
Abstract
The contraction stress test (CST) is currently the only modality used to test for placental insufficiency. It is rarely used due to possible complications. We propose a new test to assess placental reserves by measuring fetal heart rate (FHR) fetal responses to maternal exercise (FRME). A cohort of 640 term patients underwent FRME for accepted clinical indications. There was a total of 1680 tests, performed using a motorized treadmill in a moderate exercise regimen. Monitoring was provided by using standard Philips equipment (Avalon CTS and FM40). FRME was interpreted as negative (absence of decelerations, possible presence of accelerations), positive (presence of late decelerations or sustained bradycardia), or inconclusive. The results demonstrated 1506 tests were negative, 58 were positive, and 312 were inconclusive. If the test was negative, only 2% of the fetuses experienced adverse outcomes, versus 14%, when the test was positive. Positive tests were associated with 29% of category III FHR tracing, 11.6% of 5-minute Apgar score of less than 7, 9.8% admissions to the intensive care nursery, 2.2% of growth restrictions, and 1.2% of fetal or early neonatal demises. FRME if positive is associated with adverse perinatal outcome and could be included into the armamentarium of fetal testing.
Currently, the contraction stress test (CST) is the only existing test to assess fetal reserves. However, CST has a limited use because it is time consuming, requires IV placement and short hospitalization, and may put the patient in preterm labor. 1 We propose a new test to assess fetal reserves by measuring fetal heart rate (FHR) responses to maternal exercise.
The World Health Organization and the American College of Sports Medicine have issued evidence-based recommendations indicating that the beneficial effects of exercise in most adults are indisputable and that the benefits far outweigh the risks.2,3
Exercise in pregnancy has been shown to benefit most women. Regular physical activity during pregnancy improves or maintains physical fitness, helps with weight management, reduces the risk of gestational diabetes, and enhances patient’s psychological well-being. 2 In 2008, the US Department of Health and Human Services issued physical activity guidelines for adults, including pregnant women. For healthy pregnant women, the guidelines recommend at least 150 minutes per week of moderate-intensity aerobic activity. 4 The guidelines also advise that pregnant women who habitually engage in vigorous-intensity aerobic activity (i.e., the equivalent of running or jogging) can continue physical activity during pregnancy.2,3
Most of the studies addressing the fetal response to maternal exercise have demonstrated a moderate increase in FHR by 10 to 30 beats per minute over the baseline during or after exercise.5–8 A recommended exercise regimen is considered advantageous for pregnant women and safe for their fetus. A recent study has confirmed the safety of exercise for the fetus using all available fetal imaging and heart testing modalities, including non-stress test (NST), biophysical profile, and umbilical artery Doppler. 8
In view of the research data confirming the safety of exercise in pregnancy, we decided to use maternal exercise to test fetal resources. Similar to stress test in adult cardiology, CST remains the only available test for this purpose. However, CST required short hospital time, IV-line placement, and use of oxytocin and can cause iatrogenic premature labor. Exercise, on the other hand, causes increased maternal heart rate and can be used to test fetal resources. Fetal resources are determined by the type of fetal responses to decrease placental perfusion caused by maternal exercise. Healthy fetuses do not exhibit abnormal FHR tracings in response to maternal exercise. Our preliminary observation demonstrated that if utero-placental circulation has been compromised, the FHR will deteriorate during maternal exercise.9,10
Methods
Six hundred and forty patients, aged 22 to 42, between 36 and 42 weeks of pregnancy, were included in the study. A total of 1680 fetal assessments were performed for the following indications: decreased fetal movements, advanced maternal age, restricted fetal growth, pregestational and gestational diabetes, postterm pregnancy, and a history of fetal distress during previous pregnancies. For maternal exercises, we used a motorized treadmill in a moderate exercise regimen (15-minute fast walk at a speed of 3 mph with an incline of 15° to 25°). The research protocol was approved by the Institutional Review Board of NY Downtown Hospital (North America study group) and the Helsinki Committee at Moscow University School of Medicine. All participants of the study signed an informed consent.
Fetal monitoring was provided by using standard Phillips equipment (Avalon CTS and FM40). Exclusion criteria were as follows: multifetal pregnancies, fetal abnormalities, severe hypertension, morbid obesity, class III or IV heart disease, and neurological disorders. Fetal surveillance using accepted clinical modalities (NST, biophysical profile) were used in parallel to the study protocol, as required by the hospital and Institutional Review Board policy.
Adverse fetal outcomes were considered if one or more of the following were present:
category III FHR tracing (persistent late and/or deep variable decelerations, fetal bradycardia, sinusoidal rhythm)
5-minute Apgar score of less than 7
admission to the neonatal intensive care nursery (NICU), unrelated to prematurity
fetal growth restriction
fetal and early neonatal demise.
Category III FHR tracing was defined as presence of persistent, late decelerations, recurrent, variable decelerations, bradycardia, and a sinusoidal pattern. The Apgar score consisted of five parameters: heart rate, skin color, reflexes, respiratory efforts, and muscle tone; a score of 10 represented the best possible condition.
FRME, like a CST, was interpreted as negative (absence of decelerations, possible presence of accelerations), positive (presence of late decelerations or sustained bradycardia), or inconclusive (Figure 1 and Figure 2). Statistical analysis was performed using PSAW Statistics (version 18.0; IBM Corporation, New York, NY). Fisher’s exact test was used for nominal variables when the total sample size was relatively small; chi-square test was used for larger sample sizes. Wilcoxon rank test was used as a nonparametric alternative. A P value of less than .05 is considered statistically significant.
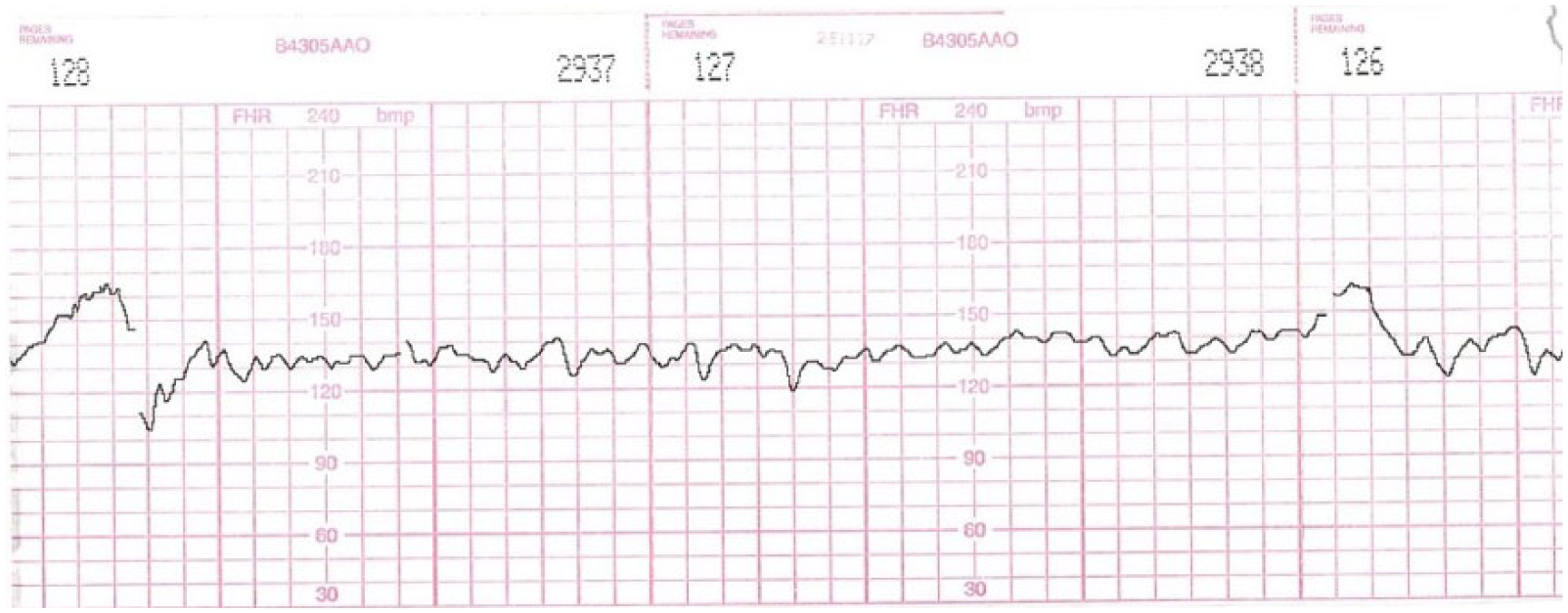
Negative FRME. Please note normal baseline, fetal heart rate accelerations, and lack of decelerations.
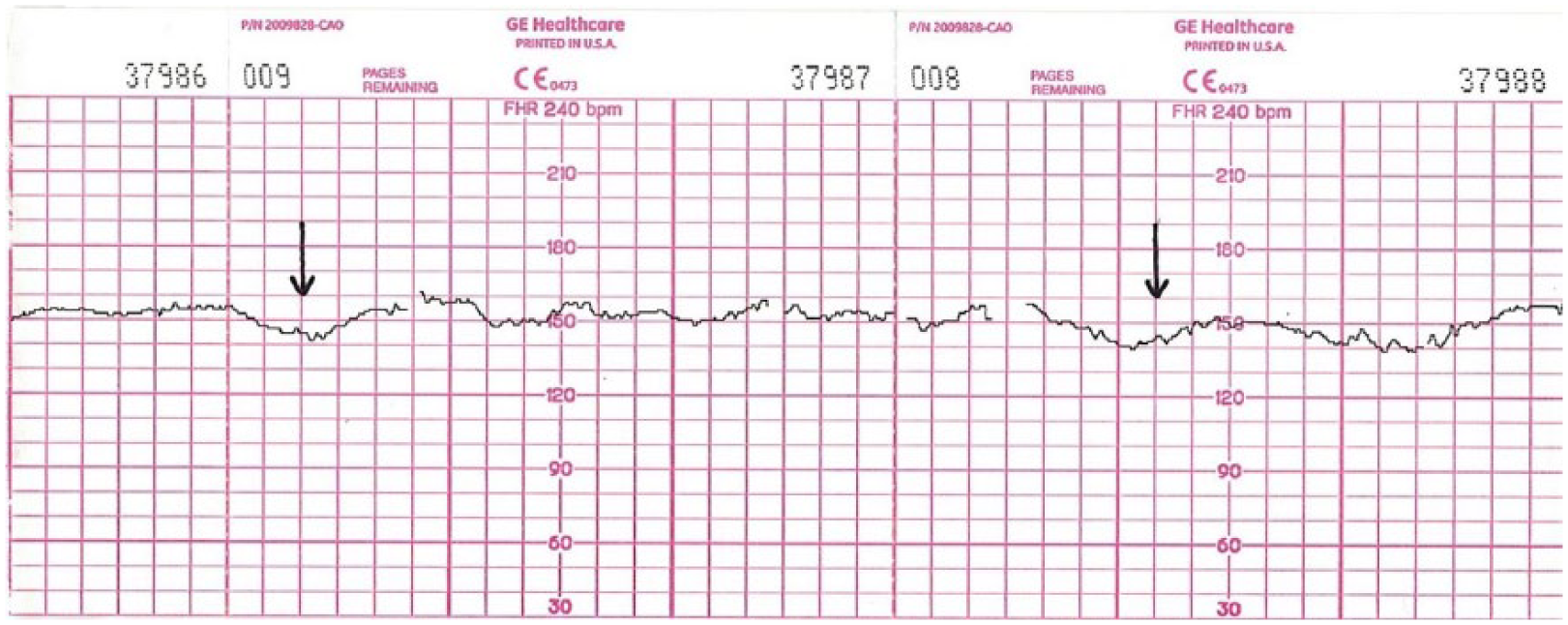
Positive FRME. Please note persistent late fetal heart rate decelerations (arrows).
Results
FRME results have been classified into 3 separate categories: negative, positive, and inconclusive. We use these parameters to assess FRME tests because they were widely used in medical literature to assess the effectiveness of CST. In all, 1506 tests were negative, 58 were positive, and 312 were inconclusive. Inconclusive results were due to artifacts and an inability to maintain a satisfactory, continuous, FHR tracing.
A Relationship Between Positive and Negative Fetal Responses to Maternal Exercise (FRME) and Overall Incidence of Adverse Perinatal Outcome. a
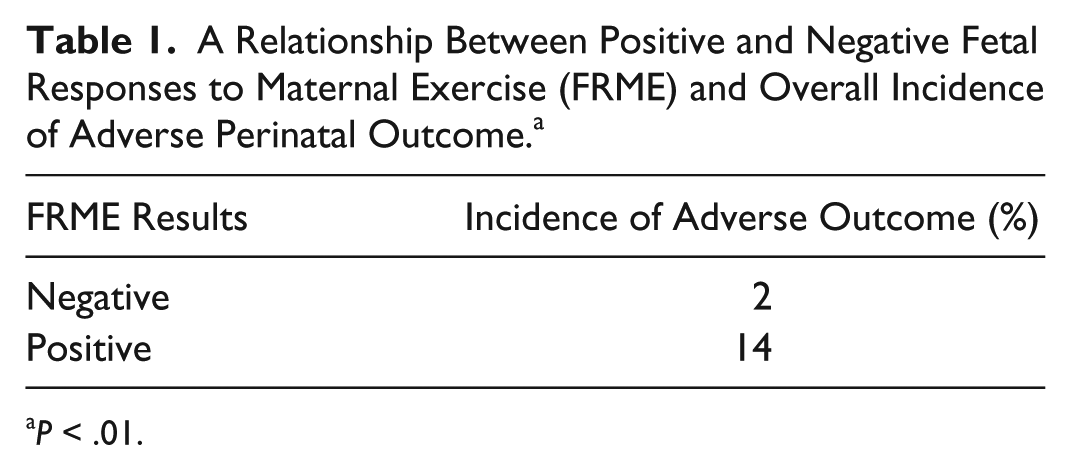
P < .01.
A Relationship Between Fetal Responses to Maternal Exercise (FRME) and Adverse Perinatal Outcomes.
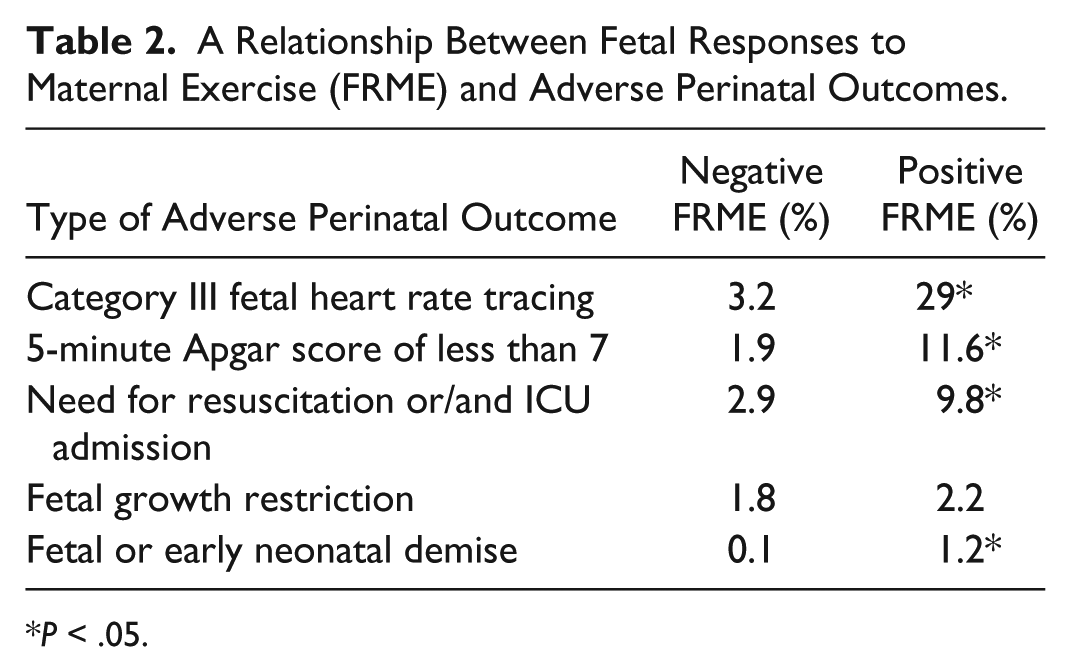
P < .05.
Discussion
FHR changes in response to maternal exercise has been reported and observed by numerous researchers.11,12 Thus, Macones et al. 12 observed short-lasting FHR decelerations in exercising mothers. Chaddha et al. 13 reported that maternal exercise may divert blood flow from the gravid uterus to the exercising limbs. Ertan et al. 14 studied fetal circulation in response to maternal exercise in small for gestational age fetuses. They concluded that fetal cerebral vasodilation became more pronounced after maternal exercise. Both research groups concluded that maternal exercise at 10% to 15% of power output may result in a transient reduction in umbilical blood flow due to placental vasoconstriction. Fetal responses to maternal exercise has been also studied by Artal et al., 15 who confirmed that exercise may induce cardiovascular changes with the selective redistribution of blood flow to the muscles away from the visceral organs. This group reported a decrease in FHR, down to 90 bpm, in 5 out of 45 fetuses as a result of maternal exercise. Green et al. 16 performed continuous FHR monitoring in 26 women who were exercising as a part of a prenatal fitness program in Australia. Eight patients while exercising in a supine position developed a decrease in FHR and beat-to-beat variability with an adverse perinatal outcome in two of them. The goal of our study was to establish the usefulness of the FRME to predict adverse neonatal outcomes. Current modalities in antepartum fetal surveillance had been largely developed in the 1990s and haven’t changed significantly since. Most of the tests currently used are not designed to assess fetal reserves.17-19
We propose an FRME test as an alternative to CST. It has advantages over CST: It can be performed in the office without intravenous administration of oxytocin. We conducted a prospective longitudinal study using the FRME test. We included fetal and early neonatal demise as the key outcome features along with the category III tracings, low 5-minute Apgar scores, and NICU admission. These parameters are considered the gold standard in assessing fetal well-being in numerous previous studies.20,21 Like the CST, positive FRME tests were associated with a seven-fold increase in adverse perinatal outcome. It appears that the FRME test is especially predictive of abnormal FHR patterns, low 5-minute Apgar scores, and NICU admissions. The main advantage of the study is its novelty. The study’s limitations are an insufficient number of high-risk patients and lack of long-term neonatal follow-up. Further improvement in distant fetal monitoring equipment will allow the number of inconclusive results to decrease. Further studies are needed to establish the place of FRME test for antepartum fetal surveillance.
Conclusion
It appears that similar to CST, positive FRME has a high correlation with adverse perinatal outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.