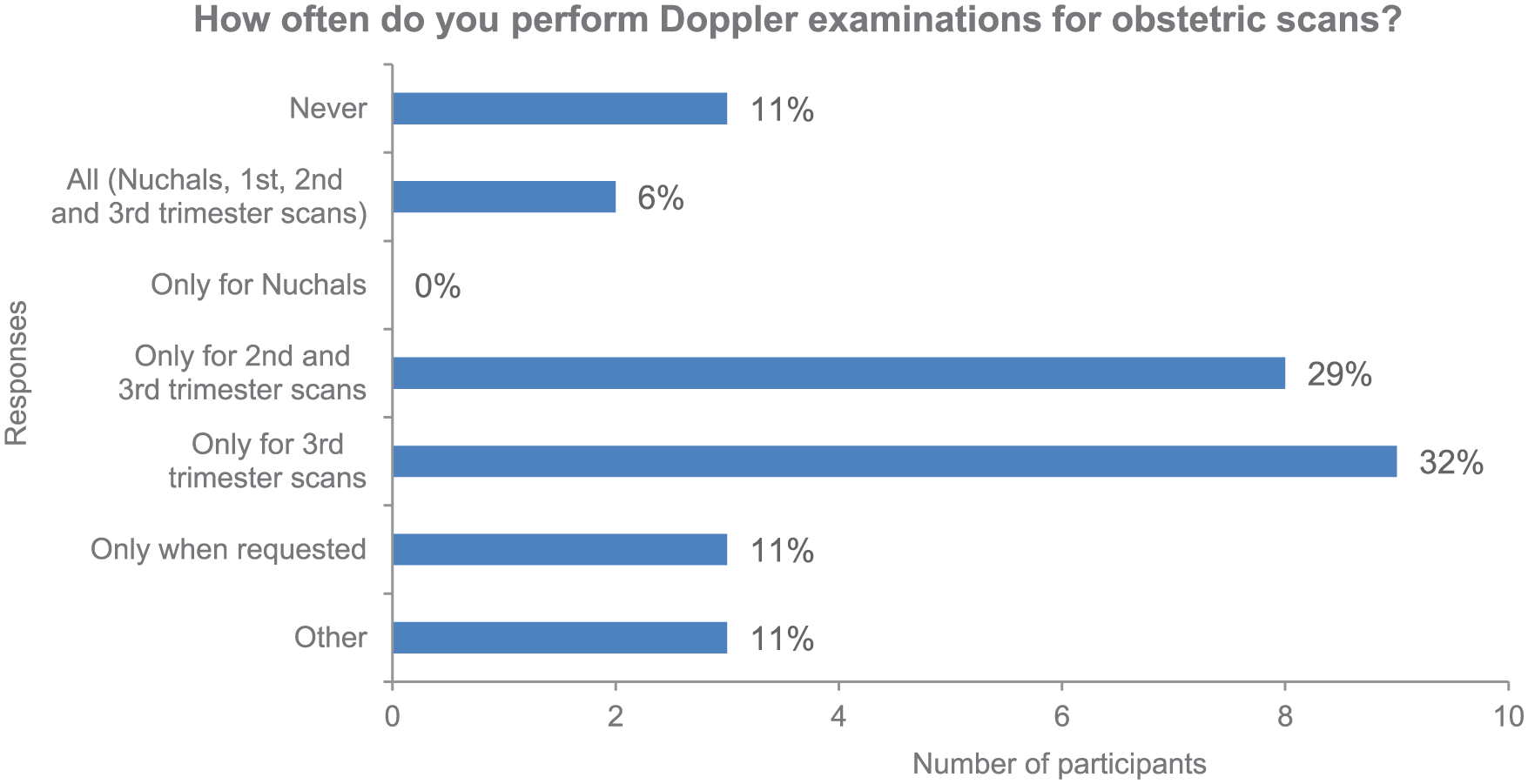
Obstetric scans where sonographers perform Doppler ultrasound.
Sonographers were then asked to rank five factors that are part of all ultrasound examinations with a score of one being most important and a score of five being least important. Figure 5 shows the average score sonographers gave for each factor. Sonographers believed that acquiring all images needed to assess patient was the most important factor of an ultrasound examination, and the TI and MI were the least important factors.
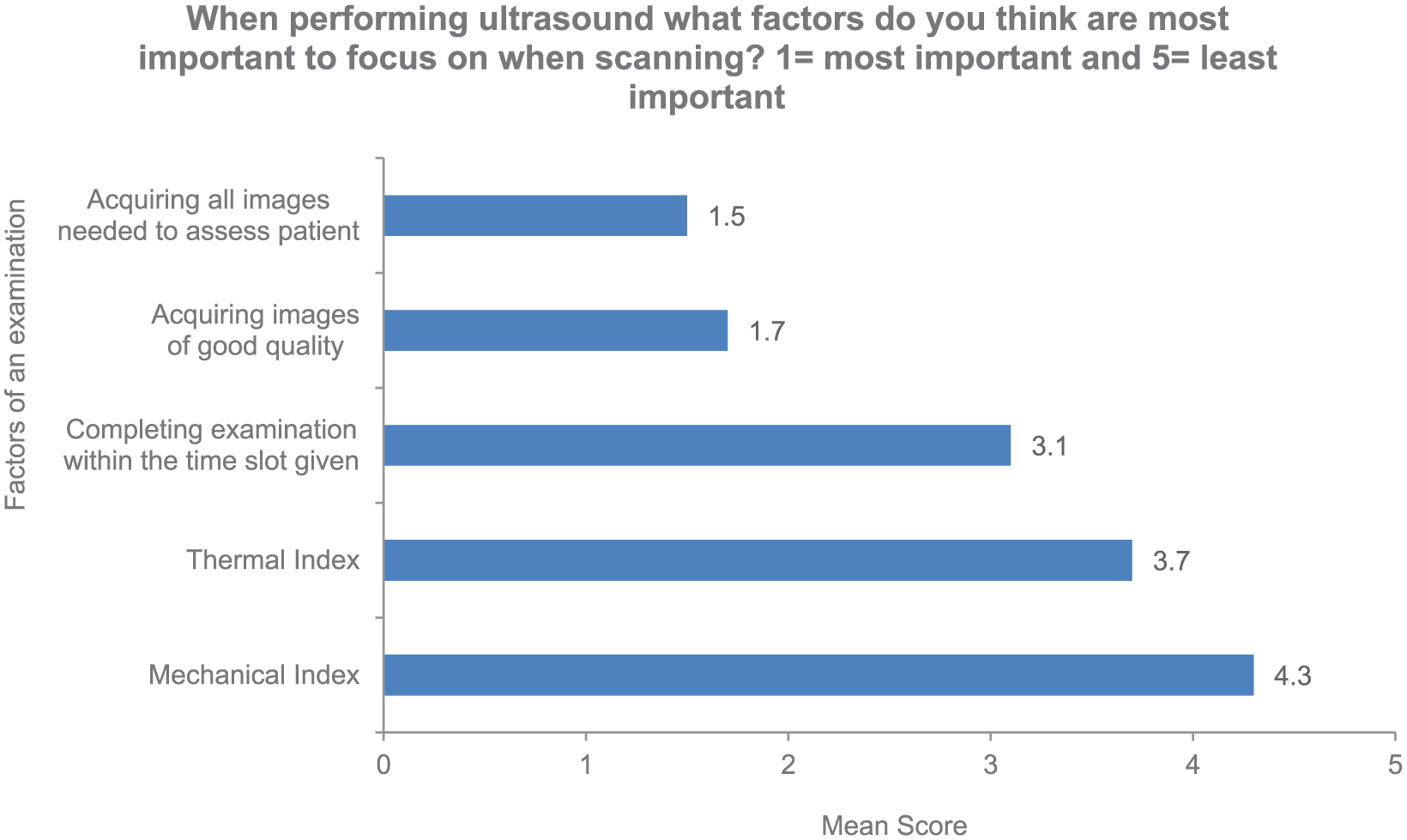
Important factors during an examination.
In the open-ended item, steps most commonly reported by sonographers to reduce the potential for bioeffects were decreasing various scanning parameters (output power, sector width, depth, frequency, gain), limiting the amount of Doppler used, adhering to the ALARA principle, and monitoring TI and MI.
Discussion
Key Findings, Strengths, and Limitations
The aim of the study was to assess the knowledge, attitudes, and practices of Australasian sonographers on the bioeffects and safety implications of ultrasound exposure. Few previous and no other Australian study has assessed attitudes. A further strength of the study was the use of a survey with face and content validity; however, the lack of reliability testing and criterion validity of the survey and the poor recruitment are limitations. The key findings suggest that Australasian sonographers have a strong familiarity with the terms associated with ultrasound and of the ALARA safety principle but few understand the WFUMB guidelines for safe TI/MI limits or knew the 1992 FDA acoustic output levels changes. Attitudes suggested most concern toward ultrasound safety in obstetric scans with uncertainty about safety for nonobstetric scans. Practices to monitor bioeffects were not a high priority overall but most commonly undertaken during obstetric scans. There was strong adherence to ALARA particularly by reducing scanning times rather than adjusting scanning parameters. Overall, the quality and comprehensiveness of the ultrasound images was a more important focus to respondents than measures to monitor potential bioeffects.
Comparison With Previous Studies
Items relating to knowledge, attitudes, and practices of ultrasound varied in the focus of the items and in their format. This made comparisons difficult.
Knowledge of Ultrasound Safety
All 10 studies found in a systematic search reported on aspects of knowledge (Table 2). Comparing well with the current study findings, in 5 of the 10 studies, <50% of participants were familiar with TI and MI and even less could accurately describe them. The Australian study by Beirne et al., 12 which was conducted at a similar time to the current study, recruiting from the same population, but with a larger sample size (n = 97 vs n = 47), reported greater familiarity with the term TI. Piscaglia et al. 13 reported that only 35% of participants knew what a TI of two indicated; in the current study, 13% could correctly define that a TI of 1 was associated with a 1° temperature rise in the tissue.
Poor knowledge of ultrasound safety statements/guidelines in the current study compared similarly to findings in Beirne et al. 12 and Piscaglia et al., 13 where familiarity with local guidelines (EFSUMB, ASUM) was 32% and 49%, respectively. In Piscaglia et al., 13 72% of participants, all physicians, knew the acoustic limits implemented by FDA, while this was correctly answered by only 41% of participants in the current study. DiGiacinto et al. 10 in a small sample (n = 15) of sonographers registered as performing obstetric ultrasound, 83% knew the BMUS recommended TI for obstetric examinations, while the current study reported 19% could correctly specify the WFUMB recommended upper limit.
Attitudes Toward Ultrasound Safety
Three previous studies3,16,17 assessed ultrasound users’ attitudes toward ultrasound safety, but all focused on obstetric ultrasound compared to the obstetric/nonobstetric combination in the current study. It may therefore not be surprising that a comparable question across the four studies related to attitudes toward Doppler use in the first trimester was more confidently answered by those studies with 19% to 37% of participants believing Doppler ultrasound in first trimester is “perfectly safe”; in the current study, a much higher percentage of participants were “unsure” of their beliefs about this, but reassuringly, no reported participant reported first trimester ultrasound to be “perfectly safe.” Interestingly, Akhtar et al. 3 and Sheiner et al. 16 reported that when compared to participants who believe there should be no limits on ultrasound examinations performed in low-risk pregnancies, those who believe there should be limits had higher knowledge of safety aspects.
Practice of Ultrasound Safety
The findings in the current study in relation to practices of monitoring TI and MI mirrored those of previous studies where this was assessed.8,12,15 Compared to the current study reporting 37%, the Australian study 12 reported that 51% of participants never monitor TI and MI during an ultrasound examination. In relation to examinations on which TI/MI are monitored, there were 19% who only monitor for obstetrics in Beirne et al. 12 compared to 40% in the current study. In Necas, 14 90% reported adhering to ALARA, compared to 63% who either always, most of the time, or sometimes adhere to ALARA in the current study. In relation to practices to reduce potential bioeffects, in Martin et al. 15 for transvaginal ultrasound (only) 14% of participants reported changing scanning parameters due to the TI/MI display. In the current study, only 3 participants mentioned that they would reduce the TI/MI and 18 participants would reduce scan parameters such as Doppler, frequency, and scan time to reduce potential risk of bioeffects. Regarding the use of Doppler ultrasound for obstetric examinations, Beirne et al. 12 reported 23% who never use Doppler for nuchals and 46% who never use it at all. In the current study, sample size, specific education, and training may explain the difference but in neither study were the samples sufficiently representative of the population to provide a confident reason. Similar percentages reported adherence to the ALARA principle in Necas 14 as found in the current study.
Dichotomy Among Knowledge, Attitudes, and Practice
Familiarity, ability to describe, TI and MI, and knowledge of where TI and MI are found during an ultrasound examination were “knowledge” questions commonly included across previous studies. In general, those with greatest familiarity had best knowledge of the location of TI and MI during an ultrasound examination. However, knowledge does not appear to translate to practices, with more than half of the participants in three previous studies8,12,15 and an even lower 37% in the current study not monitoring TI and MI.
Attitudes may also be linked to practices. In the current study where 100% of participants did not consider Doppler ultrasound to be perfectly safe in the first trimester, it was interesting to note that only 60% of those same sonographers monitored the TI and MI most or some of the time, and 3% always monitored TI and MI. Furthermore, only 40% believed training in thermal and mechanical effects was important.
Use of ALARA reportedly adhered to by 52% of participants in the current study was also claimed as a means to reduce the potential for bioeffects occurring during obstetric examinations; however, there was disparity between the frequency of monitoring TI and MI (37% never monitor) and beliefs about the importance of monitoring (88% stated monitoring is required during all ultrasound examinations). In addition, sonographers ranked TI and MI as the least important of five factors of the ultrasound examination.
The ODS and Training
The general lack of monitoring TI and MI across all studies raises questions about the practicality of the ODS and training. The introduction of the ODS placed greater responsibility on sonographers since they then needed to monitor the ODS throughout an examination as increases in the ODS raises the potential for bioeffects to occur. 9 To enable this monitoring to occur, manufacturers need to provide information about the ODS and purchasers need to provide training to sonographers to ensure the safe use of ultrasound equipment. 19 However, there is uncertainty about whether these provisions are complied with. 11 In the current study, 93% of participants reported receiving no training when a new ultrasound machine was purchased for the department, but only 40% of the sonographers believed training in TI and MI in relation to new equipment was important.
Ultrasound machines now have a higher acoustic output (720 mw/cm2) than previously, and sonographers may consider that any output level up to but not above this maximum is safe. There may be a belief by sonographers that manufacturers will not build machines that will operate at levels beyond which bioeffects may occur. This trust in the machine may explain the lack of monitoring of the TI and MI in the current studies and previous studies that assessed this area of practice.8,12,15 This was a point raised by student sonographer in the focus group who spoke of trust in the machine: “I think, we just, trust the technology we are using so much and I have never heard of it (TI/MI) being exceeded so you know I’m not gonna focus on that.” With advancing machine technology and greater responsibility transferred to the sonographer/ultrasound user, it is important that education and training in bioeffects is provided.
Guidelines and Safety Implications
An increasing number of guidelines worldwide have emerged since acoustic output levels of ultrasound machines were increased. 20 The guidelines aim to guide safe practice for sonographers but are based largely on animal studies. 19 These animal studies showed adverse effects at levels that are currently available for use in humans. While no human studies have yet demonstrated adverse effects, all but one of these studies was conducted prior to the introduction of the higher acoustic output in 1992. For fetal ultrasound, the new acceptable limit of 720 mW/cm2 is almost eight times higher than the original 92 mW/cm2 considered as an acceptable level for fetal examinations. 9 Therefore, it is now unclear as to what effect ultrasound exposure to the fetus has, and the validity associated with use of animal studies as a basis for guidelines is dubious.
Further research to explore potential bioeffects in humans may prove challenging. While some imaging modalities including X-ray and computed tomography (CT) have known harmful effects, there is a strong public perception of the safety of ultrasound scanning, particularly in imaging the fetus; there is also an expectation that multiple scans will be undertaken during pregnancy to check the health of the baby.21,22 The alternative of providing all pregnant patients with a magnetic resonance imaging (MRI) scan is problematic as MRI is not recommended for the first trimester, and in addition, would not feasible due to the higher costs and limited availability of MRI when compared to that of ultrasound.23,24
Conclusion
While Australasian sonographers showed some knowledge of the theoretical concepts associated with ultrasound bioeffects, there was poorer knowledge of guidelines, safety limits, and altered regulations for machine limits, which may impact on their safe practice. There was generally a low level of interest in ultrasound safety with uncertainly about attitudes to scans and a lack of concern about the importance of updating knowledge of bioeffects and translating this into ultrasound equipment training. With the exception of obstetric scans, particularly Doppler in the third trimester, monitoring for bioeffects was not a high priority, with attention to adjusting scanning parameters to ensure safety sacrificed for the quality and comprehensiveness of the ultrasound images. Overall, while most sonographers have the knowledge, few monitor the important parameters to reduce bioeffects in practice, suggesting a disparity with their beliefs about their importance. Further research is required to explain the disparities between knowledge, and attitudes and practices to ultrasound safety.
Footnotes
Appendix System Controls of TI and MI
System Controls of Ultrasound Machine and Influences on TI and MI.6,7,19,25,26,27
| System Control | Description | How It Affects Image Quality | How It Affects the Thermal Index (TI) | How It Affects the Mechanical Index (MI) |
|---|---|---|---|---|
| Output Power (OP) | Measures wave amplitude (Watts) | Increased OP, increases image quality by improved ultrasound beam penetration | Increased OP increases TI | Increased OP increases MI |
| Frequency (F) | Measures number of oscillations per second of particles in medium | Increased F shortens wavelength and increases image quality, also increases attenuation of the beam | Increased F increases TI | Increased F decreases MI |
| Field of View (FOV) | Measures amount if tissue viewed at one time | Decreased FOV concentrates beam to smaller space improving spatial resolution of images | Decreased FOV increases TI | Decreased FOV increases MI |
| Position of Focal Zone (FZ) | Section of beam less than twice its minimum width | Increases image quality of structures within FZ | Decreased FZ increases TI | Decreased FZ increases MI |
| Zoom | Magnifies selected area of image Two types: Write zoom and Read zoom |
Zoom increases image quality (Write zoom improves quality image more than Read zoom) | Write zoom increases TI; Read zoom does not increase TI | Write zoom increases MI; Read zoom does not increase MI |
| Mode of Operation | B-Mode, M-Mode, and Doppler imaging | Mode used determined by examination | B-Mode: Insignificant increase in TI | B-Mode: Insignificant increase in MI |
| M-Mode: Increases TI |
M-Mode: Increases MI |
|||
| Exposure Time | Total tissue exposure time |
|
Increased exposure time increases TI | Increased exposure time increases MI |
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.