
Abstract
We report the successful diagnostic and observational treatment of a renal arteriovenous malformation (RAVM) diagnosed with point-of-care color Doppler imaging. The patient presented with clinical symptoms suggestive of hydronephrosis. A physician-performed point-of-care sonography demonstrated gray-scale imaging that initially appeared to confirm renal pelvis dilatation. However, the addition of color Doppler revealed color blooming resembling a vascular turbulence within the kidney and the renal pelvis. A computed tomography angiogram was used to confirm the diagnosis of RAVM as the etiology of renal pelvic dilation. This case highlights the potential value of using color Doppler as a standard component for physicians who evaluate patients believed to have hydronephrosis.
Sonography has been proven to be a safe and cost-effective imaging modality for a variety of medical conditions. The increased portability of ultrasound equipment has led to the introduction of nonsonographers performing limited studies in a variety of clinical scenarios. Point-of-care sonography (POCS) has many advantages, including, but not limited to, more efficient diagnoses, focused treatment options, and, in some cases, eliminating additional, more expensive imaging studies.
POCS should be used by individuals formally trained to understand the instrumentation of the equipment. The specific equipment settings should include power output, concept of ALARA (As Low As Reasonably Achievable), equipment limitations, image optimization, recognition of 2D landmarks within the human body, and analysis of color Doppler signals. The physician conducting POCS in this case has been through the ultrasound accreditation process associated with the American Urological Association and the American Institute of Ultrasound in Medicine. 1
This case study illustrates how POCS was employed by a physician in conjunction with a thorough patient history and physical examination to detect an atypical urology problem.
Case Report
A 71-year-old Caucasian man with a medical history significant for recurrent nephrolithiasis presented as a new patient to his urologist with complaints of right-sided flank pain. Physician-performed POCS revealed hypoechoic regions in the superior and mid-portion of the right kidney, indicating possible hydronephrosis and thinning of the renal parenchyma (Figure 1A). A 14-mm nonobstructive calculus was also present in the lower pole of the right kidney.
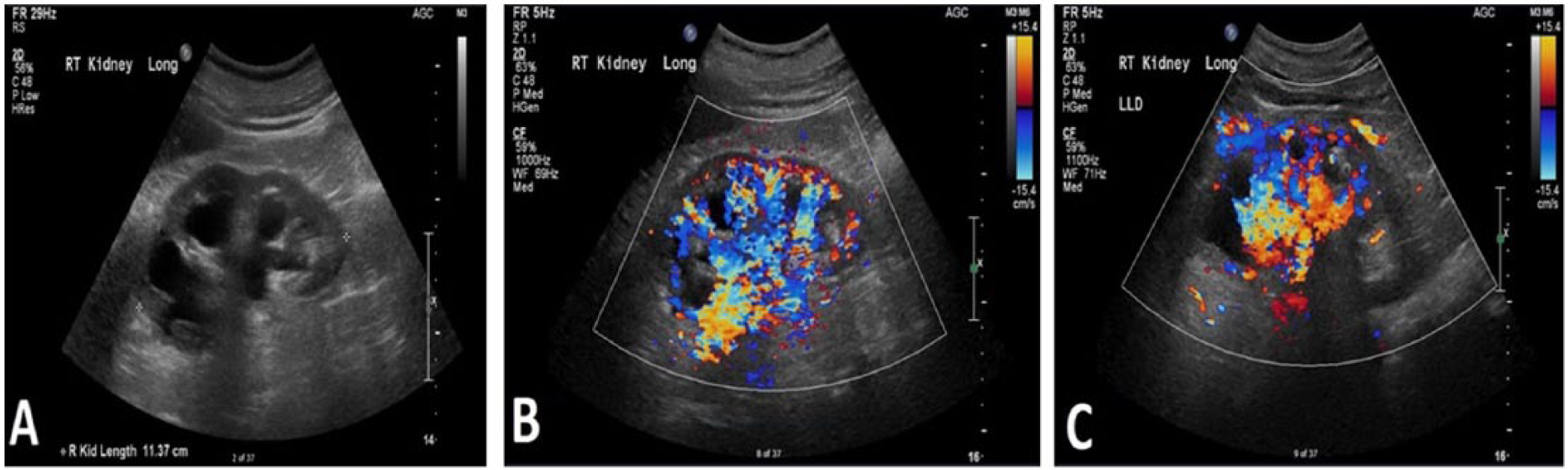
(A) Sonographic image showing hypoechogenic regions in the superior portion of the right kidney. (B, C) Color Doppler images showing prominent vascular abnormality in the superior portion of the right kidney suggestive of an arteriovenous fistula.
Color Doppler was then used to evaluate renal perfusion and interrogate the hypoechoic regions. Interrogation with color Doppler revealed high-volume vascular flow in the right renal pelvis (Figure 1B, C), suggesting a prominent vascular abnormality. The etiology of the hypoechoic regions was preliminarily diagnosed as a renal arteriovenous malformation (RAVM), and a computed tomography angiogram (CTA) was ordered for confirmation.
The arterial phase acquisition of the CTA (Figure 2) revealed abnormal vasculature with dilatation of the right renal artery and vein, including early venous opacification, and confirmed the presence of an arteriovenous fistula. The CTA also revealed cortical thinning, particularly at the upper pole of the right kidney, and a tiny 2-mm stone in the upper third of the right ureter. Images from the 3D construction of the CTA showed the dilation of multiple serpiginous renal vessels (Figure 3). Based on the patient’s current health status, conservative observational treatment was elected.
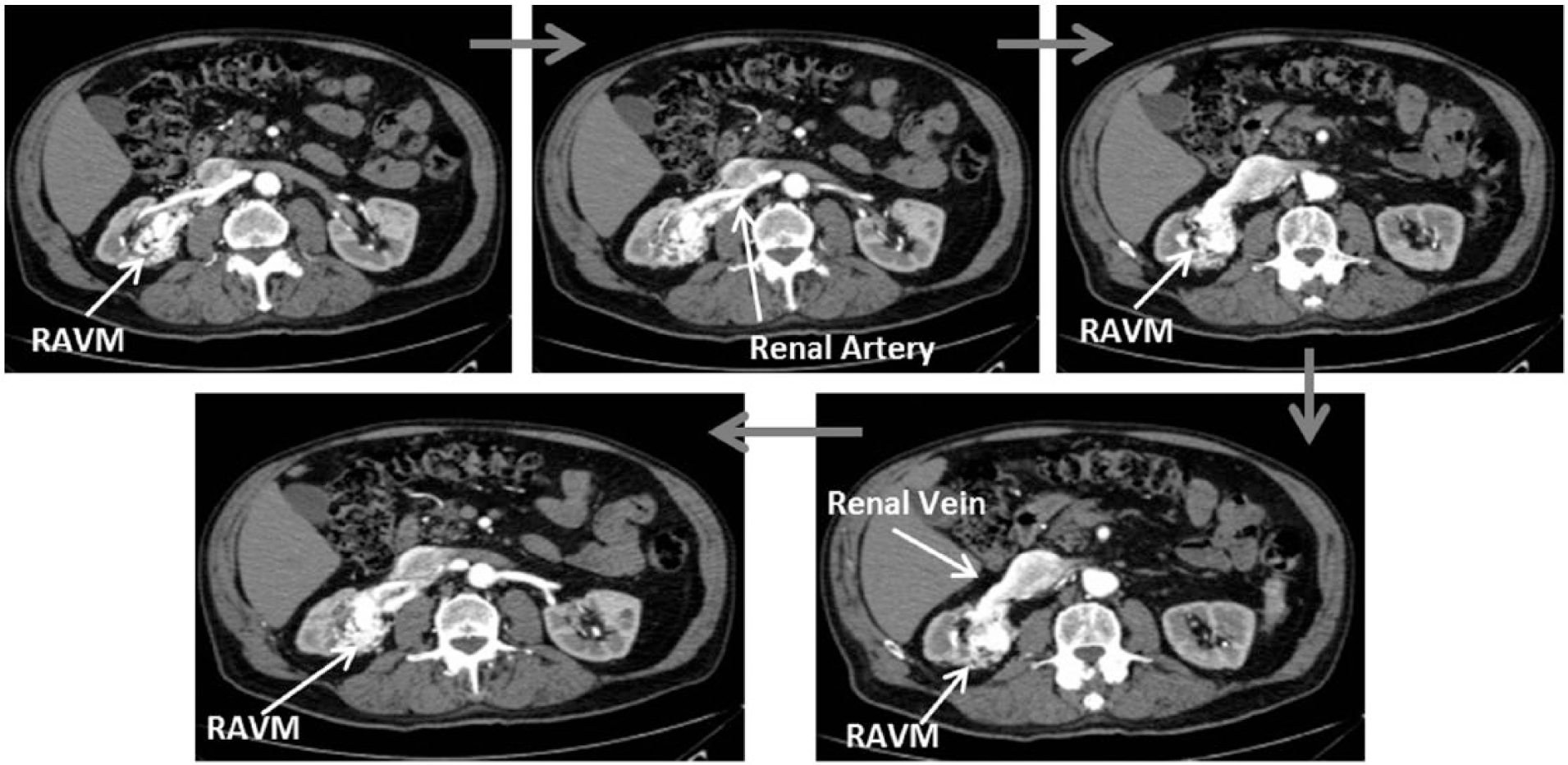
Time-sensitive computed tomography angiogram of the abdomen and pelvis showing simultaneous flow in the right renal artery and vein depicting the fistulae between the artery and the vein.
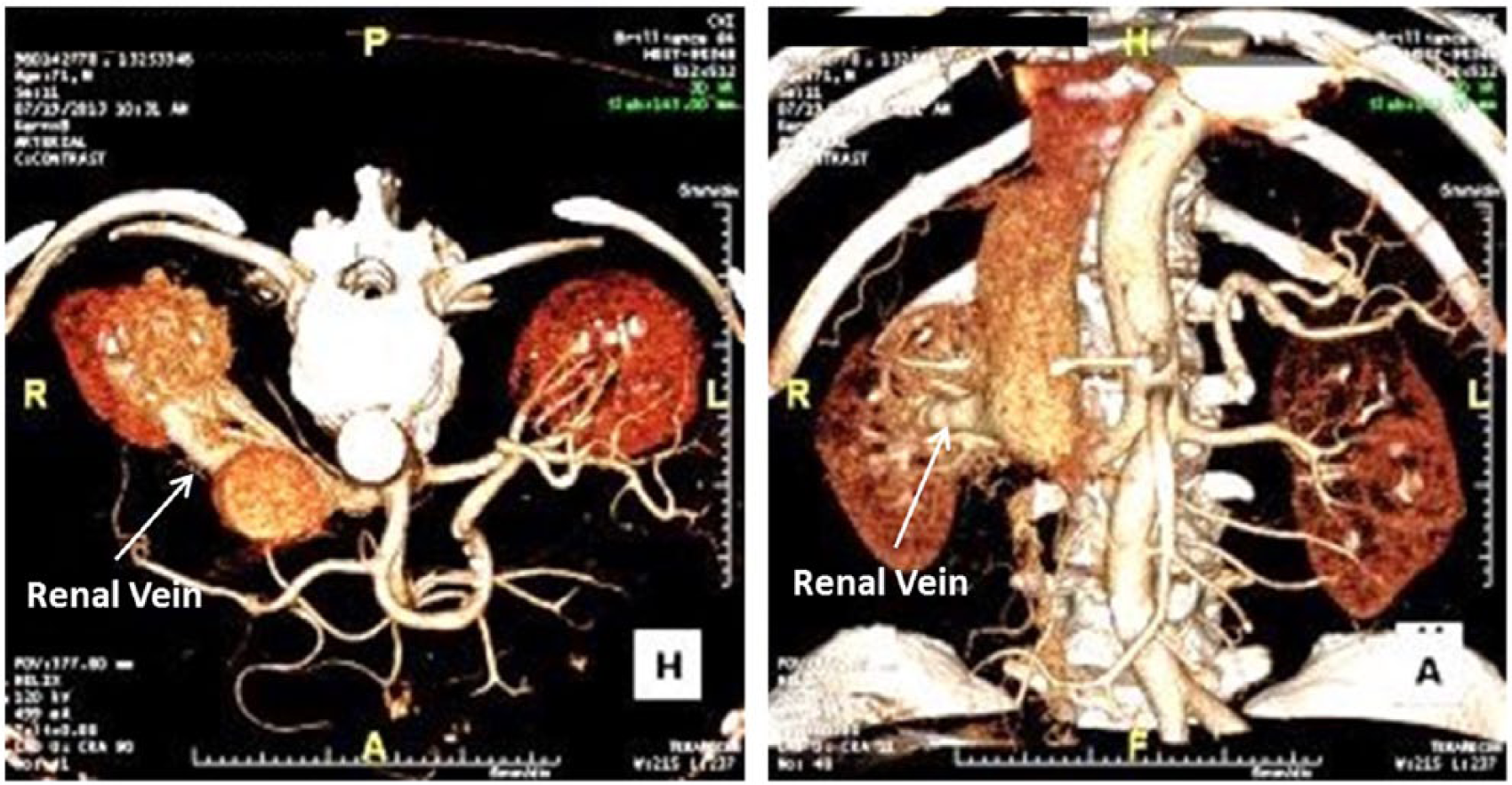
Three-dimensional computed tomography angiogram of right renal arteriovenous malformation. There is noticeable dilation of the renal veins.
A follow-up visit at 14 months confirmed that the patient was doing well. The ureteral and renal calculi were treated medically with potassium citrate and have since resolved. The patient’s right-sided flank pain also resolved. The patient’s pain resolved after medical dissolution of his uric acid calculus, as there was no treatment of the RAVM. He continues to be monitored annually for possible changes within the malformation, and formation of new calculi.
Discussion
Although not uncommon after a renal biposy, RAVMs are rare when compared with hydronephrosis. The major diagnostic challenge physicians face in identifying RAVMs with POCS is distinguishing the dilated hypoechoic renal collecting system caused by obstruction versus the hypoechoic vascular structures found in RAVMs.2,3 RAVMs are deceptive in that, like obstructive hydronephrosis, they may present with gross hematuria. Since hematuria can be a symptom of several other conditions, including bladder cancer and ureteral calculi, further imaging is often required to determine the etiology of the symptom.4,5 Naganuma et al. 4 described five cases of RAVMs, with four of the five patients complaining of hematuria. In all five cases, color Doppler was used to visualize the RAVM. 4
In the case presented, the POCS showed hypoechoic structures that can be confused with the appearance of hydronephrosis. However, the addition of color Doppler revealed vascular flow within the hypoechoic regions consistent with an RAVM rather than hydronephrosis. The RAVM was then confirmed using CTA, which showed simultaneous flow between the right renal artery and vein. This case is similar to several other case reports in which color Doppler was used to differentiate hydronephrosis from an RAVM.3,6–9
The etiology of this particular RAVM is thought to have been traumatically induced when the patient suffered a motor vehicle collision as a child. Less than 1% of RAVMs are congenital. Most are acquired secondary to surgery, cancer, or trauma.3,10–12
Treatment options for RAVMs include surveilling the abnormality for changes or presentation of symptoms, ligation of the fistula, coil embolization, or, in severe cases, total or partial nephrectomy.5,9 Unless the patient with an RAVM has severe symptoms, such as hypertension or congestive heart failure, surgical treatment is rarely required. 6 Congestive heart failure rarely presents in RAVM and is more common in patients suffering from congenital fistulas of the kidney. 7 In this particular case, surgery was deemed unnecessary as the patient did not present with hypertension or severe pain. Increased awareness among physicians who use POCS is vital given that an RAVM may mimic hydronephrosis or cystic lesions. The lack of an accurate diagnosis, potiential interventional procedures, or surgery could be extremely detremental to the patient.
Conclusion
While threatening complications exist, most RAVMs are detected incidentally and only require careful follow-up. Accurate diagnosis, however, is paramount to selecting an appropriate therapeutic course. In this case, the physician sonographer used his postgraduate training to recognize that there were other etiologies that might explain this hypoechoic appearance within the kidney. It was the addition of color Doppler that identified the hypervascular region and led to the diagnosis of RAVM. POCS performed by a properly trained physician in the use of sonography can improve patient access without compromising diagnostic accuracy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.