
Abstract
Endometrial carcinoma is the most commonly diagnosed malignancy in the female reproductive tract, mainly affecting women in their postmenopausal years. Although rare, it can also present in premenopausal women. The most common clinical presentation is episodes of abnormal uterine bleeding. Magnetic resonance imaging (MRI), computed tomography (CT), and sonography are imaging modalities used to detect endometrial carcinoma. However, a conclusive diagnosis is made through endometrial biopsy. A case is reported of endometrial distension with endometrial carcinoma and cervical stenosis listed as differentials and originally detected through CT. Sonographic assessment showed an irregular thickened endometrium and an endometrial cavity containing fluid with low-level echoes and areas of polypoid mass-like tissue. Based on these findings, the patient underwent an endometrial biopsy that provided confirmation of endometrioid adenocarcinoma (International Federation of Gynecology and Obstetrics [FIGO] Stage 1).
Keywords
Endometrial carcinoma is the most common type of gynecological cancer whose incidence is increasing. Reports indicate that about 40 100 new cases were diagnosed in 2008, and 52 630 new cases were diagnosed in 2014 in the United States.1–3 This malignant disease affects approximately 1 in every 50 women, with most of the cases presenting in postmenopausal women. 1 Endometrial carcinoma has an unknown etiology. The most common clinical sign is abnormal uterine bleeding. Histologically, the most common subtype of endometrial carcinoma is endometrioid adenocarcinoma, which accounts for 75% of endometrial carcinoma cases.1,3 Endometrial carcinoma is curable with early diagnosis; however, the treatment and prognosis depend on the stage of the tumor at the time of diagnosis. Diagnosis can only be made through an endometrial biopsy. 3
Case Report
A 65-year-old female presented to the emergency department with nausea and vomiting along with dizziness and generalized abdominal pain. These symptoms had been present for two weeks. The patient also reported vaginal bleeding for approximately six months to a year. Patient was unsure of the exact onset of the vaginal bleeding. Patient had a medical history of interstitial lung disease, status post right lung transplant, diverticulitis, GERD, hypertension, and hyperlipidemia. Based on her symptoms, an abdominal-pelvic computed tomography (CT) exam was ordered. The CT findings included a prominent distention of the endometrial cavity (Figure 1). Endometrial cancer and cervical stenosis were listed as differentials. Based on these findings, a pelvic sonogram was suggested to further evaluate the endometrial cavity.
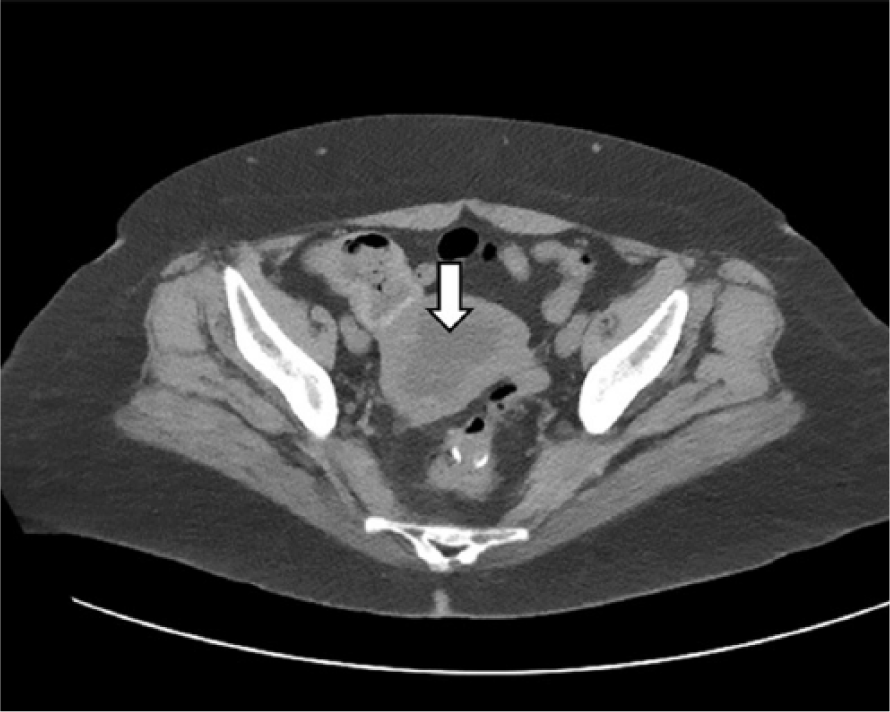
Axial computed tomogram with contrast of the pelvis showing prominent distention of the endometrial cavity (arrow).
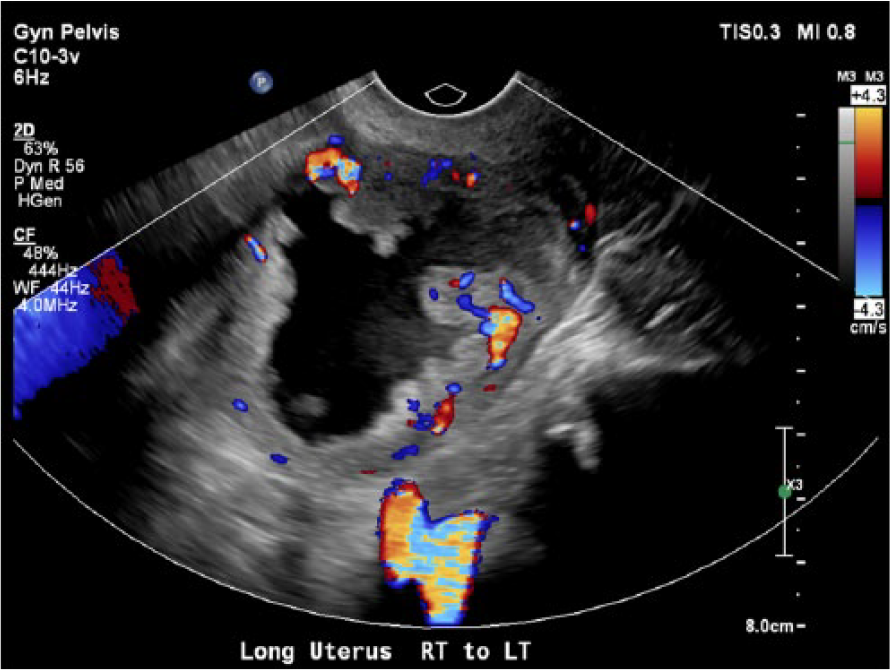
A transabdominal and transvaginal pelvic sonogram was performed using Philips EPIQ 7G (Philips Healthcare, Bothell, Washington) with a C5-1 MHz curvilinear array transducer and a C10-3v MHz transvaginal transducer. The pelvic sonogram demonstrated normal ovarian sonographic appearance, normal bilateral adnexa, and no free fluid in the pelvis. The uterus was regular in contour and measured 8.4 cm in length and 7.2 cm in width (Figures 2 and 3). The myometrium appeared thin and heterogenous with normal vascularity (Figure 4). The endometrium appeared irregularly thickened with areas of polypoid mass-like soft tissue measuring up to 1.9 cm in length (Figures 5 and 6). The endometrial cavity was distended with fluid containing low-level echoes (Figure 7). The cervix also appeared to be indistinct and inseparable from the endometrial mass with mild expansion of the internal os (Figure 8). No cervical measurement was obtained during this exam. Color Doppler evaluation demonstrated significant peripheral vascularity of the endometrium and within the polypoid mass-like soft tissue areas (Figure 9). Based on the sonographic findings that correlated with the CT findings, an endometrial biopsy was recommended.

Longitudinal gray-scale image showing the uterus length at 8.4 cm and regular borders.

Transverse gray-scale image demonstrating the uterus width at 7.2 cm.
Longitudinal gray-scale with color Doppler showing a thin heterogenous myometrium with normal vacularity.

Transverse gray-scale image of the uterus showing irregular thickened endometrium with areas of polypoid mass-like soft tissue.
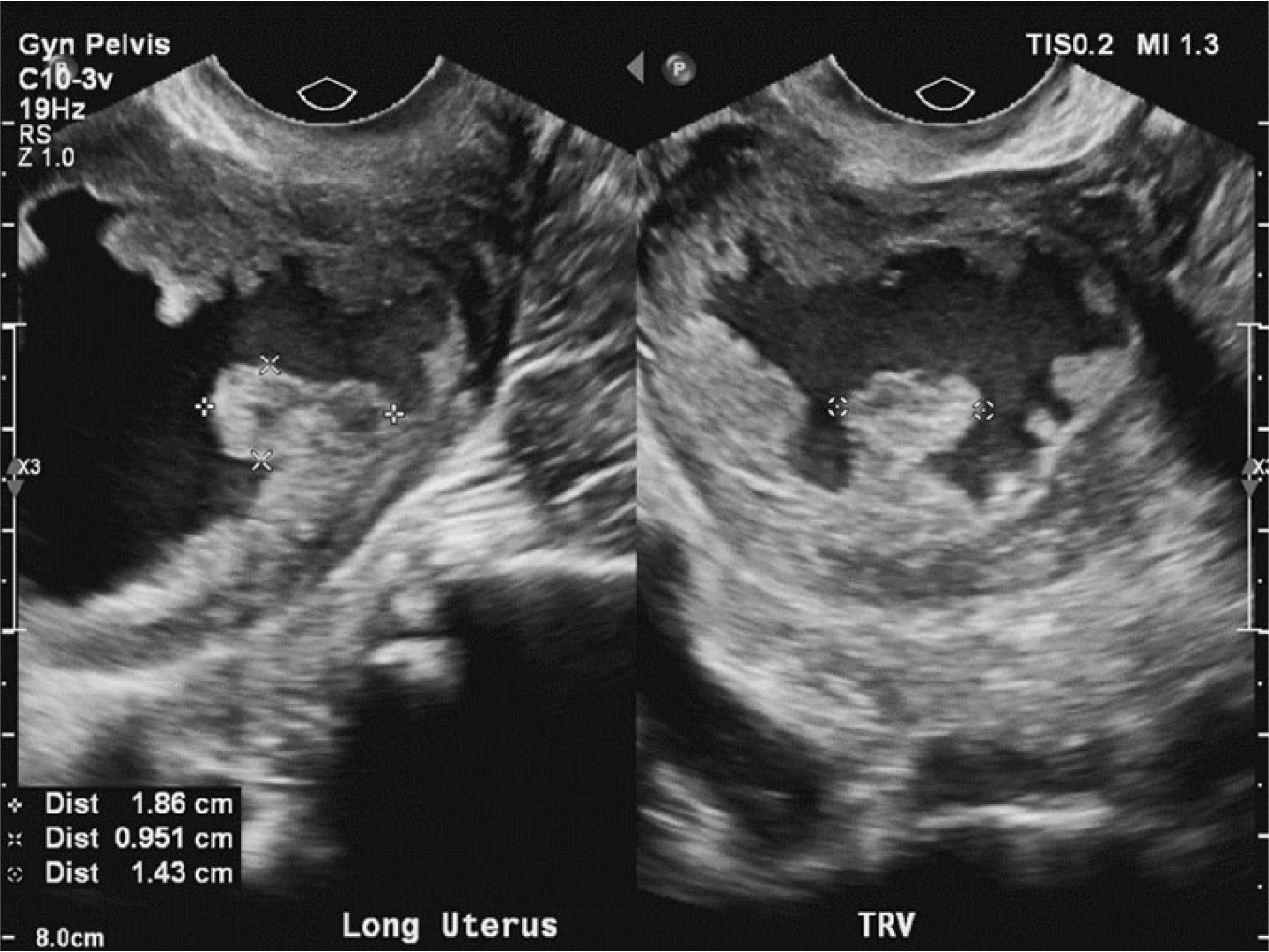
Transverse and longitudinal gray-scale image of the uterus showing the endometrial polypoid mass-like soft tissue measuring 1.9 × 1 × 1.4 cm.

Longitudinal gray-scale image of the uterus demonstrating the distention of the endometrial cavity with fluid containing low-level echoes and posterior enhancement.

Longitudinal gray-scale image of the uterus showing the cervix as indistinct and inseparable from the mass with mild expansion of the internal os.
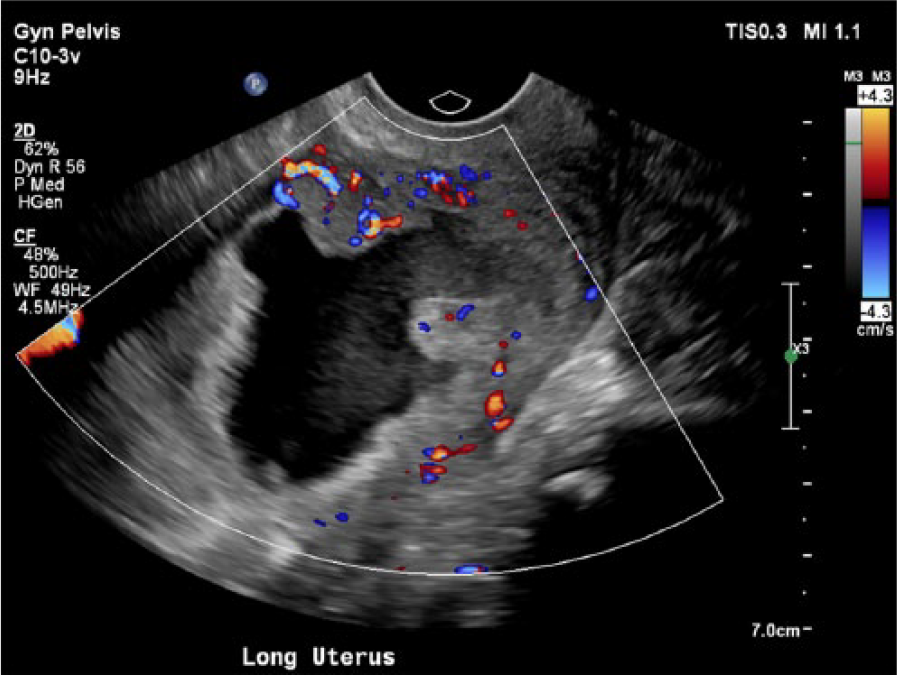
Longitudinal gray-scale image with color Doppler depicting significant peripheral vascularity of the endometrium and within the polypoid mass-like soft tissue areas.
An endometrial biopsy was performed two days after the initial imaging studies. During the biopsy, a sterile speculum was placed into the vaginal canal. The cervix was prepped with betadine and distended to 1 cm. Seven passes of an endometrial pipelle resulted in extraction of serosanguinous tinged/clean fluid. As the patient was stable and tolerant, 3 more passes of the pipelle were performed with a small amount of tissue extracted. All fluid and tissue sampled were sent to the pathology lab. The specimen examined consisted of a 2.7 × 2.2 × 0.6 cm aggregate of hemorrhage, tissue, and blood fragments mixed with coagulum and mucus. The pathology report indicated endometrioid adenocarcinoma and was classified by the International Federation of Gynecology and Obstetrics (FIGO) as Stage I. The patient underwent robotic-assisted hysterectomy and bilateral salpingo-oophorectomy days later. No follow-up information was available.
Discussion
Endometrial carcinoma typically presents in the postmenopausal years with an average of age of 59 years old. However, 2% to 14% of the cases affect women in their premenopausal period of less than 40 years of age.4,5 It is the most common type of gynecologic malignancy in developed countries, with an increasing incidence affecting approximately 1 in every 50 women. 6 Histologically, the most common type of endometrial carcinoma is endometrioid adenocarcinoma, also known as endometrial carcinoma type 1.1,5 This type of tumor develops from the epithelial cells found in the endometrial glands. Nonendometrioid carcinoma, also known as type II endometrial carcinoma, resembles clear cell or ovarian serous adenocarcinoma. Type II endometrial carcinomas are considered high-grade tumors and have a worse prognosis.5,7 The exact etiology of this malignancy is unknown. The risk factors associated with endometrial carcinoma are obesity, nulliparity, diabetes, hypertension, endometrial hyperplasia, inherited forms of colorectal cancer, unopposed estrogen stimulation, tamoxifen, and polycystic ovarian syndrome.4,8 Estrogen is thought to increase by the inactivation of gene PTEN (phosphate therapy and tensin homologue), a tumor suppressor in patients with cancer. This inactivation of the PTEN gene allows for the proliferation of normal and neoplastic cells within the endometrium. 7 Tamoxifen is used as an estrogen antagonist in breast cancer patients but acts as an estrogen agonist in the uterus, allowing the proliferation of cells in endometrial tissue. 6 This proliferation of tissue leads to the most common clinical symptom, postmenopausal bleeding. Patients can also present with abdominal or pelvic pain and abdominal distension.1,9
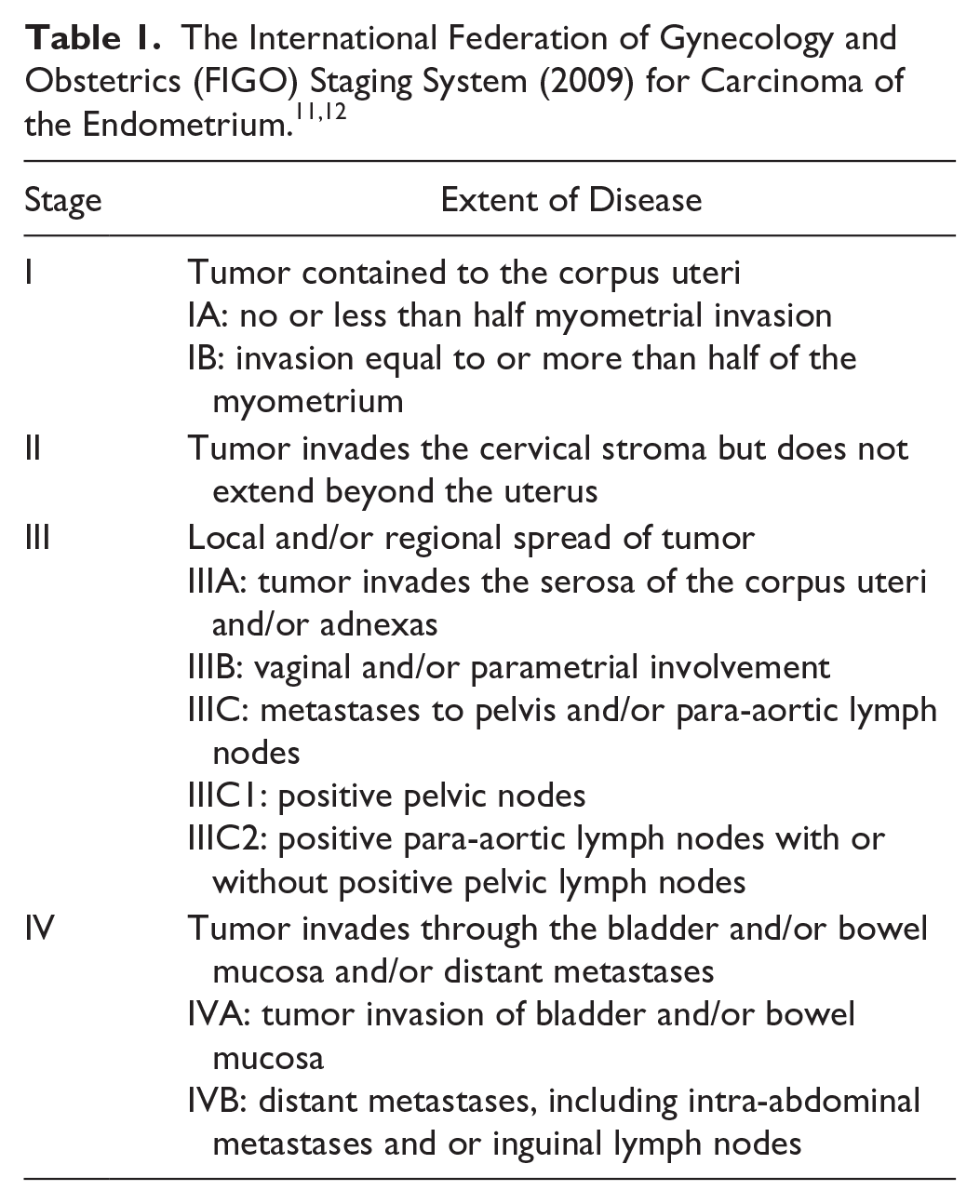
Most cases of endometrial carcinoma are diagnosed in the early stage of the disease.2,10 The FIGO criteria, revised in 2009, describes four stages of endometrial carcinoma. Stage I: Carcinoma is contained within the uterus. Stage II: Carcinoma extends into the cervix and myometrium. Stage III: Carcinoma invades through the serosa of the uterus pelvic area and pelvic or para-aortic lymphadenopathy. Stage IV: Carcinoma invades the bladder or rectum, outside the pelvis, and distant organs (Table 1).11,12
Sonography is the initial imaging tool used for abnormal vaginal bleeding, and it also plays an important role in screening for abnormal endometrial thickness and the visualization of the depth of myometrial invasion with an 88% sensitivity. 9 The normal sonographic appearance of the endometrium is described as homogenous, even in thickness, with no displacement by abnormal surrounding structures.5,6,14 The sonographic findings associated with endometrial carcinoma are an irregular thickened and heterogenous endometrium, trapped blood in the uterine cavity (hematometra), and an enlarged uterus. It can also present as an endometrium with a mass-like appearance. 14 A transvaginal sonogram may better demonstrate myometrial invasion as an irregular thickened central endometrial interface with hypoechoic/echogenic areas within the endometrium and hyperechoic areas in the myometrium. 14 Normal endometrium measurement in premenopausal women varies depending on the hormonal phase of the menstrual cycle ranging from 4 mm to 14 mm. However, the endometrium atrophies after menopause and usually measures less than 8 mm. 14 In postmenopausal women with abnormal uterine bleeding and no history of hormone replacement therapy (HRT), an endometrium measuring greater than 4 to 5 mm could be indicative of endometrial carcinoma.6,14 Color Doppler may demonstrate increased vascularity within the endometrium or the myometrial invasion. In addition, sonography is helpful in differentiating between tumors limited to the uterus or tumors with extrauterine invasion.5,7,14 In a recent study, 3D sonography in conjunction with power Doppler demonstrated its utility in cases of endometrial carcinoma. Three-dimensional sonography can obtain an endometrial volume (EV) in all planes and power Doppler vascular information within the area of interest in the endometrium. 15 The pitfalls of sonography when evaluating the endometrium and uterus are body habitus and bowel gas.
Magnetic resonance imaging (MRI) and CT are useful imaging modalities in the diagnosis of endometrial carcinoma. Magnetic resonance imaging is the gold standard for staging of endometrial carcinoma because it gives important information about the size and extent of the tumor yet sometimes lacks the ability to accurately detect myometrial and cervical invasion and metastases to lymph nodes. 12 Computed tomography can provide information about lymph node metastases, although poor sensitivity and specificity in the detection of tumor metastases to lymph nodes, cervix, and myometrium have been reported. 13 Although imaging tools are useful, the only definitive diagnosis can be through endometrial biopsy.
The treatment and prognosis depend on the stage of the carcinoma at the time of diagnosis. Because most cases (75%-80%) are found at Stage I (malignancy is confined to the endometrium/uterus), patients have a favorable treatment and prognosis.9,12 The type of treatment for endometrial carcinoma considers the age of the patient, health of the patient, and degree of invasion. 6 The most common treatment in postmenopausal women is surgical intervention through total hysterectomy and bilateral salpingo-oophorectomy. After the removal of the uterus, myometrial and cervical invasion is investigated through pathology. Chemotherapy and radiation is recommended in cases of tumor metastases or deep myometrial invasion. In cases of metastases to lymph nodes, malignant lymph nodes may be removed. For women of childbearing age, with endometrial carcinoma Stage IA with no myometrial invasion, progestin therapy is a more conservative treatment over radical surgery; however, there is a risk of tumor recurrence. In cases of advanced endometrial carcinoma, palliative therapy such as the use of progestins is recommended. Gn-RH (gonadotropin-releasing hormone) agonists are used to manage the recurrence and metastases of the disease after failure of surgery or radiotherapy.4,9 The prognosis for patients is good in cases that are provided an early diagnosis. The five-year survival rate in patients with Stage I endometrial carcinoma is 95%. 1 Satisfactory prognosis decreases in those patients with advanced or recurrent tumors. The five-year survival rate of endometrial carcinoma for patients with Stage III is 59.6%. Endometrial carcinoma has 15% to 20% tumor recurrence occurring after surgery. Routine clinical follow-up is recommended to patients with a history of endometrial carcinoma for the management and recurrence of the disease.1,13
Conclusion
Endometrial carcinoma is the most common malignancy in the female reproductive tract. It predominantly affects postmenopausal women; however, a small percentage of premenopausal women are affected by this disease. The exact etiology is unknown. The main clinical presentation is abnormal uterine bleeding. There are many risk factors associated with endometrial carcinoma. This case study demonstrates the importance of utilizing sonography in the evaluation of endometrium thickness and myometrial invasion as it could assist in differentiating between tumors confined to the uterus and those with extra-uterine invasion. An early diagnosis and expedited treatment at an earlier stage of the disease provides a better prognosis for the patient.
Footnotes
Acknowledgements
The author would like to thank and recognize Lynn Schluns, BS, RDMS, RVT, El Centro College DMS program coordinator, for providing the opportunity and support to write this article. Special thanks to my mentor, Maria Johnson, RVT, RDMS, who provided essential feedback and guidance.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.