
Abstract
This study assessed the performance of a pocket-sized ultrasound system for the diagnosis of proximal lower limb acute deep vein thrombosis (DVT) compared to a full-sized ultrasound system. Patients who needed urgent lower limb sonograms for acute DVT were invited for the study. In each examination, the investigator scanned the patient using the pocket-sized system and then repeated the scan using the full-sized system. The sensitivity, specificity, and accuracy of the pocket-sized system were determined in reference to the full-sized system. The venous segments that failed to be visualized using the two systems were compared. One hundred lower limbs comprising 500 venous segments were examined. There were four venous segments, including two mid and two lower femoral veins in two patients who failed to be visualized using both systems. The sensitivity, specificity, and accuracy for diagnosing proximal lower limb acute DVT were 100% (95% confidence interval [CI], 94.94%–100%), 100% (95% CI, 99.05%–100%), and 100% (95% CI, 99.19%–100%), respectively. The pocket-sized ultrasound system and the full sized-ultrasound system demonstrated a comparable performance in detecting acute DVT in the leg.
With technological advancement, battery-powered pocket-sized ultrasound systems became commercially available in the late 1990s. These ultrasound devices are relatively inexpensive compared with full-sized systems. Moreover, they are much smaller and lighter, so they could be easily carried everywhere, thus rendering sonography readily available for bedside and acute care applications.
Lower limb acute deep venous thrombosis (DVT) is a significant medical condition that can potentially lead to life-threatening pulmonary embolism. 1 Contrast X-ray venography is the traditional gold standard for diagnosing lower limb DVT, but these examinations are seldom performed today.1 –4 Sonography is now widely accepted as cost-effective and the preferred imaging modality for investigating acute DVT.2 –7 A meta-analysis found that sonography has a high sensitivity (range, 93.2%–95.0%; pooled sensitivity, 94.2%) and a high specificity (range, 93.1%–94.4%; pooled specificity, 93.8%) for diagnosing proximal lower limb DVT but a much lower sensitivity for distal lower limb DVT (range, 59.8%–67.0%; pooled sensitivity, 63.5%). 7
An early diagnosis of lower limb DVT is crucial for patient management. In this regard, a pocket-sized ultrasound system may serve as a readily available technology facilitating the delivery of a timely diagnostic imaging examination. Pocket-sized ultrasound systems have been evaluated in many studies for their applications in many fields such as cardiac, abdominal, obstetric, and gynecological imaging, but very few studies investigate their application for detecting venous thrombosis.8 –13 This study aimed to evaluate the performance of a pocket-sized ultrasound system in the diagnosis of acute DVT in the proximal lower limbs compared to a full-sized ultrasound system.
Methods
Study Design and Participants
This was a single-center prospective study adopting a convenience sampling strategy. This study was conducted in the Department of Radiology of an acute care hospital with more than 1500 beds accepting urgent referrals from all clinical specialties. Adult patients referred for urgent sonographic examinations for suspected lower limb acute DVT were invited for the study until 100 lower limbs were examined.
Ethical approval was obtained from the Institutional Research Ethics Board, and written informed consent was obtained from the participants.
Ultrasound Systems
The pocket-sized ultrasound system used was a General Electric Vscan equipped with a dual probe, which consists of a phased-array transducer on one end and a linear-array transducer on the other (GE Healthcare, Wauwatosa, WI). The linear-array transducer, covering a frequency bandwidth of 3.4 to 8 MHz, was used. The standard ultrasound system employed was a Philips iU22 Ultrasound System (Philips, Bothell, WA), using a L9-3 linear array transducer (frequency bandwidth: 9 MHz–3 MHz) covering a similar frequency bandwidth.
Investigators
Each examination was performed by one of the three investigators consisting of two radiologists and one registered vascular technologist, with all of them having more than 10 years’ experience in diagnostic sonography practice.
The Examinations
According to the American College of Radiology (ACR) Appropriateness Criteria, the major sonographic diagnostic criterion for acute DVT is the failure of complete compression of the venous walls when pressure is applied to the skin on real-time grayscale imaging. 5 As also mentioned in the criteria, color Doppler can be used for characterizing a thrombus as obstructive or partially obstructive, and an augmentation test using duplex ultrasound can rarely provide additional information for diagnosis.5,14 In a prospective study of 1980 patients investigating lower extremity DVT by using venous augmentation, all blood clots were first detected by compression on grayscale imaging, and no additional DVT was discovered by augmentation. 14 Augmentation only facilitated the visualization of the veins or the detection of slow flow. 14 Due to the limited roles of color Doppler and augmentation for the diagnosis, we adopted the compression test as the diagnostic criterion for acute DVT in this study.
As in line with our department protocol, instead of routinely performing bilateral whole lower limbs, only the affected proximal lower limbs were examined in this study. Although we do not include distal lower limbs in our protocol, a serial sonography examination could be performed upon clinical request to exclude proximal extension of distal lower limb DVT.
The proximal lower limb deep veins were divided into five venous segments for sonographic evaluation and statistical analysis:
The common femoral vein in the groin
The upper femoral vein, denoting the segment of the femoral vein in the upper thigh
The mid-femoral vein, denoting the segment of the femoral vein in the mid-thigh
The lower femoral vein, denoting the segment of the femoral vein in the lower thigh
The popliteal vein, behind the knee
The examinations were performed with the patients supine and the affected lower limbs externally rotated and slightly abducted. The venous segments were identified and evaluated with and without compression on transverse real-time grayscale imaging.
For the sake of comparison, each patient was assessed on the same session using both ultrasound systems. To avoid being biased by the results from the full-sized system, the investigator first scanned the patient using the pocket-sized system and then repeated the scan using the full-sized system.
Any venous segments that failed to be visualized and assessed by each ultrasound system were noted. The compressibility of the successfully visualized venous segments was recorded. The depths of the venous segments from the skin surface were measured from the images using electronic calipers.
Statistical Analyses
The sensitivity, specificity, and accuracy of the pocket-sized ultrasound system for diagnosing proximal lower limb DVT were determined using the results from the full-sized system. This was chosen as the reference standard since the aim was to compare the performance of the pocket-sized system with the full-sized system. Moreover, as this study focused on the diagnosis of acute DVT, lower limbs with chronic DVT, either from known clinical histories or from the diagnoses made by the standard ultrasound system, were excluded from statistical analysis.
The proportions of venous segments that failed to be visualized by the two ultrasound systems were compared. These uninterpretable results due to failed visualization would be regarded as invalid inconclusive results, and they would not be included into the cross-tabulation of valid results by acute DVT. 15
The number of any indeterminate results for the diagnosis of acute DVT in the successfully visualized venous segments for the two systems would be compared and included in the analysis for sensitivity, specificity, and accuracy.
The statistical tests were performed using an online free open-source software OpenEpi (version 3.01) provided by Open Source Epidemiological Statistics for Public Health. 16
To ensure a sufficient statistical power for the study, a sample size estimation was performed. Since the basic unit for our analysis is an individual venous segment, we needed to know the prevalence of DVT in the lower limb venous segments for the sample size calculation. However, most studies in the literature provided the prevalence in terms of the proportion of patients who had DVT. Therefore, we conducted a retrospective review of 50 ultrasound examinations for the incidence of acute DVT in the lower limb venous segments in our center, and a prevalence of 16% was found. Accordingly, assuming the sensitivity and specificity of both to be 95%, for a precision of 5% and an estimated prevalence of 16%, a sample size of 456 venous segments is required at the 95% confidence level. Thus, we planned to examine a total of 100 lower limbs, comprising 500 venous segments in this study.
Results
Five hundred venous segments in 100 lower limbs of 84 patients (mean age: 70; range: 37–96), including 55 females and 29 males, were examined. Chronic DVT was found in five lower limbs in five patients, and these 25 venous segments were excluded.
One hundred percent of the common femoral veins, upper femoral veins, and popliteal veins were successfully depicted by both ultrasound machines. However, four venous segments, including two mid-femoral veins and two lower femoral veins in two patients, failed to be depicted by the pocket-sized system due to their deep location resulting from severe lymphedema. These four same venous segments also failed to be visualized using the full-sized ultrasound system for the same reason. The average depth of these four venous segments was estimated to be more than 5 cm from skin, compared to an average depth of about 3 cm for the successfully visualized mid to lower femoral venous segments. Therefore, 97.9% of mid-femoral veins and lower femoral veins were successfully assessed by both ultrasound systems. Overall, 99.2% (471/475) of all venous segments were successfully depicted by both systems, and 0.8% (4/475) failed to be visualized using both systems. Therefore, the proportions of venous segments that failed to be visualized by the two ultrasound systems were identical. For the successfully visualized venous segments, there were no indeterminate results for the determination of acute DVT for both systems. Accordingly, a total of 471 venous segments were included for statistical analysis for sensitivity, specificity, and accuracy.
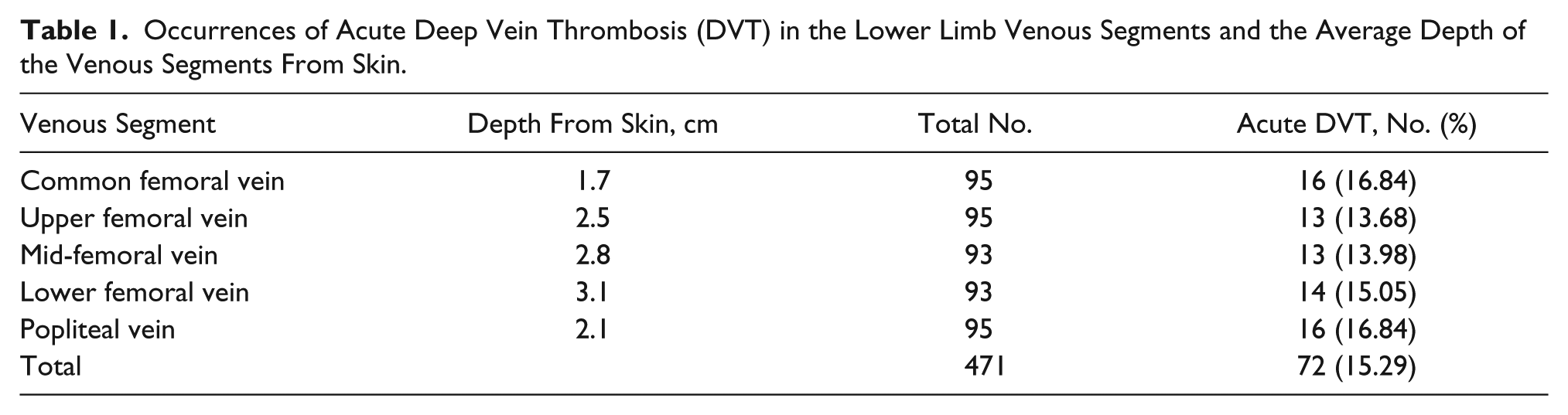
Acute DVT was found in 72 venous segments (72/471, 15.3% of venous segments) in 20 lower limbs of 19 patients (19/79, 24.1% of patients) by the full-sized ultrasound system. The same findings were noted in the same venous segments by the pocket-sized system. For the remaining 399 venous segments with no venous thrombus noted by the full-sized system, congruent results were found by the pocket-sized system. The occurrences of acute DVT in the various venous segments and the depths of the venous segments are summarized in Table 1. Figure 1 is a flowchart showing the results from both ultrasound systems for the determination of diagnostic accuracy of the pocket-sized ultrasound system in diagnosing proximal lower limb acute DVT.
Occurrences of Acute Deep Vein Thrombosis (DVT) in the Lower Limb Venous Segments and the Average Depth of the Venous Segments From Skin.
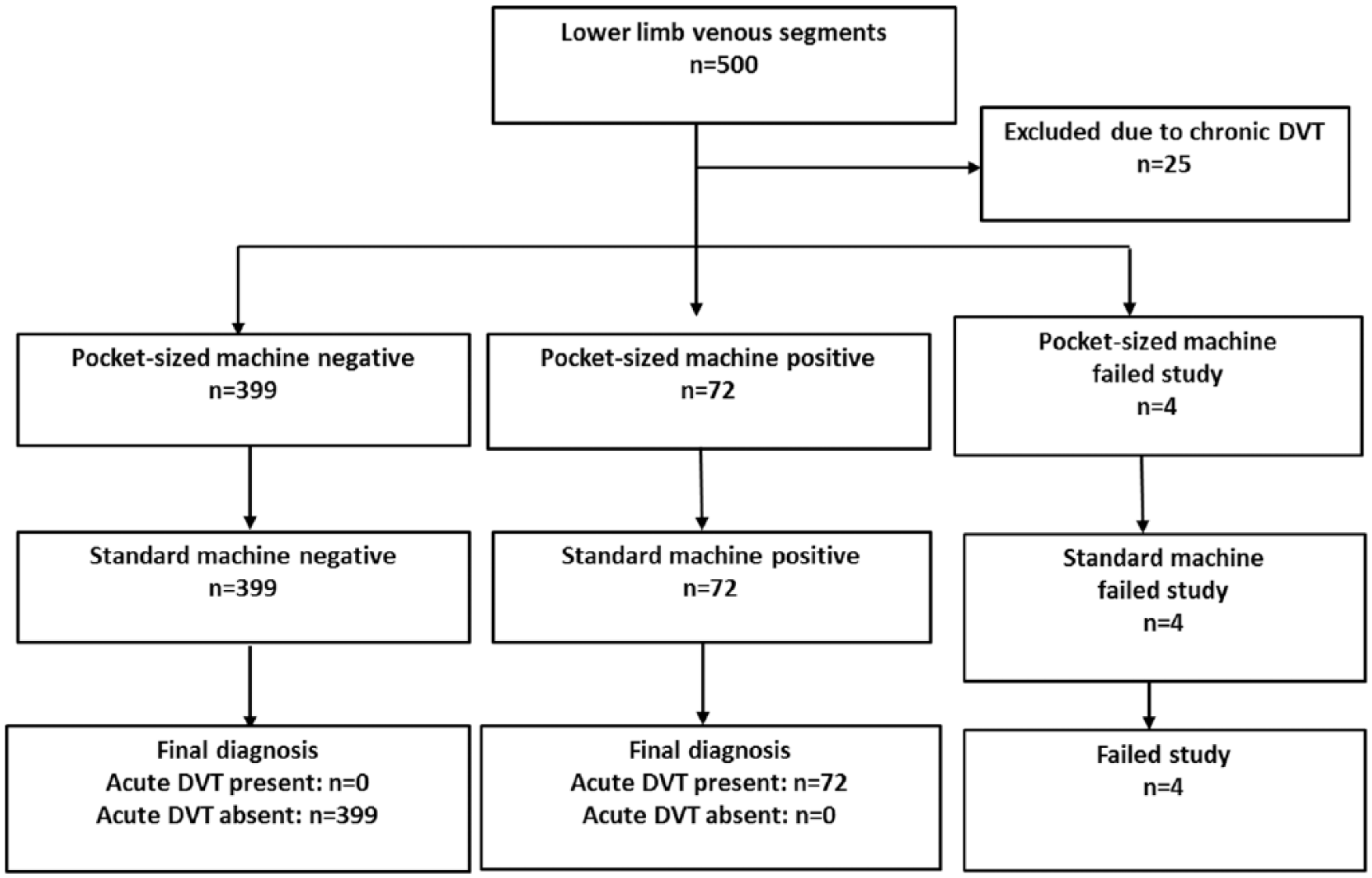
Flowchart showing the results from the pocket-sized and standard ultrasound system in the determination of the diagnostic accuracy of the pocket-sized system in diagnosing proximal lower limb acute deep vein thrombosis (DVT).
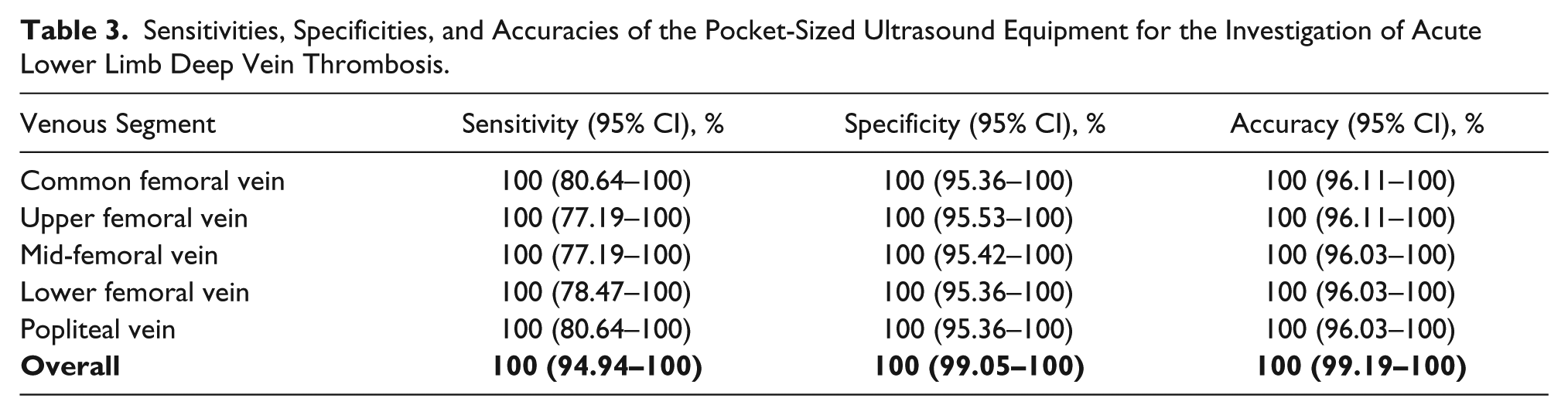
The overall sensitivity, specificity, and accuracy of the pocket-sized machine for the detection of proximal lower limb acute DVT were 100% (95% CI, 94.94%–100%), 100% (95% CI, 99.05%–100%), and 100% (95% CI, 99.19%–100%), respectively. The diagnostic accuracies for the various venous segments were 100% (95% CI, 96.11%–100%) for the common femoral vein, 100% (95% CI, 96.11%–100%) for the upper femoral vein, 100% (95% CI, 96.03%–100%) for the mid-femoral vein, 100% (95% CI, 96.03%–100%) for the lower femoral vein, and 100% (95% CI, 96.03%–100%) for the popliteal vein. A cross-tabulation of the results from the pocket-sized system by the results from the standard system is shown in Table 2. The sensitivities, specificities, and accuracies of the pocket-sized system for proximal lower limb acute DVT in the various venous segments are tabulated in Table 3.
Contingency Table of the Results: Pocket-Sized Ultrasound Equipment vs. Ultrasound Equipment.
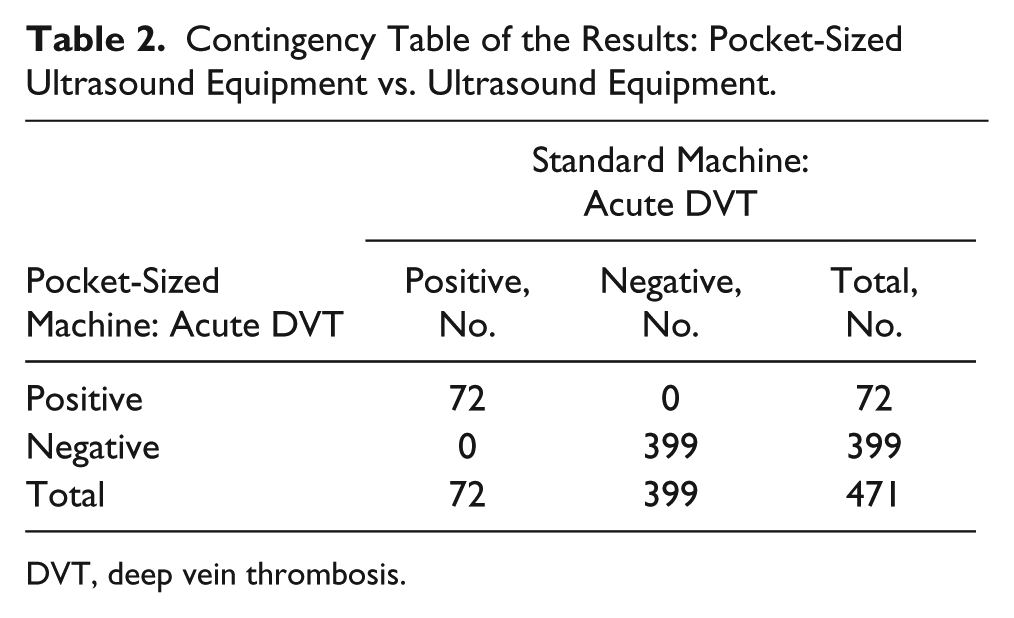
DVT, deep vein thrombosis.
Sensitivities, Specificities, and Accuracies of the Pocket-Sized Ultrasound Equipment for the Investigation of Acute Lower Limb Deep Vein Thrombosis.
The images produced by the pocket-sized and full-sized ultrasound systems are presented in Figure 2 and Figure 3 for comparison.
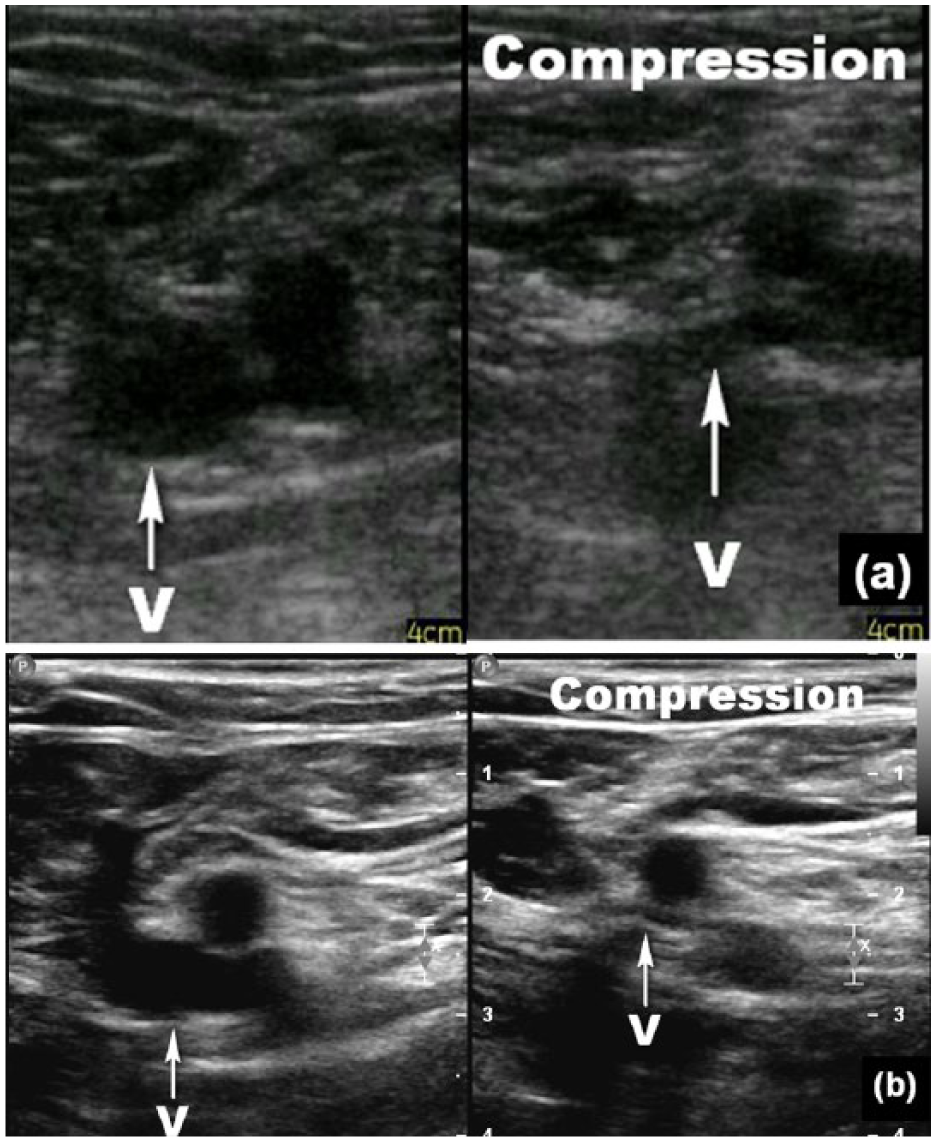
Transverse sonogram of a normal fully compressible common femoral vein in a 57-year-old woman with bilateral lower limb swelling produced by the pocket-sized ultrasound system (a) and the full-sized ultrasound system (b). The common femoral vein is denoted by “v.” The image on the left was produced with no compression, and the one on the right was taken with compression. Both ultrasound systems were able to depict the venous segment. However, the images produced by the pocket-sized system showed a higher level of background noise such that the venous lumen was filled with low-level echoes. In contrast, the venous lumen displayed by the full-sized system was free of internal echoes.
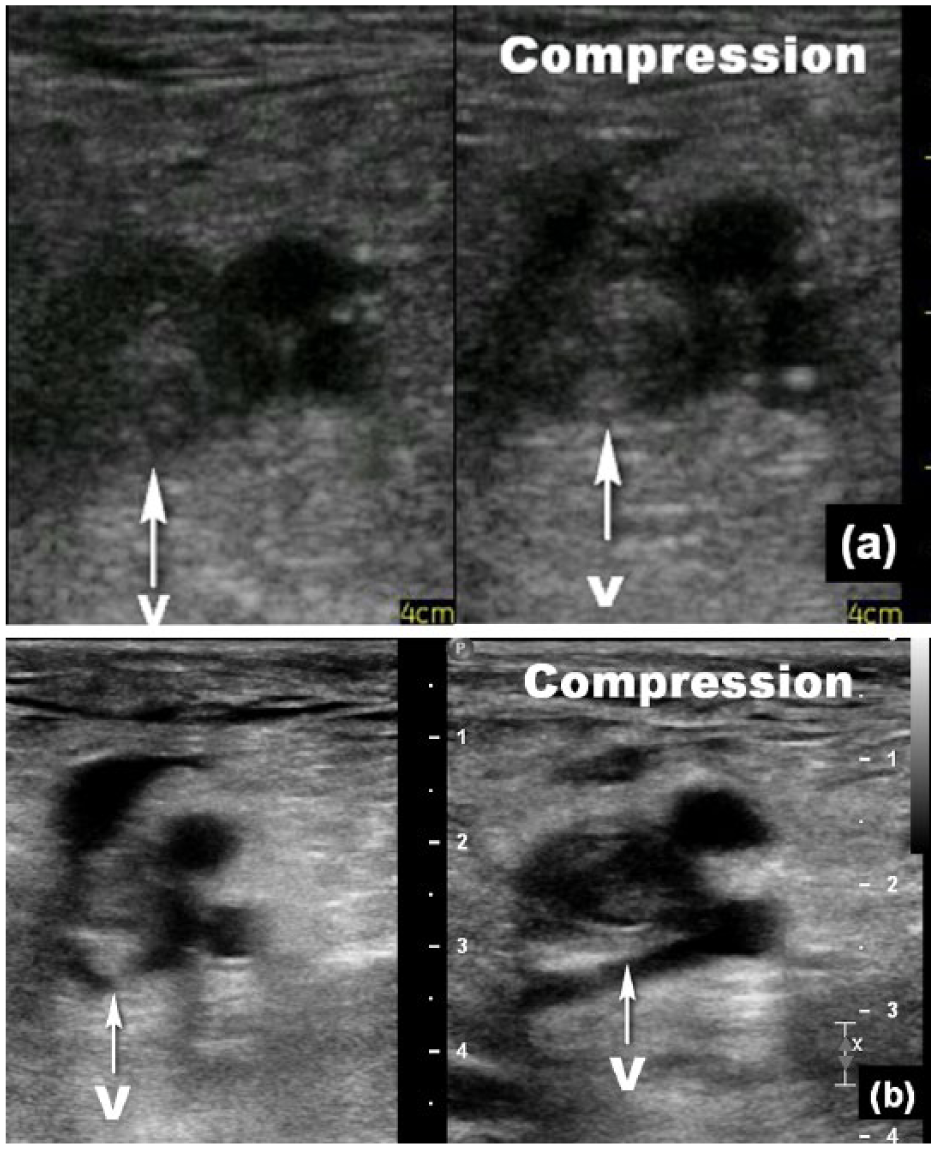
Transverse sonogram of a dilated incompressible common femoral vein in a 42-year-old woman with ovarian carcinoma produced by the pocket-sized ultrasound system (a) and the full-sized ultrasound system (b). The common femoral vein is denoted by “v.” The image on the left was produced with no compression, and the one on the right was taken with compression. Both systems were able to depict the veins, but the signal-to-noise ratio and detail resolution appeared lower in the images produced by the pocket-sized system compared to the full-sized system.
Figure 2 displays two dual images of a normal fully compressible common femoral vein produced from both systems. Both systems were able to depict the venous segment. However, the images produced by the pocket-sized system showed a higher level of background noise such that the venous lumen was filled with low-level echoes. In contrast, the venous lumen displayed by the full-sized system was free of internal echoes.
Figure 3 displays two dual images of a dilated incompressible common femoral vein filled with thrombus in a patient with ovarian carcinoma from the two ultrasound systems. Both systems were able to depict the veins, but the signal-to-noise ratio and detail resolution were lower in the images produced by the pocket-sized system compared to the full-sized system.
Discussion
Based on the results from this study, the performance of the pocket-sized ultrasound system in diagnosing proximal lower limb acute DVT is comparable to that of a full-sized ultrasound system. Both systems showed congruent results on positive and negative diagnoses for all the venous segments, with accuracy, sensitivity, and specificity all being 100%. Our results are similar to a recent study, which also reported a sensitivity of 100% and a specificity of 100% for detecting DVT in femoral veins and popliteal veins. 13 In comparison, this recent study found a lower sensitivity for detecting calf vein DVT using a pocket-sized system (sensitivity, 80%; specificity, 100%) and a lower feasibility for visualizing the calf veins (feasibility, 96%) compared to that for femoral veins (feasibility, 98%) and popliteal veins (feasibility, 100%). 13
Regarding the proportion of proximal lower limb venous segments that failed to be visualized, both systems showed the same result. Four venous segments (0.8% of all venous segments) could neither be depicted by both systems due to their deep-seated locations (average depth estimated to be more than 5 cm from skin) beyond the penetration power of the transducers. Penetration power is largely determined by transducer frequency: the lower the frequency, the higher the penetration power. 17 Therefore, the comparable penetration power of the two machines can be attributed to the comparable lowest frequencies offered by the two transducers, being 3.4 MHz for the pocket-sized system and 3 MHz for the full-sized system. Nevertheless, it should be noted that a lower frequency transducer such as a curvilinear array for abdominal imaging can be used to assess these deep-seated veins, although we did not include these lower frequency transducers for comparison in this study.
For image quality, although the images produced by the pocket-sized system had a lower signal-to-noise ratio and reduced resolution, the image quality was adequate for the investigation of proximal lower limb venous segments compared to the full-sized system. Pocket-sized ultrasound systems have been assessed elsewhere for applications in the field of echocardiography, abdominal imaging, and obstetric and gynecological imaging.8 –12 This study showed that the pocket-sized system has a promising role in the investigation of proximal lower limb acute DVT.
Nevertheless, we found some limitations of the pocket-sized system under study during our use. The images produced by this pocket-sized machine are in JPEG or MP4 format, which cannot be archived in the Picture Archiving and Communication System (PACS) for documentation and future reference, in contrast to the DICOM format produced by a full-sized system. Furthermore, the pocket-sized ultrasound system is charged by a battery that requires periodic recharge, and scanning is not allowed during recharging. In addition, as shown in the displayed images (Figures 2 and 3) in the results, the signal-to-noise ratio and detail resolution of the pocket-sized system appeared lower compared to the full-sized system, although the specifications on detail resolution of the pocket-sized system are not available from the vendor.
There are some limitations in this study. No X-ray venography was performed to determine the true accuracy, sensitivity, and specificity of the pocket-sized ultrasound system in the detection of the disease. The accuracy, sensitivity, and specificity derived from this study solely applied to the comparable detection rates of proximal lower limb DVT in our group of subjects between the two diagnostic ultrasound systems. In addition, we recruited our subjects in a single center using a convenience sampling strategy, which can be prone to selection biases. As a result, the external validity of this study may be limited, and generalization of the study results to the population may not be valid. Also, the operators were not blinded to the results of the full-sized system, but we endeavored to eliminate the biases by performing each examination with the pocket-sized system first before using the full-sized system. Furthermore, sonographic examinations are operator-dependent procedures, but all our investigators have more than 10 years’ experience in vascular sonography. This may minimize the effect of the operator’s technique on the results of the examinations. Moreover, since our examination protocol does not include the lower legs in the investigation of lower limb DVT, the calf veins were not studied in this research.
In conclusion, the pocket-sized ultrasound system demonstrated a comparable performance to a full-sized ultrasound system in this study, which found an overall sensitivity, specificity, and accuracy of the pocket-sized machine for the detection of proximal lower limb acute DVT being 100% (95% CI, 94.94%–100%), 100% (95% CI, 99.05%–100%), and 100% (95% CI, 99.19%–100%), respectively. The pocket-sized ultrasound system might serve as a readily available and valuable option for the investigation of proximal lower limb acute DVT, facilitating timely patient management, especially in the bedside and acute care settings.
Footnotes
Acknowledgements
We thank Ellen L. M. Yu, Research Officer, Clinical Research Centre, Princess Margaret Hospital, Hong Kong, for her statistical advice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.