
Abstract
Zenker diverticulum, also known as a pharyngeal pouch, is the most common type of esophageal diverticulum. While sonography is not the imaging modality of choice for diagnosis of a suspected diverticulum, it is not uncommon to detect during a sonographic examination. Typically, a Zenker diverticulum is located in close proximity to the left thyroid gland.
Keywords
Zenker diverticulum is the most common type of esophageal diverticulum. It is located in a natural area of weakness on the posterior pharyngeal wall, in an area known as the Killian triangle. 1 Although Zenker diverticulum is a posterior structure, if large enough, it may project to the left side of the neck. They often appear in close proximity to the left thyroid,2,3 as presented in this case.
Case Report
A 75-year-old man was referred to the sonography department for surveillance of known thyroid nodules. He presented with a complaint of neck tenderness and chronic dysphagia with solid foods. His symptoms had persisted for approximately 1 year.
A detailed sonographic evaluation was performed using a Philips IU-22 ultrasound system (Philips Medical, Bothell, Washington) with a L12-5 MHz and a C8-5 MHz transducer. The sonogram showed unchanged bilateral thyroid nodules. The right thyroid nodule met criteria for a fine-needle aspiration (FNA). Images of the left thyroid showed a 20-mm × 16-mm air-filled structure, adjacent to the thyroid in the area of the expected esophagus (Figures 1 and 2). When the patient swallowed, air was visible moving through this structure.
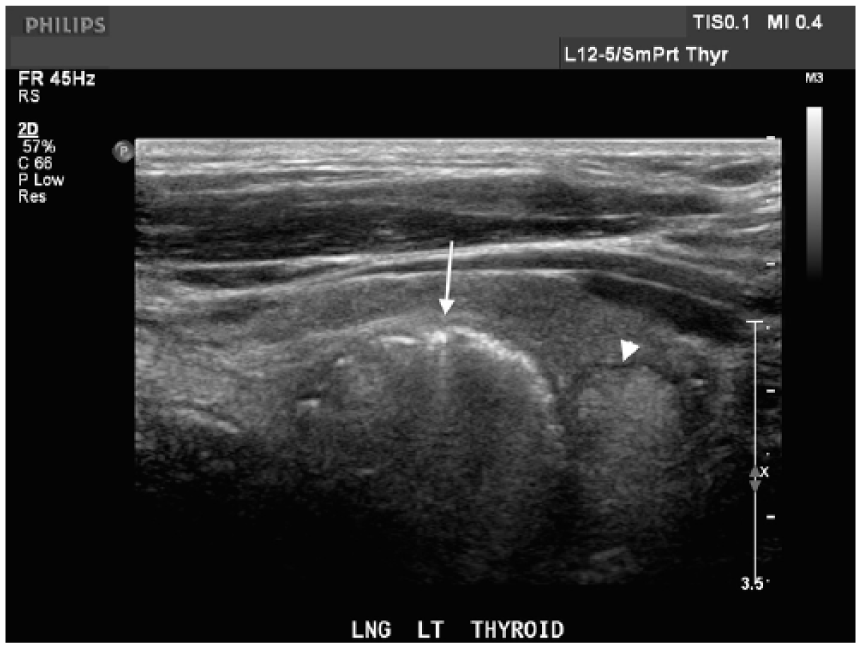
Longitudinal sonogram of the left neck demonstrates an air-filled Zenker diverticulum (arrow) in the expected area of the left thyroid. The left thyroid nodule (arrowhead) is also demonstrated.
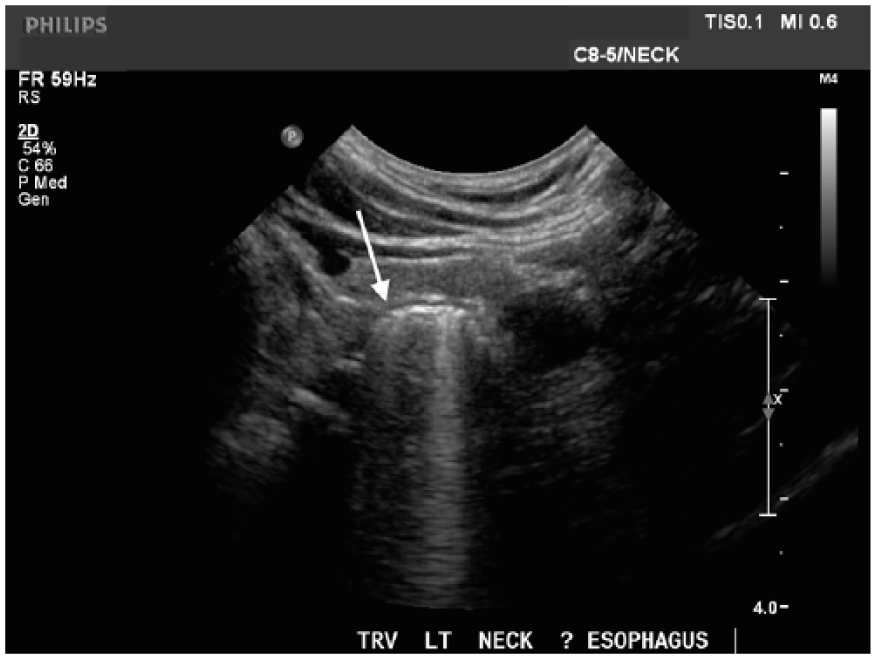
Transverse sonogram of the left thyroid gland with the Zenker diverticulum in the expected area of the esophagus (arrow). The diverticulum is filled with air; note the dirty shadow demonstrated.
After the sonogram, additional tests were performed. A FNA of the right thyroid nodule determined it was a benign follicular nodule. The patient also had a barium swallow fluoroscopic study of the esophagus. The esophagogram demonstrated an esophageal stricture, hiatal hernia, and a 17-mm × 10-mm esophageal Zenker diverticulum (Figure 3). A few months later, the patient returned for an esophageal biopsy. The biopsy incidentally revealed a diagnosis consistent with Barrett esophagus without dysplasia. No further follow-up was available for this patient at the time of this case report.

Barium swallow esophagram demonstrating barium-filled diverticular sac (arrow) on the left side of the patient’s neck. This fluoroscopic study confirmed the sonographic findings.
Discussion
Zenker diverticulum is also known as cricopharyngeal or pharyngoesophageal diverticulum. It is the most common type of esophageal diverticulum. It is located in a natural area of weakness on the posterior pharyngeal wall just proximal to the upper esophageal sphincter, in an area known as the Killian triangle.1,4 Although Zenker diverticulum is a posterior structure, if large enough, it may project to the left side of the neck. They often appear in close proximity to the left thyroid gland.2,3
Zenker diverticula are thought to be acquired as a result of increased intrapharyngeal pressure from premature closure of the cricopharyngeal sphincter before pharyngeal contraction. This results in protrusion of mucosa.2,4 The diverticular pouch includes only mucosa and submucosa and thus should be considered a pseudodiverticulum. 1
Zenker diverticula occur most commonly in the elderly population, typically in the seventh and eighth decades of life. Patients are rarely affected before the age of 40; this is thought to be due to loss of tissue elasticity and decrease in muscle tone with age. 5 Most patients affected with this entity are men.1,4,5
As the diverticular sac enlarges, it will typically become symptomatic for the patient.5,6 If the sac is large enough, it may be palpated as a mass of dough-like consistency on a physical examination. The most common clinical symptom is dysphagia, occurring in approximately 80% to 90% of patients.1,4,5 Other common symptoms include retention of food in diverticula, spontaneous regurgitation of undigested food, noisy swallowing, malnutrition, voice changes, and halitosis. Respiratory complications may include hoarseness, asthma, pneumonitis, and lung abscess.4,7 The most serious complication is pulmonary aspiration. 1
Some cases of Zenker diverticula will be found incidentally on imaging studies of the neck. Sonography, computed tomography, and a barium swallow esophagram are the most common examinations to detect a diverticulum. A sonographer performing a sonographic examination of the neck might overlook the diverticulum or mistake it for a thyroid nodule. This case provides sonographic features of this diverticulum as a helpful reminder. As with the appearance of thyroid nodules, sonographic findings of an esophageal diverticulum may vary. The most common finding is a nodule consisting of a rounded hyperechoic mass with a hypoechoic wall. There may be unclear borders and multiple relatively strong punctate echoes. Microcalcifications in thyroid nodules also appear as multiple strong punctate echoes.3,8–10 There will not be any detectable blood flow in the diverticula, whereas Doppler can be used to evaluate blood flow in a thyroid nodule. 8 Esophageal diverticula may have fluid and debris simulating a complex thyroid cyst, hemorrhagic adenoma, or abscess. A thyroid abscess is very rare, as the thyroid is quite resistant to infection. Thyroid abscess will also have associated fever and pain.2,10
Dynamic sonographic imaging is especially helpful in the diagnosis of a Zenker diverticulum. Demonstration of the nodule with the patient swallowing or drinking water will show movement of contents (air, water, debris) to and from the diverticular sac. Drinking water is typically the most useful way to detect movement.2,8 Compression with the ultrasound transducer may also be beneficial to change the shape and echogenicity of the lesion.
A barium swallow esophagram is typically used to confirm a diagnosis of a suspected diverticulum. It will reveal a wide-neck outpouching at the posterior aspect of the pharyngealesophageal junction. The outpouching retains barium.7,8 Once the diverticulum is established, it progresses in size (sac diameter elongates and descends), 7 and therefore routine surveillance is recommended. The American College of Radiology’s appropriateness criteria rate the barium swallow esophagram as the best diagnostic examination for dysphagia. 11
Treatment options for the diverticulum vary according to location, symptoms, and size. 12 Treatment is typically indicated for all symptomatic patients with or without associated complications. 4 Ideally, treatment should be done electively before nutritional and respiratory complications have time to develop. If perforation occurs, treatment then becomes a surgical emergency. 7 Treatment approaches of the diverticular sac have evolved over the years. For decades, an open surgical approach was performed. It consisted of a neck incision and myomotomy of the upper esophageal sphincter, as well as removal or suspension of the diverticulum. Today, a much less invasive transoral endoscopic technique is used with endoscopic stapling, diverticulectomy, or diverticuloplexy used to treat the diverticular sac.1,12
This case also included an incidental diagnosis of Barrett esophagus. While this is not a typical finding with Zenker diverticula, the most common symptom, dysphagia, is present with both. Barrett esophagus is most commonly caused by chronic reflux esophagitis. It is considered a premalignant condition, and therefore routine surveillance is recommended. These patients have a 30 to 40 times greater risk than the general population of developing esophageal cancer. 13
Conclusion
This case demonstrated the importance of sonographic imaging that includes not only the thyroid gland but also the surrounding structures during an examination of the neck. It is important to be aware of the sonographic findings of Zenker diverticulum. While routine surveillance and diagnosis of suspected diverticula are done with a barium swallow esophagram, the use of sonography for identifying incidental diverticula during a thyroid sonogram is very important.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.