
Abstract
The objective of this study was to determine the accuracy of sonography in a human immunodeficiency virus–associated nephropathy (HIVAN) diagnosis. A sample of 340 HIVAN patients underwent laboratory CD4+ count, serum creatinine/glomerular filtration rate (GFR) estimation, and sonographic echogenicity grading. The accuracy of sonography in predicting an HIVAN diagnosis was calculated. Mean CD4+ count, serum creatinine, and GFR for male and female HIVAN patients was 153.1 ± 103.2 cells/mm3 and 121.9 ± 91.0 cells/mm3, 218.4 ± 147.4 mmol/L and 222.0 ± 150.4 mmol/L, and 50.1 ± 23.6 mL/min/1.73 m2 and 39.3 ± 20.6 mL/min/1.73 m2, respectively; 56.9% of patients had echogenicity grade 3. On the basis of CD4+ count, serum creatinine, and GFR, the area under the curve was 0.76 and ≈ 1, respectively; the area under the curve was 0.63, 0.79, 0.70, 0.79 and 0.91, 0.99, 1, 1 for grades 0, 1, 2, and 3 echogenicity, respectively. With a high level of apathy to voluntary HIV/AIDS screening and late patient presentation, sonography (grade 3 renal echogenicity) can assist in predicting an HIVAN diagnosis.
Human immunodeficiency virus (HIV) infection, which causes acquired immunodeficiency syndrome (AIDS), remains a major public issue in the world. The public health challenge posed by HIV/AIDS is worse in developing countries, especially those in the sub-Saharan region of Africa. 1 HIV infection has a wide spectrum of renal manifestations. Renal function impairment is caused by direct HIV infection or indirectly by nephrotoxic drugs used in HIV/AIDS treatment, with HIV-associated nephropathy (HIVAN) being the most common cause of renal failure in the HIV infected.1,2,3
HIVAN develops at the latent stage of HIV infection. Risk factors for HIVAN development include a CD4+ cell count less than 200 cells/mm3 as well as a high viral load. 4 HIVAN is characterized by increasing serum creatinine, low glomerular filtration rate (GFR), and severe proteinuria (> 3 g/24 h). HIVAN is predominant among people of African descent and is notorious for its rapid progression to renal failure and end-stage renal disease. 5
Sonography is the most common and most widely deployed imaging modality in the evaluation of HIV-infected patients with renal diseases in Nigeria. 6 Common sonographic findings (Figure 2) in HIV-infected patients with nephropathy include enlarged kidneys and increased cortical echogenicity.7,8 In spite of this, the specific diagnosis of HIVAN relies primarily on histopathologic study that involves renal biopsy. 9 To improve prognosis, early HIVAN diagnosis is important. Whereas physical evaluation is largely nonspecific, 10 renal biopsy is needed for a definitive HIVAN diagnosis, but it is not readily done in Nigeria because of the lack of nephrologists, infrastructure, and funds. Monitoring residual renal function in patients with chronic kidney disease is important, 11 and measurement of GFR is the gold standard for renal function assessment. 12 In Nigeria, HIVAN diagnosis is generally made on the basis of clinical signs and laboratory estimated serum creatinine levels. In spite of its usefulness, biochemical monitoring of residual renal function among AIDS patients is very expensive. 13 According to an estimate by Africa HIV/AIDS, 14 Nigeria has the second highest adult HIV/AIDS prevalence in Africa. In Nigeria and other developing countries with a poorly funded health care system, a relatively less expensive and easily available diagnostic modality for HIVAN is needed. The aim of the present study was to characterize laboratory changes among AIDS patients with nephropathy to determine the utility of renal cortical echogenicity for predicting HIVAN diagnosis.
Method
This prospective cross-sectional study was carried out at a tertiary hospital in Lagos, Southwest Nigeria, from August 2015 to September 2016. In line with the standards for reporting diagnostic accuracy studies, potentially eligible participants were identified. They were first-time attendees who presented with symptoms and signs of the AIDS disease. Only those who were confirmed sero-positive for HIV antibodies by enzyme-linked immunosorbent assay and subsequent Western blot test and who had not commenced antiretroviral therapy were eligible. A sample of 340 adults was recruited from eligible participants in a consecutive manner. With regard to the control group, the eligible participants were healthy adults who included the patients’ relatives, hospital staff, and students. Those who were confirmed to be sero-negative to the HIV antibody after laboratory screening were identified. A 1:1 male-to-female ratio was used to select 340 age- and sex-matched healthy adults for the control group. The Health Research and Ethics Committee of the hospital approved the study design, and an informed written consent was obtained from all participants prior to the study. Only adults (≥ 18 years) were included in the study. Patients with a blood pressure > 140/90 mm Hg in two consecutive measurements were also excluded. Additionally, those patients with diabetes mellitus (as defined by American Diabetes Association criteria), disseminated pulmonary tuberculosis, fungal infection, viral infections such as hepatitis B or C, vasculitides, and a history of prolonged use of nonsteroidal anti-inflammatory drugs were excluded.
Data Collection
Information concerning each patient’s age, marital status, and occupation was collected. A laboratory scientist used blood samples collected by a physician to perform direct flow cytometry, which was done to calculate CD4+ percentage using a CYFLOW Counter-II flow cytometer (Model 110168222; Partec Inc., Görlitz, Germany), whereas serum creatinine was quantified using a COBAS TaqMan automated chemistry analyzer (COBAS AmpliPrep/COBAS TaqMan SN-394418; Roche Diagnostics, Risch-Rotkreuz, Switzerland). Estimation of glomerular filtration rate (eGFR) was done from serum creatinine levels using the GFR e-calculator. A sonographer with more than 8 years’ experience in renal/abdominal sonography used high resolution ultrasound equipment with a 3.5 MHz convex probe (XG SSA-58GA; Toshiba Diagnostic Ultrasound Systems Ltd., Tokyo, Japan) to perform the imaging examinations in the study.
Patients were placed in the right or left anterior oblique position for imaging of the right and left kidneys, respectively. Care was taken to ensure that renal pyramids were well visualized; that images demonstrated even amounts of cortical tissue around the renal sinus, except at the medial aspect of the kidney; and that the upper and lower poles of the kidney were clearly demonstrated. These parameters had to be met before an image of a kidney was considered optimal. 15 Frozen images were stored in the image storage center of the ultrasound equipment and were later copied using an external disk drive. The liver was used as the standard comparison criterion, 16 and the renal echogenicity was categorized as follows:
Grade 0: Kidney cortical echogenicity is slightly less than that of the liver.
Grade 1: Kidney cortical echogenicity is the same as that of the liver.
Grade 2: Kidney cortical echogenicity is moderately higher than that of the liver, with moderate loss of corticomedullary distinction.
Grade 3: Kidney cortical echogenicity is much higher than that of the liver, with complete loss of corticomedullary distinction.
Data Analysis
MedCalc statistical software for biomedical research, version 12.5 (MedCalc Software, Ostend, Belgium), was used. Mean viral load, CD4+ count, serum creatinine, and GFR for HIVAN patients were computed. Proportions for grades 0, 1, 2, and 3 echogenicity were compared using the chi-square statistic. One-way analysis of variance (ANOVA) was used with Scheffe’s post-hoc test to determine the usefulness of sonography in predicting an HIVAN diagnosis.17,18 Pearson’s product-moment correlation analysis was used to determine whether correlation exists between renal echogenicity, CD4+ count, serum creatinine, and GFR. True and false positive rates of serum creatinine were used to plot receiver operating characteristic (ROC) curves. Thereafter, operating characteristics of the ROC curves such as area under the curve (AUC) and diagnostic likelihood ratios (LRs) were used to determine which renal echogenicity grade is most predictive of an HIVAN diagnosis on the basis of CD4+ count, serum creatinine levels, and GFR. Results were tested for statistical significance at an alpha level of P = .05.
Results
Based on the 340 patients studied, 54.7% were male and 45.3% were female. The mean age, weight, height, and body mass index were as follows, respectively: 42.7 ± 9.4 years, 70.4 ± 10.8 kg, 1.6 ± 0.6 m, and 41.4 ± 5.1 kg/m2. The mode for age was 45 to 49 years for men and 35 to 39 years for women. Additionally, demographics were that 40.3% of the patients were married, 53.2% were traders, 27.9% were artisans, 15.9% were civil servants, and 2.9% were members of the armed forces. Among the complete patient cohort, 87.4% were diagnosed as having HIVAN.
Mean viral load, CD4+ count, serum creatinine, and GFR for male and female HIVAN patients were 303204.0 ± 24812.9 copies/mL and 216514.6 ± 18823.0 copies/mL, 153.1 ± 103.2 cells/mm3 and 121.9 ± 91.0 cells/mm3, 218.4 ± 147.4 mmol/L and 222.0 ± 150.4 mmol/L, 50.1 ± 23.6 mL/min/1.73 m2 and 39.3 ± 20.6 mL/min/1.73 m2, respectively.
All 340 participants in the control group and non-HIVAN patients (12.6%) had a grade 0 (normal) echogenicity, whereas 83.7% of non-HIVAN patients had insignificant immunosuppression. When the 297 HIVAN patients were considered, 56.9% had grade 3 echogenicity, and 51.5% of HIVAN patients with grade 3 echogenicity had severe immunosuppression. Figures 1 and 2 show echogenicity grades 0, 1, 2, and 3. A strong negative correlation exists between renal echogenicity and CD4+ count (r was −0.610, −0.609, −0.514, and −0.621 for grades 0, 1, 2, and 3; P < .05); the coefficient of correlation (r) was 0.813, 0.7630, 0.8832, and 0.9135, respectively, for grades 0, 1, 2, and 3 echogenicity (P = .0001) for the strength of association between renal echogenicity and GRF.
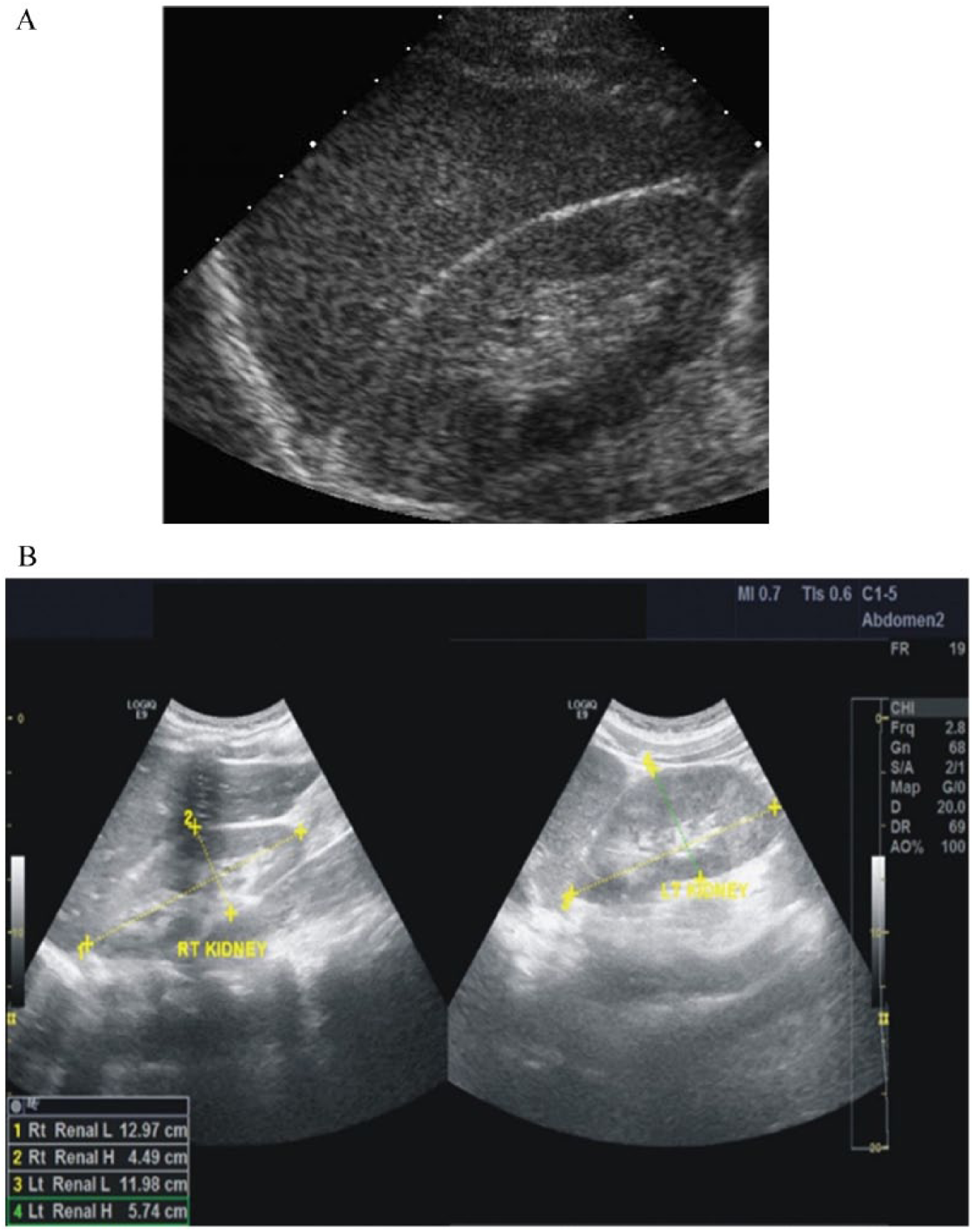
Sonograms showing renal echogenicity grades 0 (A) and 1 (B).
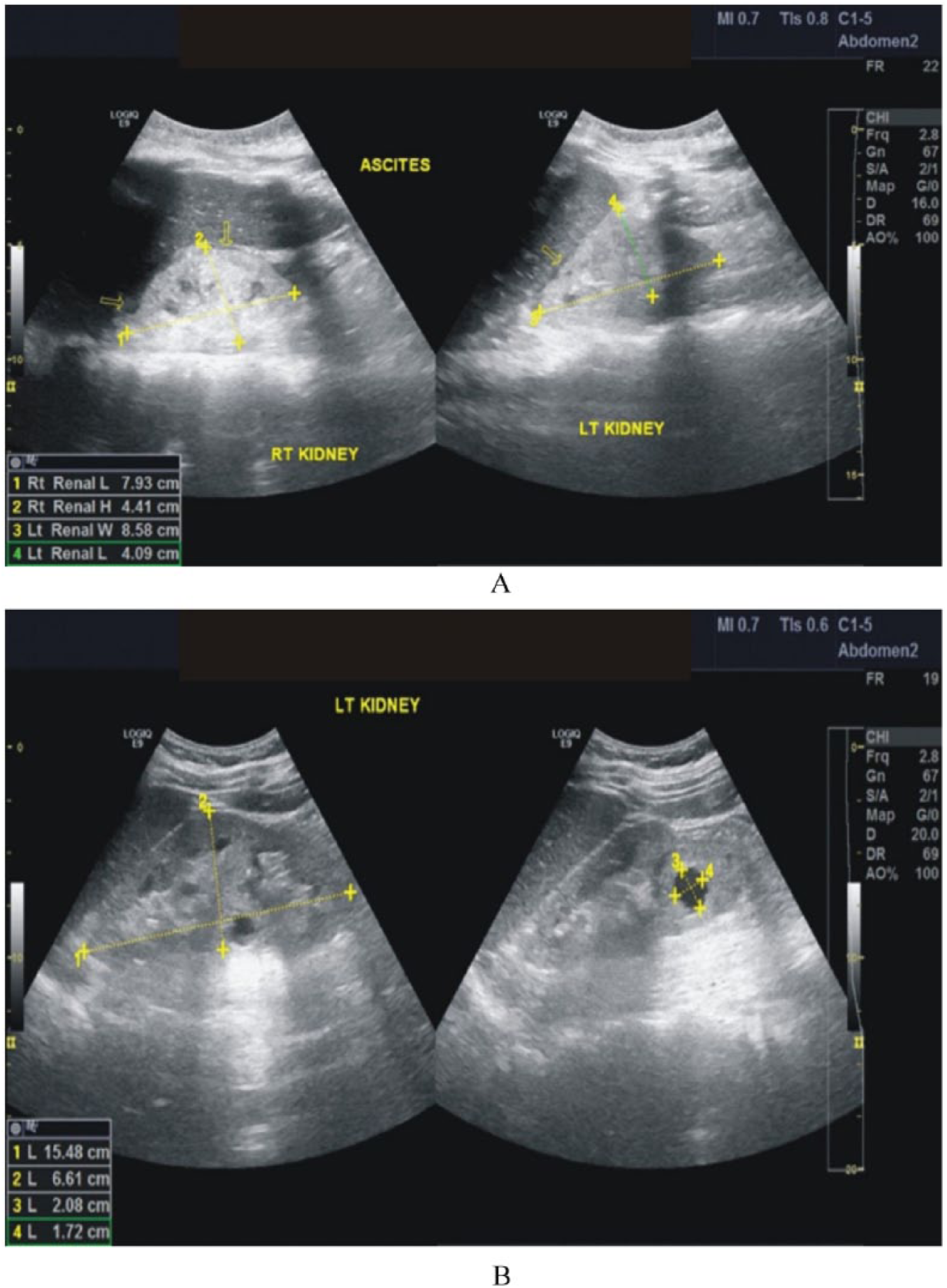
Sonograms showing renal echogenicity grades 2 (A) and 3 (B).
Table 1 indicates that at an F value of 5, sonography was a good model for predicting an HIVAN diagnosis on the basis of the CD4+ count (P = .004), serum creatinine (P = .035), and GFR (P = .002). Additionally, at each cutoff level of renal echogenicity as well as the CD4+ count, diagnostic accuracy was high (AUC = 0.76; Figure 3 and Table 2). On the basis of serum creatinine and GFR, sonography was an excellent predictor of an HIVAN diagnosis (AUC ≈ 1; Tables 3 and 4 and Figure 4). Figure 5 demonstrates that sonography is more accurate in predicting an HIVAN diagnosis on the basis of eGFR and serum creatinine than on the CD4+ count. Using the CD4+ count, serum creatinine, and eGFR, a renal echogenicity grade of 3 was the most accurate in predicting an HIVAN diagnosis (Tables 5, 6, and 7 as well as Figures 5B and 6, respectively).
ANOVA With Scheffe’s Test for Sonographic Prediction of Immunosuppression and Renal Function Impairment. a
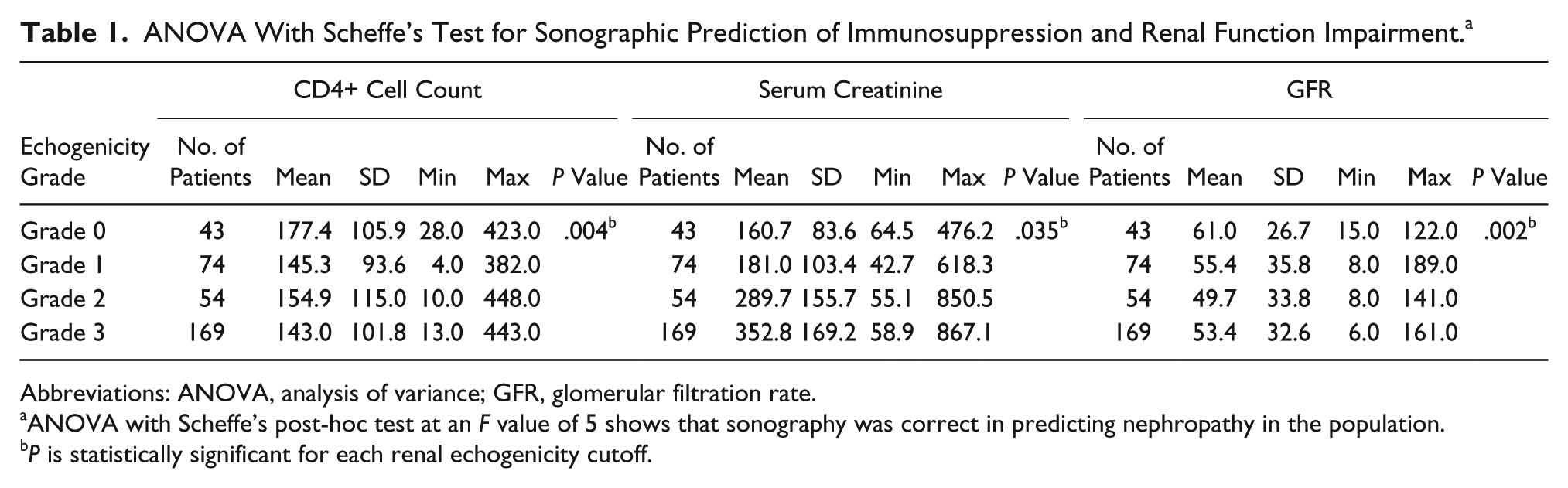
Abbreviations: ANOVA, analysis of variance; GFR, glomerular filtration rate.
ANOVA with Scheffe’s post-hoc test at an F value of 5 shows that sonography was correct in predicting nephropathy in the population.
P is statistically significant for each renal echogenicity cutoff.
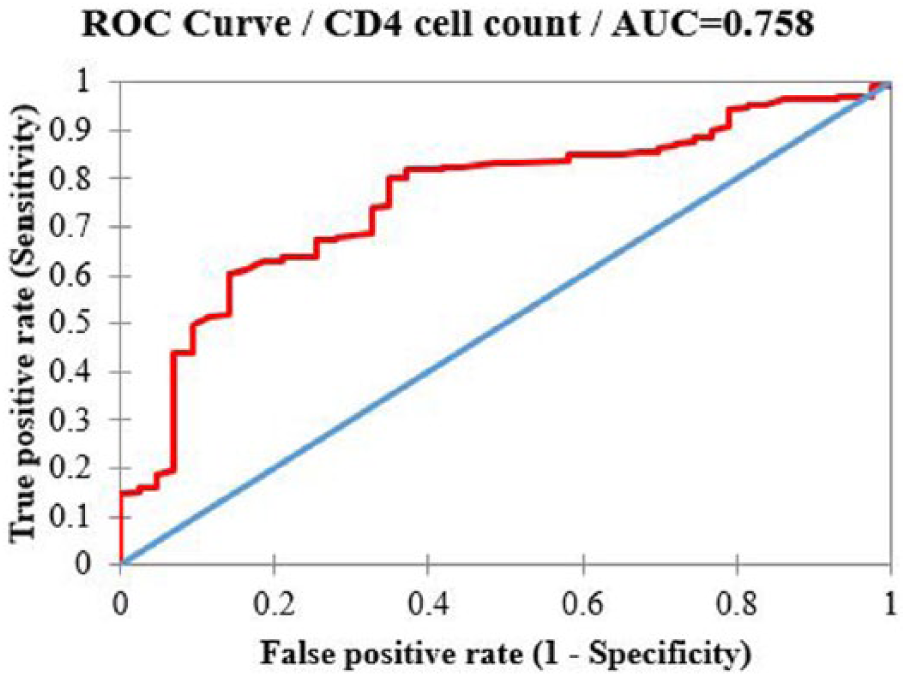
Receiver operating characteristic (ROC) curves of echogenicity versus CD4+ cell count. AUC, area under the curve.
Operating Characteristics for the Accuracy of Renal Echogenicity in Predicting a Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of CD4+ Count. a
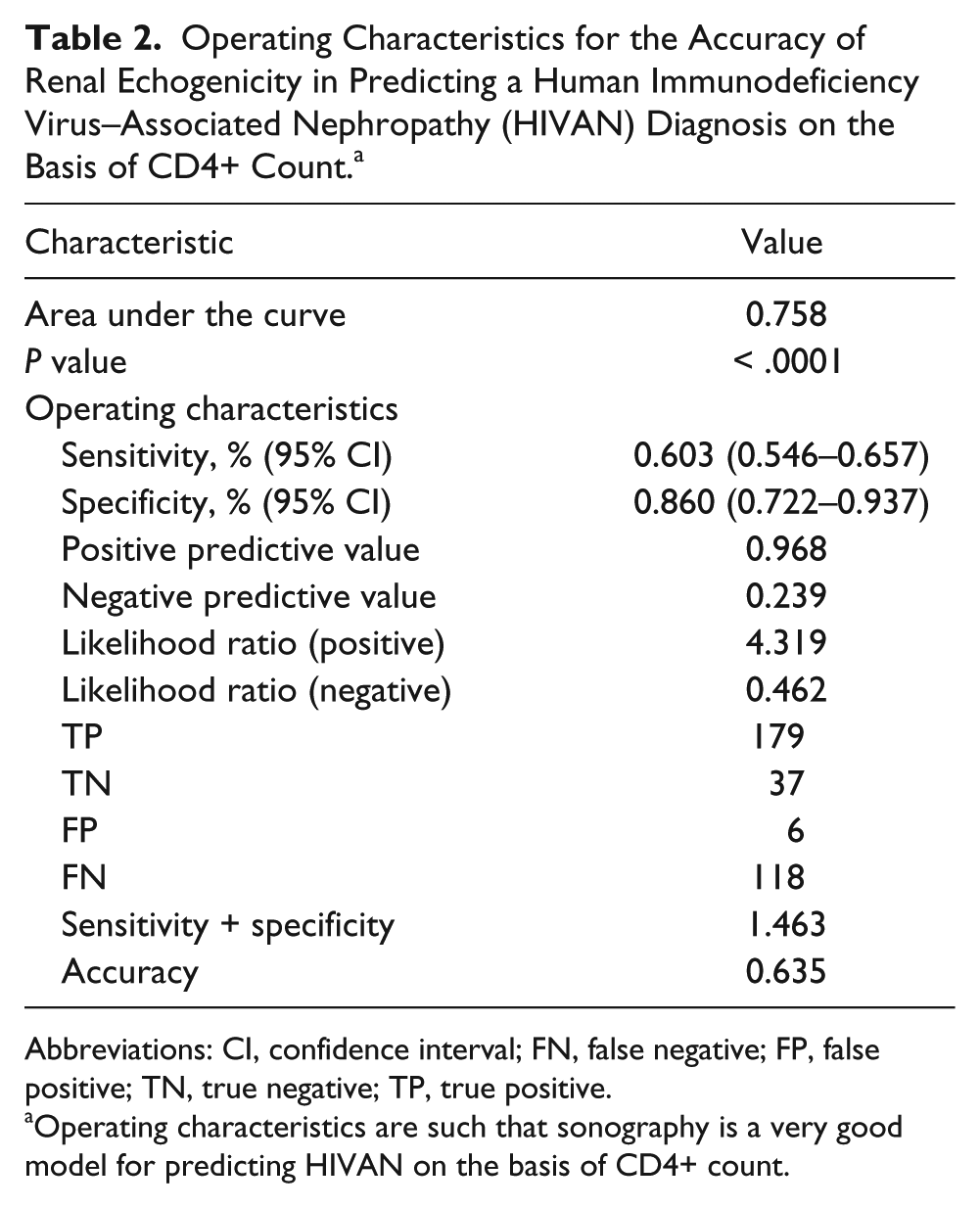
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics are such that sonography is a very good model for predicting HIVAN on the basis of CD4+ count.
Operating Characteristics for the Accuracy of Renal Echogenicity in Predicting a Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of Serum Creatinine Level. a
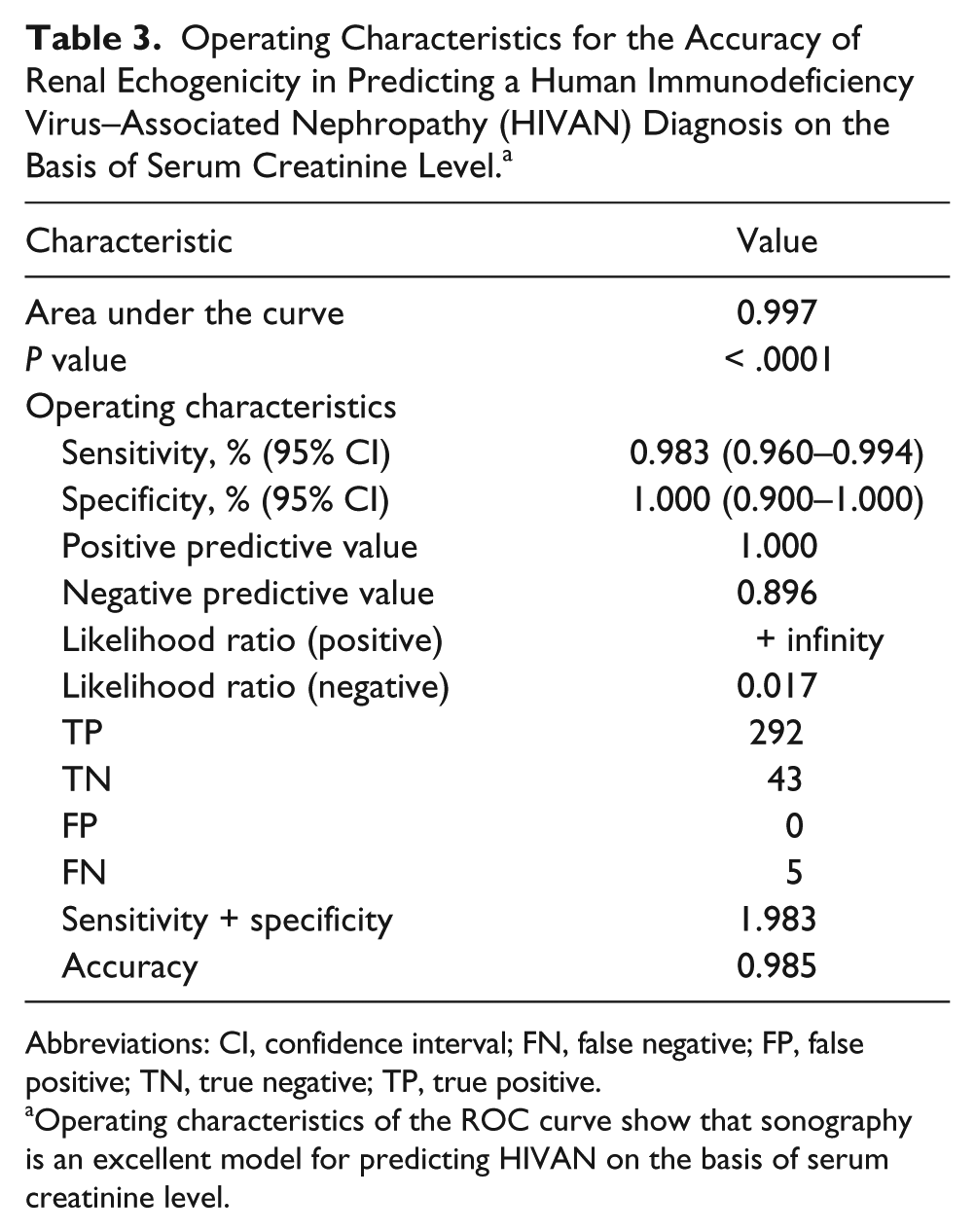
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics of the ROC curve show that sonography is an excellent model for predicting HIVAN on the basis of serum creatinine level.
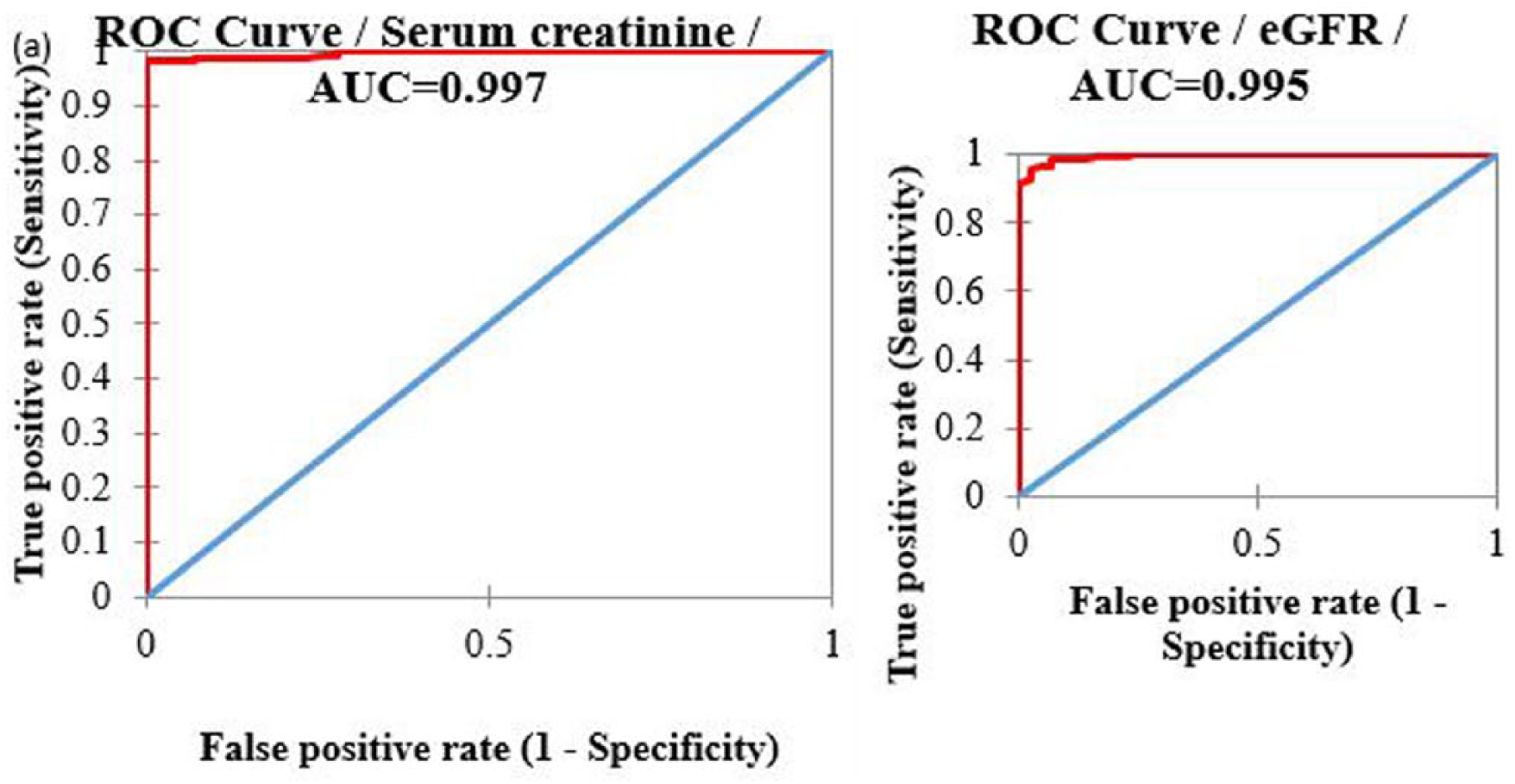
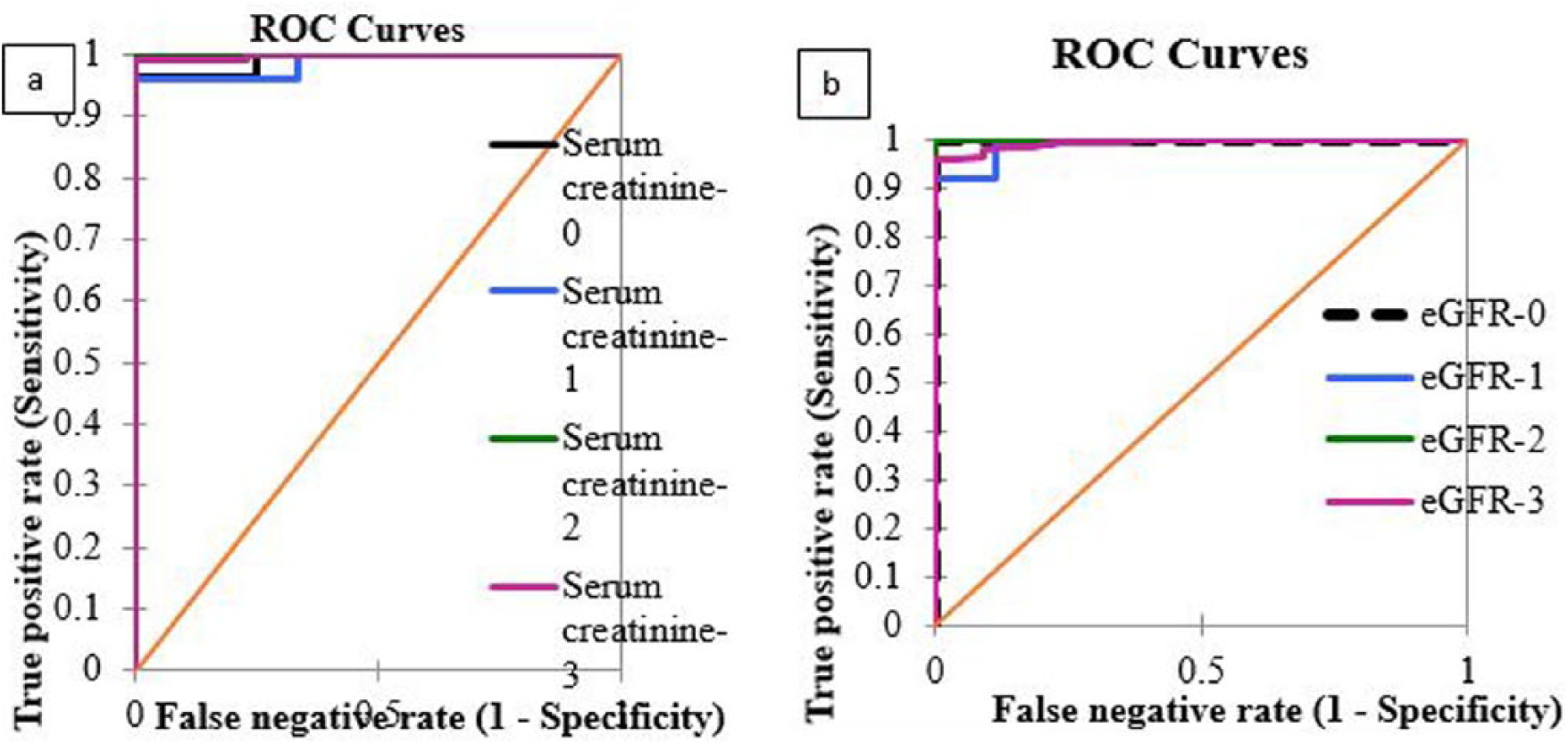
Receiver operating characteristic (ROC) curves showing accuracy of sonography in predicting a human immunodeficiency virus–associated nephropathy (HIVAN) diagnosis on the basis of serum creatinine and estimation of glomerular filtration rate (eGFR). AUC, area under the curve.
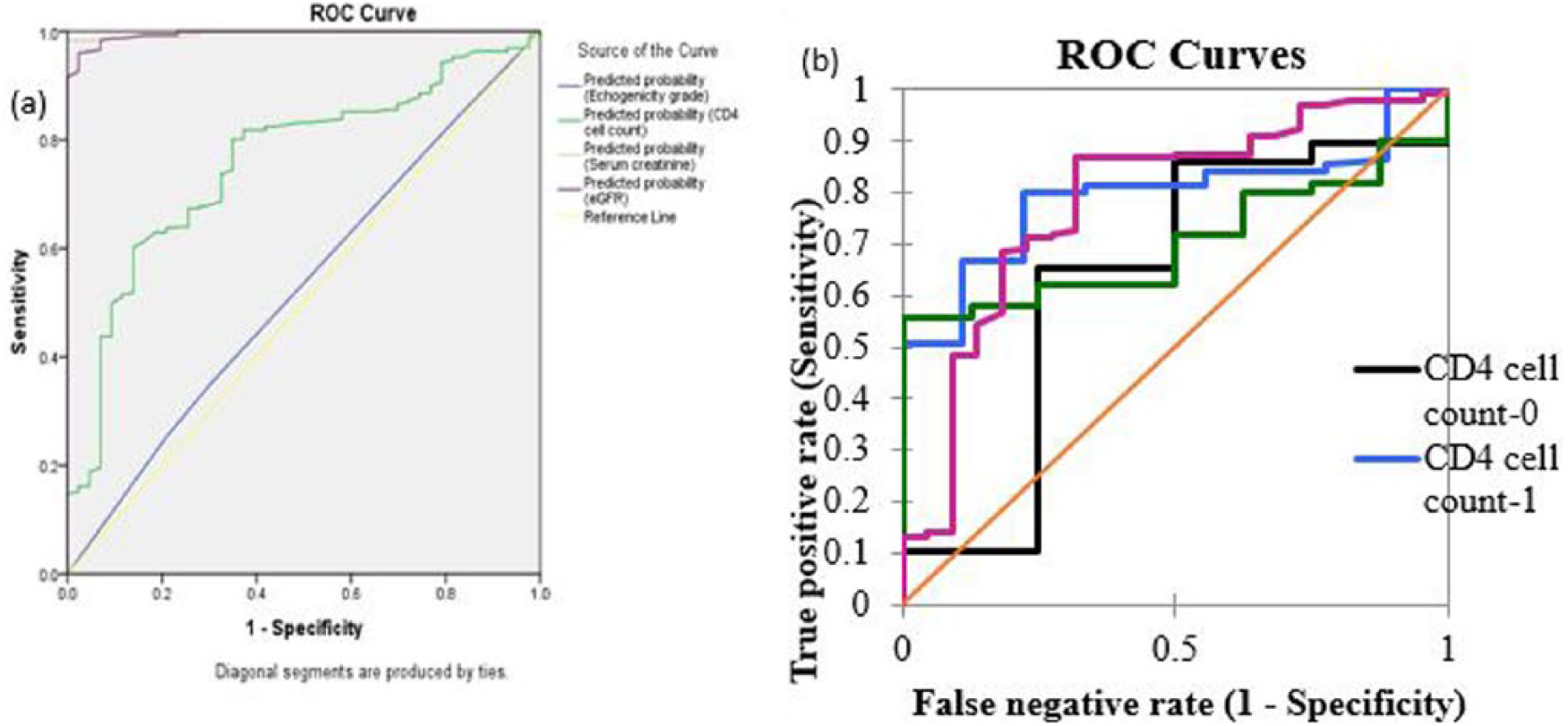
Receiver operating characteristic (ROC) curves of comparison of accuracy renal echogenicity in predicting a human immunodeficiency virus–associated nephropathy diagnosis.
Operating Characteristics for the Accuracy of Renal Echogenicity in Predicting a Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of Estimation of Glomerular Filtration Rate. a
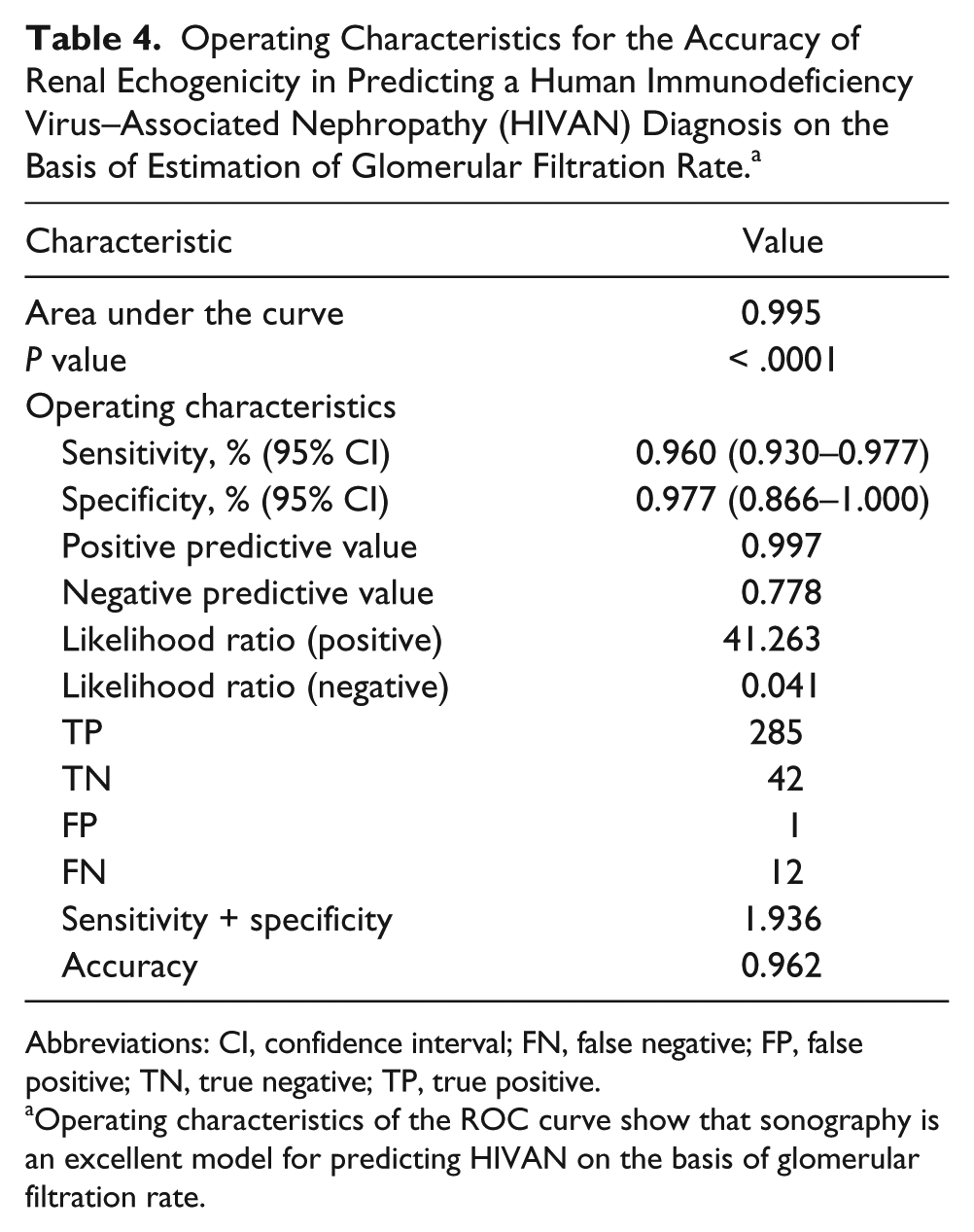
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics of the ROC curve show that sonography is an excellent model for predicting HIVAN on the basis of glomerular filtration rate.
Operating Characteristics for the Accuracy of Renal Echogenicity Grades 0, 1, 2, and 3 in Predicting a Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of CD4+ Cell Count. a
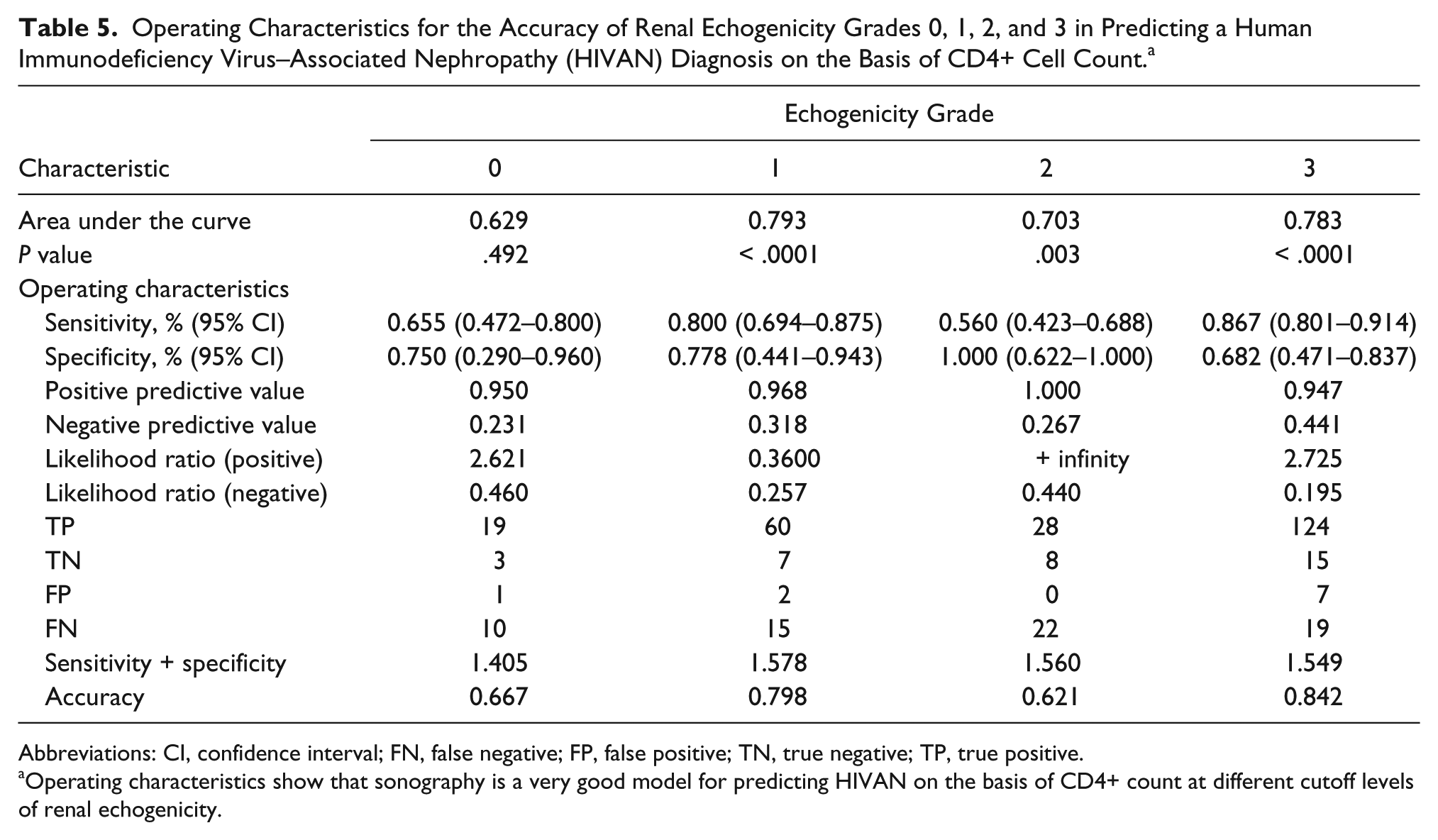
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics show that sonography is a very good model for predicting HIVAN on the basis of CD4+ count at different cutoff levels of renal echogenicity.
Operating Characteristics for the Accuracy of Renal Echogenicity Grades 0, 1, 2, and 3 in Predicting a Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of Serum Creatinine. a
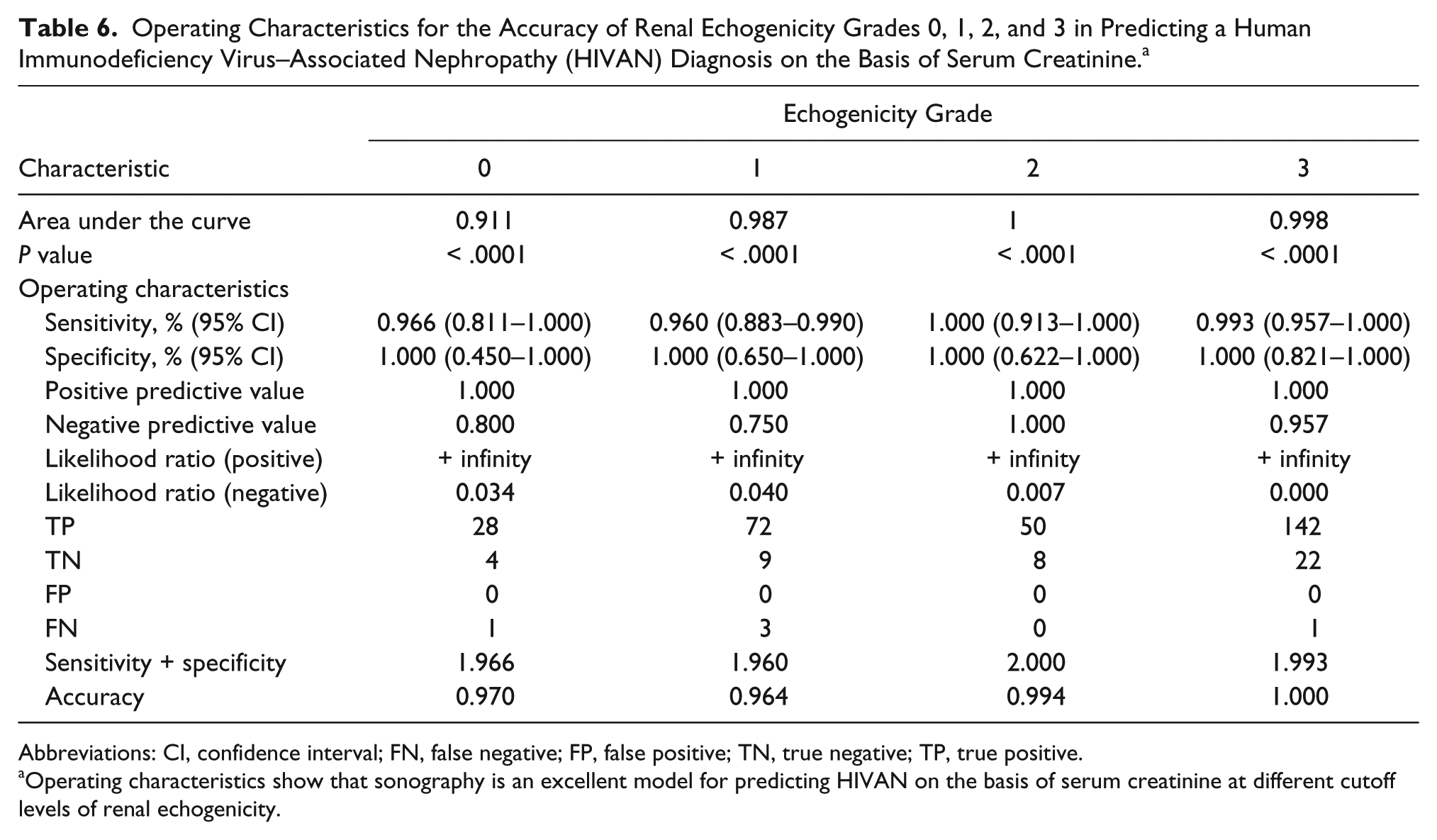
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics show that sonography is an excellent model for predicting HIVAN on the basis of serum creatinine at different cutoff levels of renal echogenicity.
Operating Characteristics for the Accuracy of Renal Echogenicity Grades 0, 1, 2, and 3 in Predicting Human Immunodeficiency Virus–Associated Nephropathy (HIVAN) Diagnosis on the Basis of Glomerular Filtration Rate. a
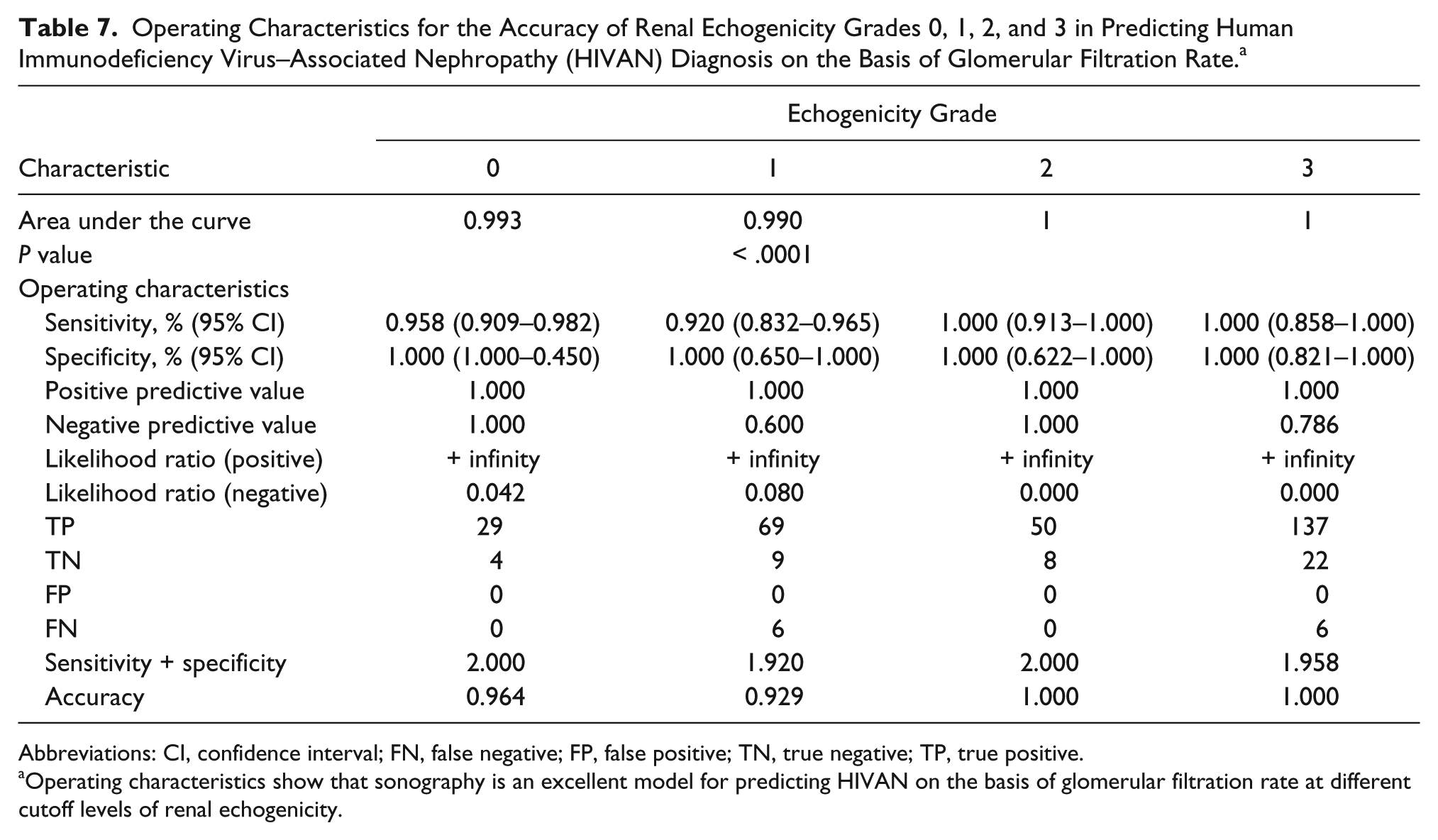
Abbreviations: CI, confidence interval; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Operating characteristics show that sonography is an excellent model for predicting HIVAN on the basis of glomerular filtration rate at different cutoff levels of renal echogenicity.
Comparison accuracy of renal echogenicity in human immunodeficiency virus–associated nephropathy prediction at different cutoff levels of renal echogenicity on the basis of serum creatinine and estimation of glomerular filtration rate (eGFR).
Discussion
The HIV/AIDS pandemic is largely predominant among the sexually active and economically productive age groups within the cohort studied. This is similar to the data previously reported by Kwaifa and Bosan 17 as well as Garko et al. 18 The scourge is predominant among self-employed (traders and artisans with a diverse incidence of AIDS) and married patients. This trend may indicate that the HIV/AIDS pandemic could negatively affect economic activities and could also disrupt many family structures in the Lagos metropolis. This finding may indicate that the economic burden of HIV/AIDS could worsen in Nigeria. There were slightly more men than women in the study, which is different from what was previously reported elsewhere in the country.19–21 Male predominance in the present study could be attributed to the fact that women generally have less access to health care because of unequal socioeconomic status and cultural practices in the sub-Saharan African region. 22
The high intensity of HIV infection in the population was perhaps a true reflection of their antiretroviral therapy naivety. Mean viral load in the population was higher than the previously reported mean among different AIDS patient cohorts on antiretroviral therapy in Nigeria.18,20 Immunosuppression was severe (worse among women) in the population as exemplified by mean CD4+ cell count < 200 cells/mm3. This shows that HIV infection was at its advanced stage before these patients presented for medical attention. These results are similar to previous reports across the country.18–21,23,24 This pattern would seem to indicate that the public awareness campaigns for voluntary HIV/AIDS screening may have underachieved, on the basis of these patient results. Although the exact time of HIV infection was not determined prior to the study, it appears that women were probably more susceptible to immunosuppression. The immunosuppression may be connected to reported sexual dimorphism with respect to HIV-RNA levels because of sex-biased gene expression of HIV-RNA among adults. 25 This phenomenon could also be attributed to sexual differences in cytokine production or other innate or adaptive immune mechanisms that cause differences in target cell availability or permissiveness to infection. 26 Renal function impairment was severe (worse among women) in the population. A similar pattern of renal function impairment was reported in Cameroon. 27 Although mean serum creatinine level in the study is smaller than 399 mmol/L and > 800 mmol/L previously reported in Nigeria,19,24 it does suggest that renal failure could become a worrisome medical condition in this future population.
It is known that the kidney is highly echogenic among AIDS patients with nephropathy.12,27 The present study supports this notion because all participants in the control group and non-HIVAN AIDS patients had a normal renal echogenicity (i.e., grade 0). In particular, most HIVAN patients had a grade 3 renal echogenicity (Figure 2) with complete loss of corticomedullary differentiation. This may suggest that sonographic grading of renal echogenicity has the potential to determine HIVAN in a patient. All patients with severe immunosuppression had a grade 3 renal echogenicity, whereas the Pearson’s product-moment correlation analysis showed a significantly strong negative association between renal echogenicity and CD4+ count (P < .05). The coefficient of correlation (r) was highest for a grade 3 echogenicity, thus supporting that a grade 3 renal echogenicity was most predictive of an HIVAN diagnosis. A strongly negative correlation between renal echogenicity and CD4+ count had previously been reported in Nigeria.18,21
In the present study, the F value (F = 5; Table 1) obtained from one-way ANOVA with Scheffe’s post-hoc test showed that sonography (i.e., renal echogenicity at different cutoff levels) was a categorical predictor of an HIVAN diagnosis. It is usually assumed that when the F value is positive, the ability of a diagnostic model with different predictors to accurately predict a positive diagnosis of a disease entity is not due to chance. In the present study, sonography was the diagnostic model, whereas its multiple predictors were echogenicity grades 0, 1, 2, and 3; hence, it is plausible to suggest that sonography could be relied on to predict an HIVAN diagnosis. This viewpoint lends support (albeit indirectly) to the notion that a strong and statistically significant positive correlation exists between renal echogenicity and serum creatinine increase. 28 The usefulness of sonography in predicting an HIVAN diagnosis being reported in the population studied is in agreement with the view that AIDS patients with HIVAN have significantly lower CD4+ counts, higher viral loads, higher serum creatinine levels, and lower GFR compared with the control group. This agreement was also reported in an HIV-positive, race-matched cohort study. 29
On the basis of CD4+ count (immunosuppression), the renal echogenicity at different cutoff levels could be a good diagnostic model for HIVAN, with an overall accuracy of 0.64. In addition to overall accuracy, the AUC was 0.76, and other operating characteristics of the ROC curve (Table 2 and Figure 3) all suggest that sonographic grading of renal echogenicity appears to be a good model for predicting severe immunosuppression in HIV-infected patients with symptoms and clinical signs of yet-to-be diagnosed AIDS. It may also be useful for those who have not commenced antiretroviral therapy. In like manner, ROC curves with their operating characteristics (Table 3 and Figure 4) also showed that sonographic grading of renal echogenicity was accurate in detecting renal function impairment vis-à-vis serum creatinine level. On the basis of GFR, the AUC, sensitivity, specificity, and overall accuracy of sonographic grading of kidney echogenicity in predicting an HIVAN diagnosis was ≈ 1.0 (Table 4 and Figure 4). All this reaffirms that in this group of patients, sonography was an excellent predictor of an HIVAN diagnosis, on the basis of serum creatinine level and GFR.
The positive likelihood ratio (LR+ = 2.62) of renal echogenicity grade 0 in predicting an HIVAN diagnosis on the basis of CD4+ count was greater than its negative likelihood ratio (LR– = 0.46) in the present study. It is generally believed that when the positive is higher than the negative LR, the chance of a diagnostic model to correctly predict a positive outcome is high. On face value, therefore, grade 0 renal echogenicity was good at predicting an HIVAN diagnosis. But a grade zero kidney echogenicity score depicts a normal renal cortex, 16 which is a rather negative outcome in the present study. This outcome implies that a renal echogenicity graded 0 ruled out rather than ruled in an HIVAN diagnosis in the present study. With this, we support Atta et al.’s 30 opinion that renal echogenicity grade 0 is more reliable in ruling out rather than ruling in an HIVAN diagnosis.
With an AUC of 0.79 (P = .0001) and overall accuracy of 0.80, grade 1 renal echogenicity was accurate in predicting an HIVAN diagnosis. But just like grade 0 renal echogenicity, a grade 1 score was mostly found among AIDS patients with normal kidneys in the present study. On the basis of these results, we support Atta et al., 30 who categorized grades 0 and 1 as low renal echogenicity grades and reported that they had a high degree of diagnostic utility in ruling out an HIVAN diagnosis on the basis of CD4+ count. In spite of this, we suggest that a renal echogenicity of grade 1 for an AIDS patient who is yet to commence treatment could be a strong indicator of mild renal damage orchestrated by HIVAN, as previously suggested.18,20
The role of grade 2 renal echogenicity in predicting an HIVAN diagnosis appeared quite ambiguous in the present study because it had an AUC of 0.70 and overall accuracy of 0.62 (Table 5 and Figure 5). It also had low sensitivity (0.56) but high specificity (1.0). Although the present study’s AUC suggests that it is a good diagnostic model, its sensitivity (0.56) is barely above average. Therefore, a renal echogenicity of grade 2 may, in actual fact, be unable to truly detect HIVAN in the cohort studied. A diagnostic model is perfect for detecting positive patients when its sensitivity (also known as the true positive rate) is equal to 1. If the sensitivity were equal to 0.5, the diagnostic model would not be considered good enough because such an average sensitivity is merely equivalent to a random coincidence. With high specificity, low sensitivity, and a slightly above average overall accuracy (0.62), we submit that a grade 2 kidney echogenicity score was equivocal in the prediction of an HIVAN diagnosis on the basis of CD4+ count in the present study. This conclusion is in agreement with Atta et al.’s 30 opinion that an echogenicity grade 2 score is not helpful in establishing or excluding the diagnosis of HIVAN.
On the basis of CD4+ count, grade 3 renal echogenicity was accurate in detecting severe immunosuppression and, by extension, was useful in predicting an HIVAN diagnosis as shown by the operating characteristics of the ROC curve (Table 5 and Figure 5). Its overall accuracy and sensitivity in predicting an HIVAN diagnosis were 0.84 and 0.87, respectively. With this result, we submit that a grade 3 renal echogenicity was not equivocal in predicting an HIVAN diagnosis on the basis of CD4+ count in the population studied. Others have earlier reported that grade 3 renal cortical echogenicity had the highest potential to diagnose HIVAN.30,31 The present study also supports the notion that grade 3 renal cortical echogenicity is the most consistent sonographic feature of the kidney in advanced AIDS.7,27 It is also instructive to note that there was complete loss of corticomedullary differentiation (Figure 2) in all the patients with grade 3 renal echogenicity in the population studied. These results are thus in alignment with the opinion of some investigators who had previously reported that an increase in renal echogenicity and marked loss of corticomedullary architecture are distinctive of HIVAN.18,20
Sonography was accurate in predicting an HIVAN diagnosis at different cutoff levels of renal echogenicity on the basis of serum creatinine levels and GFR, as shown by ROC curves with their operating characteristics (Tables 6 and 7 and Figure 6). In fact, the AUC (≈ 1; P < .0001), sensitivity, and specificity (0.983 and 1.00, respectively) were excellent for each grade of renal echogenicity. These results showed that sonography was an excellent predictor of an HIVAN diagnosis on the basis of serum creatinine levels or GFR at different cutoff levels of renal echogenicity in the present study. This implies that sonography could be more accurate in predicting an HIVAN diagnosis on the basis of serum creatinine and/or GFR than on the basis of CD4+ count.
When the accuracy of different grades of renal echogenicity in predicting an HIVAN diagnosis on the basis of CD4+ count, serum creatinine levels, and/or GFR was compared, sonography was good at predicting an HIVAN diagnosis in the present study. It is, however, instructive to point out that although each echogenicity score or a combination of scores was accurate, grade 3 renal echogenicity alone was more accurate (overall accuracy = 0.98) in predicting an HIVAN diagnosis. This study supports Atta et al., 30 who had earlier posited that a renal echogenicity grade 3 taken alone had higher specificity (0.95) than grade 2 alone or grade 2 or 3 taken together. In their view, the sensitivity and negative predictive value of sonography as a diagnostic model for HIVAN were highest when defining HIVAN as grades 2 and 3 renal echogenicity, whereas its specificity and positive predictive value were highest when defining HIVAN as grade 3 only. In the present study, however, specificity and positive and negative predictive values either for grade 3 alone or for 2 and 3 taken together were similar. The difference in sensitivity and specificity may be connected to the fact that renal echogenicity was correlated with CD4+ count, serum creatinine level, and GFR in the present study, whereas Atta et al. 30 correlated renal echogenicity with biopsy findings in their study.
A major limitation of this study was that renal biopsy/histopathology, which is the gold standard for HIVAN diagnosis, was not completed. Generalizability of results may also be limited by the sample because Nigeria is a country of 170 million people with a diverse incidence of HIV/AIDS. The sample in the present study, however, appears to be one of the largest samples drawn from a solely African HIV/AIDS population. Subjective grading of renal echogenicity is another limitation of the present study. Quantification of renal echogenicity could have made the present study more objective and more translatable.
Conclusion
Apathy to voluntary HIV/AIDS screening and late presentation of patients are quite high; hence, the HIV/AIDS pandemic continues to be a major threat to socioeconomic activities in the metropolitan city of Lagos. Renal parenchymal disease characterized by enlarged kidneys with complete loss of corticomedullary differentiation may be rampant among AIDS patients. Sonographic renal echogenicity grading appears to be more accurate in predicting an HIVAN diagnosis on the basis of serum creatinine level/GFR than on the basis of CD4+ count. Grade 3 renal echogenicity was the most accurate in predicting an HIVAN diagnosis in this cohort of AIDS patients, who were yet to commence antiretroviral treatment.
Footnotes
Acknowledgements
We are grateful to participants in the study for their understanding and patience. We also wish to thank Ms. Hope Onoshevwe for analyzing our data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.