
Abstract
Purpose:
This was a feasibility study of shear wave ultrasound elastography for characterization of liver tumors and to compare the tissue elasticity values of hepatocellular carcinoma (HCC), liver metastases, and normal liver tissues.
Methods:
Forty-one patients and 30 healthy volunteers were recruited and categorized into HCC, liver metastasis, and control groups based on their computed tomography and sonographic examinations. Elasticity values of different groups were compared statistically.
Results:
Mean (standard deviation) elasticity values for HCC, liver metastasis, and normal liver tissue were 51.45 (14.96), 49.89 (13.82), and 6.63 (1.65) kilopascal, respectively. Statistically significant differences were found between the elasticity values of HCC and liver metastasis with normal liver tissue. Based on the receiver operating characteristics analysis, 18.25 kilopascal may differentiate the malignant focal liver lesions from the normal liver tissue with both sensitivity and specificity of 100%.
Conclusion:
Shear wave ultrasound elastography may be able to differentiate HCC and liver metastasis from normal liver tissue based on the tissue elasticity values.
Palpation is one of the oldest clinical examination methods used for the evaluation and detection of tumors or masses. 1 The principle of palpation lies in the fact that tumors are usually harder or stiffer than the surrounding tissues. Pathologic conditions such as neoplasm or inflammation are known to alter the tissue elasticity. 2 However, manual palpation is a skill-dependent method and is limited to detecting larger structures or abnormal masses where the tissue stiffness is considerably different from the surrounding tissues. Furthermore, interpretation of the palpation is subjective and does not provide any quantified data. 3
Ultrasound elasticity imaging has been regarded as an extension of the ancient art of palpation. 1 Over the past 2 decades, ultrasound elasticity imaging (commonly known as elastography) has emerged as a valuable tool to visualize and quantify soft tissue stiffness and viscoelastic properties. The principle of elastography is based on the premise that tissue elasticity is altered in the abnormal tissue. 2 For instance, malignant tumor tissue is usually stiffer compared to the surrounding normal tissues.4,5 During elastography, an excitation force is applied. The tissue’s response to the excitation force is measured and used to infer the mechanical properties of the tissue. Generally, excitation force can be applied externally by static compression or internally using ultrasound radiation force.3,6
Real-time shear wave ultrasound elastography (SWE), introduced by SuperSonic Imagine, is a novel technology involving remote generation of transient mechanical forces into the tissues by an ultrasonic transducer. The resulting shear waves are imaged with the same transducer at an ultra-fast imaging sequence (up to 20 000 frames per second) in order to provide a quantitative elasticity map. 7 Integration of SWE with the ultrasound system provides real-time images for the identification of the area of interest. SWE has been well established for the assessment of breast, 8 thyroid, 9 prostate, testicles, and musculoskeletal system. 10
Several studies have used SWE for the assessment of diffuse liver disease11,12 and focal liver lesions. 13 However, data on SWE assessment of focal liver lesions, especially hepatocellular carcinoma (HCC) and metastatic lesions, are still limited. Therefore, this study was conducted to assess the elasticity values of the malignant focal liver lesions, that is, HCC and metastatic liver lesions using SWE. In particular, the aims of the study were to compare the elasticity values between HCC, liver metastases, and normal liver tissues, as well as to evaluate the potential of SWE in the characterization of these tissues.
Methods
Patient and Control Groups
This study was approved by the Institutional Medical Ethics Committee (Protocol No. MEC 937.13). Liver cancer patients who had undergone multiphasic liver computed tomography (CT) examination were recruited. The inclusion and exclusion criteria are given in Table 1. Following diagnostic CT examination, patients were sent for SWE examination for the measurement of lesion elasticity. In addition, healthy volunteers older than 20 years with normal liver sonographic results and without any history of liver disease or liver intervention were recruited as the control group. The control group provided reference elasticity values for normal liver tissue that were used as a comparison for the elasticity values of HCC and liver metastasis. All patients and volunteers were counseled about the procedure of the SWE examination and written informed consent was obtained from all patients and volunteers prior to the examination.
Inclusion and Exclusion Criteria for Patient Recruitment.
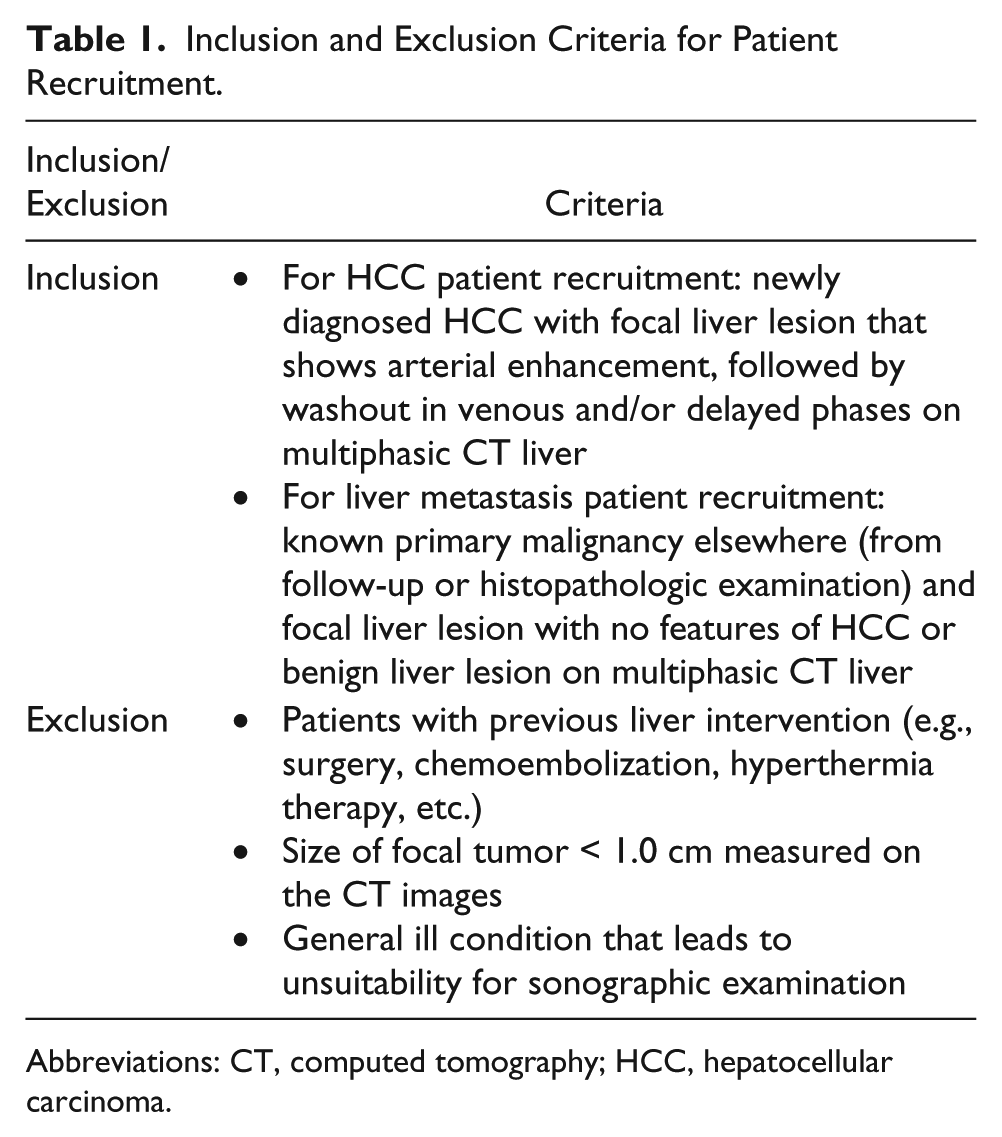
Abbreviations: CT, computed tomography; HCC, hepatocellular carcinoma.
Study Design
All patients were required to fast for at least 6 hours prior to the CT and SWE examination to avoid any possibility that may affect liver stiffness. The sonogram and SWE imaging were performed by a trained radiologist who was blinded to patients’ diagnosis to avoid bias. During the sonographic and SWE measurements, the right lobe of the liver was examined in the left lateral decubitus position, with the right arm in maximum abduction. Scanning was performed with intercostal approach with minimal pressure applied on the skin. The dedicated sonogram of the liver was performed during breath-hold to minimize motion artifact. The age, gender, weight, and body mass index (BMI) were recorded for all patients and volunteers, whereas the serum alanine transaminase (ALT) level was collected from only the HCC and liver metastasis patients. The serum ALT level was measured as enzyme unit per liter where the normal serum ALT level is within the range of 30 to 65 units per liter.
CT and SWE Imaging Protocols
Dynamic multiphase CT was performed on the liver cancer patients to differentiate HCC from liver metastasis using a 128-slice CT scanner (Somatom Definition AS; Siemens AG, Erlangen, Germany). All patients fasted for at least 6 hours prior to the CT examination. Following non-contrast enhanced scan (Phase 1), 100 mL iodinated contrast agent, Ultravist 300 (Bayer Schering Pharma, Berlin, Germany), was injected at a rate of 5 mL per second. The early arterial phase (Phase 2) was triggered when the threshold enhancement of 100 Hounsfield units (HU) was detected using a bolus tracking method. The late arterial phase (Phase 3) was started immediately following the early arterial phase scan in the caudocephalic direction. The portal venous (Phase 4) and delayed scan (Phase 5) started at a fixed delay of 60 seconds and 90 seconds, respectively, from the beginning of contrast injection. Patients were instructed to hold their breath in full inspiration during each scan.
After CT examination, patients were sent for SWE imaging. Prior to the elasticity measurement, real-time sonography was performed using a shear wave ultrasound system and an SC6-1 convex probe (Aixplorer; SuperSonic Imagine, Aix-en-Provence, France) to identify the lesion(s). During SWE measurements, a standardized 5-mm-diameter circular region of interest (ROI) or “Q-Box” was placed within the focal liver lesions. The placement of the Q-Box should avoid the portal vein in order to reduce the incidence of reverberation artifacts and increased subcapsular stiffness. Elasticity values (in kilopascal [kPa]) and 2D maps were obtained using the dedicated software of the ultrasound system. Lesion size (maximum diameter measured on conventional sonography), depth of lesion, and elasticity values along with its minimum and maximum ranges were recorded. Stiffness pattern of the lesion (homogeneous or heterogeneous) was also determined based on the standard deviation (SD) value within the ROI. A homogeneous lesion was defined as a lesion with an SD within the ROI of less than 5 kPa, whereas a heterogeneous lesion has a value higher than 5 kPa.
Statistical Analysis
All statistical analysis was performed using Statistical Package for the Social Sciences (SPSS version 23.0; IBM Corporation, Armonk, NY). The elasticity values among HCC, liver metastasis, and control groups were compared using Mann-Whitney U tests. The correlations between the lesion heterogeneity of HCC and liver metastasis groups were analyzed using Fisher exact test, whereas the correlations between elasticity value, lesion size, BMI, and ALT level of HCC and liver metastasis groups were made using Spearman rho correlation test. In addition, the BMIs of different groups were compared using Kruskal-Wallis test. A confidence interval of 95% was used in all the statistical tests and P value < .05 was considered as statistically significantly different. Furthermore, receiver operating characteristics (ROC) analysis was carried out to determine the elasticity cut-off value for malignant focal liver lesions (including both HCC and liver metastasis) from the normal liver. Sensitivity and specificity for the cut-off value were reported.
Results
Patient Population
A total of 41 patients (28 male, 13 female) with an average (SD) age of 60 (12) years were enrolled in the study. The SWE examination was successfully performed on 25 patients, whereas 16 patients did not complete the examination due to inability to hold their breath adequately (n = 4) or lesion-related factors such as lesion was too near to the portal vein (n = 3); was too deep in location, that is, more than 6 cm (n = 1); and appeared isoechoic on the sonogram (n = 8). The patients who completed the SWE examination were categorized into two groups: HCC group (n = 16 with 18 lesions examined) and liver metastasis group (n = 9 with 10 lesions examined) based on the CT diagnosis results. A control group of 30 volunteers (12 male, 18 female) with an average (SD) age of 54 (11) years was recruited. The demographic and diagnostic information of the patients and volunteers is given in Supplementary Table 1.
Liver Elasticity Measurement
The SWE examinations were performed on 18 HCC and 10 metastatic lesions. Examples of SWE and sonographic images of HCC, a metastatic lesion, and normal liver tissues (control group) are shown in Figure 1. The mean (SD) size of the HCC lesions examined was 8.4 (4.7) cm in diameter and 4.3 (1.7) cm in depth. In comparison, the mean (SD) diameter and depth for the metastatic lesions were 4.5 (2.2) cm and 3.6 (1.5) cm, respectively. No significant correlation was found between the lesion’s sizes and the associated elasticity values in HCC (r = 0.449, P = .06) and liver metastasis (r = 0.176, P = .627) groups.
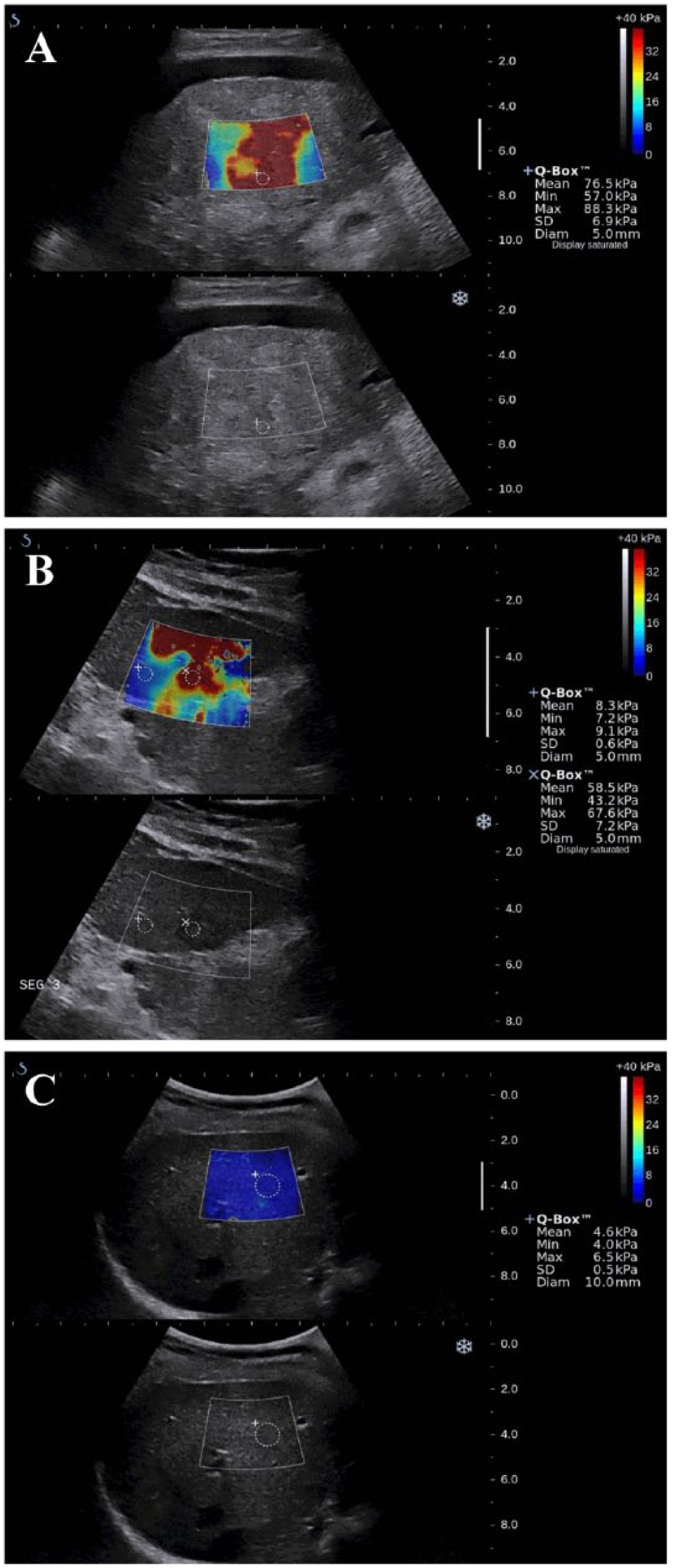
Shear wave ultrasound elastography and B-mode sonograms of (A) hepatocellular carcinoma, (B) liver metastasis, and (C) normal liver (control group). For each image, an elasticity map (top panel) is displayed for the area corresponding to the region of interest in the B-mode image (bottom panel). Another smaller region of interest called the “Q-Box” with an arbitrary size can be set to calculate the average value of the stiffness within the area. The color scale and calculated elasticity values (kPa) are displayed on the right panel of each image.
The mean elasticity values of the lesions for HCC, liver metastasis, and control groups are summarized in Table 2. The elasticity values of the HCC were statistically significantly (P = .001) higher than the elasticity values obtained from the control group. A similar observation was found for the liver metastasis group, where the elasticity values of the liver metastasis lesions were statistically significantly higher (P = .001) than the elasticity values of the control group. However, no statistically significant difference (P = .811) was found for the elasticity values between the HCC and liver metastasis groups. A box plot showing the distribution of the elasticity values of HCC, liver metastasis, and control groups is shown in Figure 2.
Mean Elasticity Values and Statistical Test Results for Different Patient Groups.
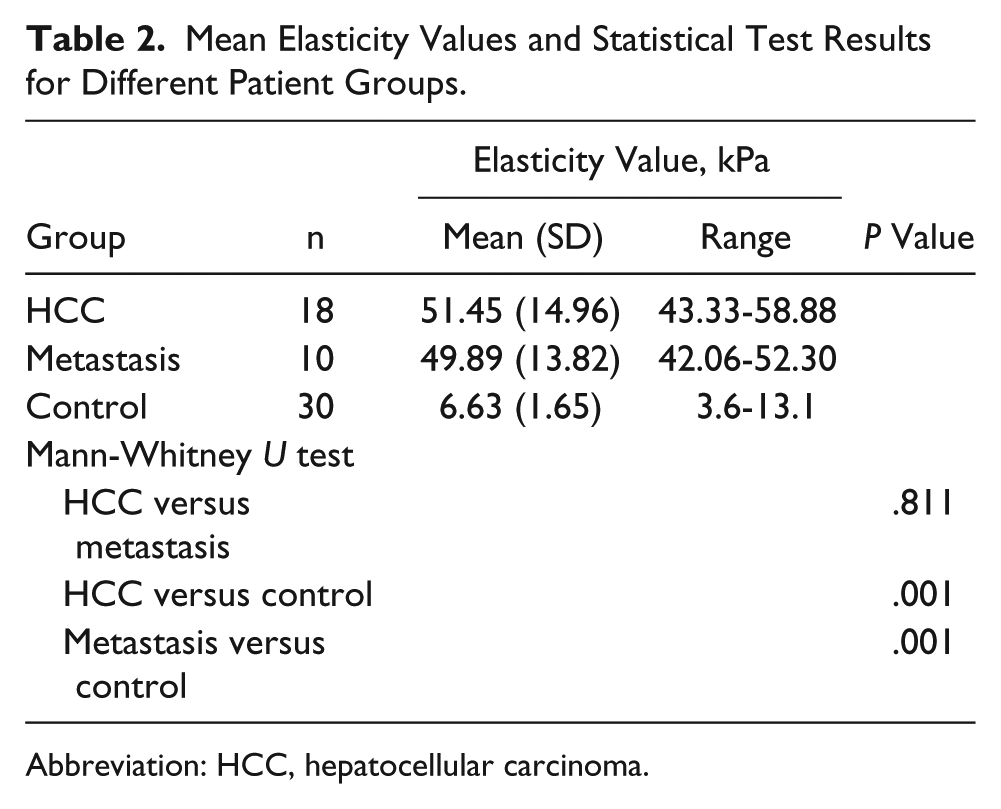
Abbreviation: HCC, hepatocellular carcinoma.
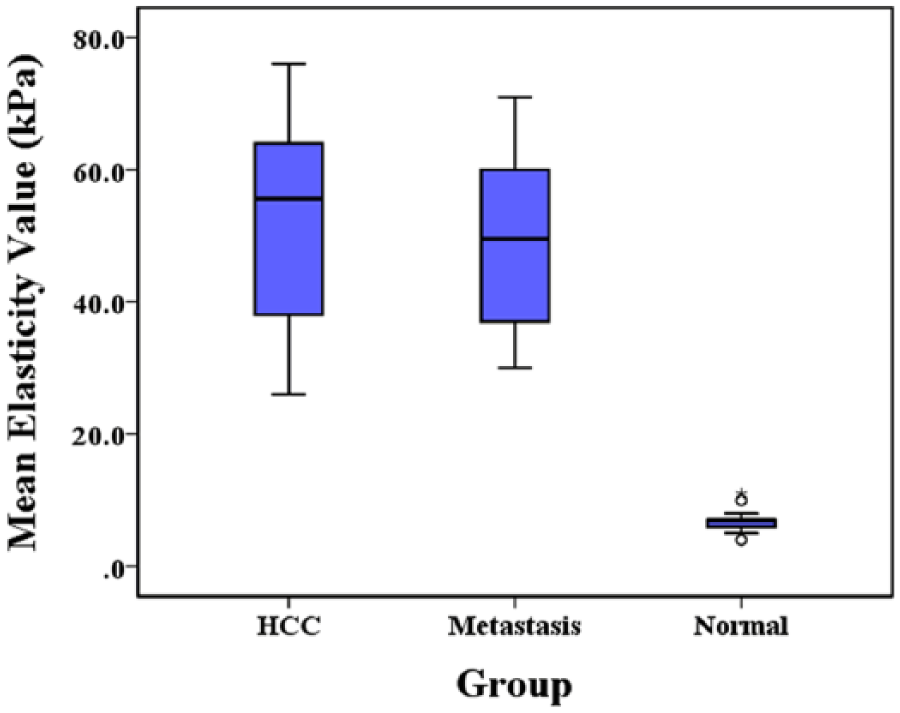
Box plot showing the elasticity values of hepatocellular carcinoma (HCC), liver metastasis, and normal liver (control) groups.
The distribution of the stiffness patterns of all lesions examined is presented in Table 3. About 28% (n = 5) of the HCC lesions and 40% (n = 4) of the metastatic lesions were found to be heterogeneous. No statistically significant difference (P = .677) was observed for the lesion stiffness patterns between HCC and liver metastasis groups.
Distribution of Stiffness Patterns in Hepatocellular Carcinoma (HCC) and Liver Metastasis Groups.
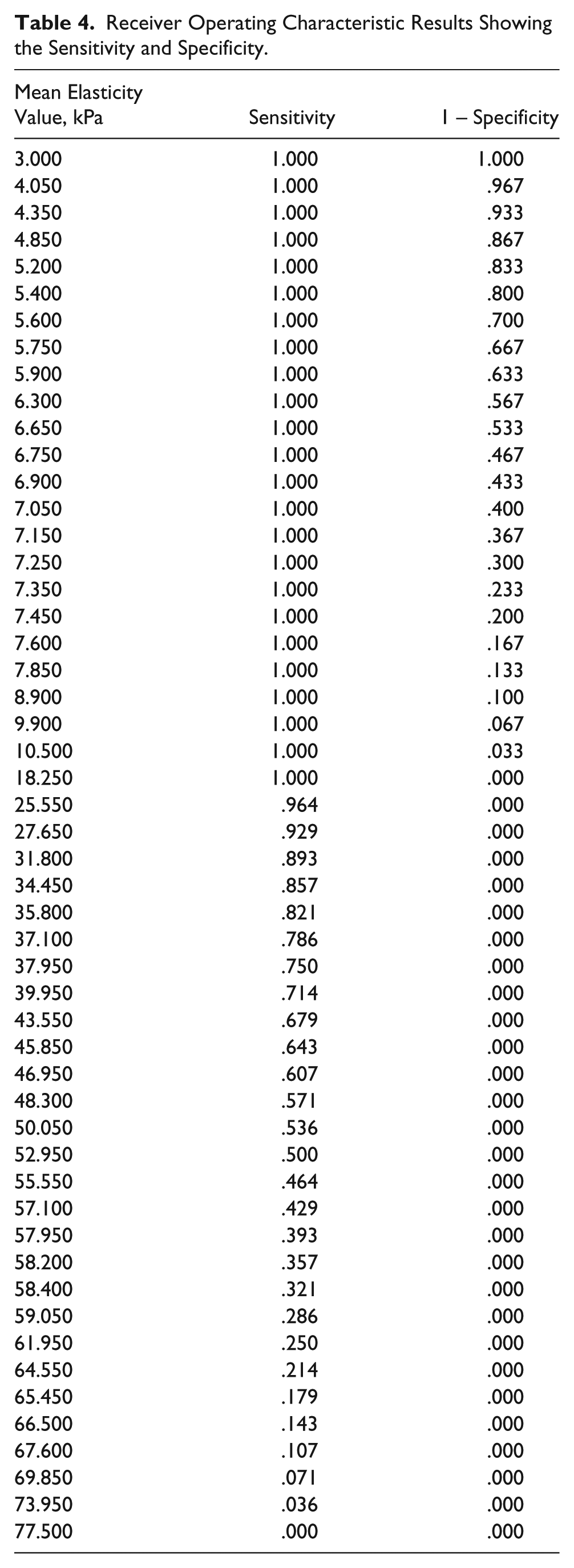
From the ROC analysis, a cut-off value of 18.25 kPa was obtained to differentiate between malignant focal liver lesions (HCC and liver metastases) and normal liver tissues, with both sensitivity and specificity achieved at 100% (see Table 4). Since the elasticity values of HCC and metastatic lesions were not statistically significantly different, ROC analysis was not performed to determine the elasticity cut-off value between HCC and metastatic lesions.
Receiver Operating Characteristic Results Showing the Sensitivity and Specificity.
Correlation Between Elasticity Values With BMI and Serum ALT Level
The mean BMI and serum ALT levels of HCC, liver metastasis, and control groups are shown in Table 5. The BMIs of HCC, liver metastasis, and control groups were not statistically significantly different (P = .069) from each other. From the Spearman rho correlation analysis, a weak negative correlation (r = −0.235, P = .349) was observed between BMI and elasticity values of the HCC group, whereas a weak correlation (r = 0.389, P = .266) was observed for the liver metastasis group. A weak correlation (r = 0.378, P = .039) was also found between the BMI and elasticity values in the control group. However, only the correlation observed in the control group was considered significant. The ALT level of the HCC group was significantly (P = .026) higher than the ALT level obtained from the liver metastasis group. Weak or no correlation was found between the ALT levels and elasticity values of the HCC (r = 0.055, P = .829) and liver metastasis (r = 0.438, P = .206) groups.
Mean (Standard Deviation) Body Mass Index (BMI) and Serum Alanine Transaminase (ALT) Levels in Different Patient Groups.

Abbreviation: HCC, hepatocellular carcinoma.
Discussion
Sonography is the most widely used modality for HCC screening as it is relatively low cost and widely available. 14 Detection and characterization of focal liver lesions are critical for screening patients with chronic liver disease. Data on elasticity values of focal liver lesions are limited as previous elasticity studies used different types of elasticity imaging modalities. This study provided a potential understanding of the role of SWE in characterizing HCC, liver metastases, and normal liver tissue in terms of tissue elasticity.
Although the lesion size varied between the HCC and liver metastases patients, there was no significant relationship observed between the elasticity value and lesion size. This was in accordance with earlier studies13,15 suggesting that there was no statistical correlation observed between the lesion’s size and stiffness value.13,15 The mean (SD) elasticity value for normal liver tissue obtained from this study (6.6 [1.7] kPa) was in close agreement with the elasticity value of normal liver parenchymal at 7.7 kPa, reported earlier. 11 In addition, the elasticity values of the HCC and liver metastatic lesions obtained from this study (51.45 [14.96] and 49.89 [13.82] kPa, respectively) were also similar to the values reported by Park et al. 15 (45.7 [35.7] and 67.4 [43.4] kPa, respectively). However, these values were found to be relatively higher than the values reported by Guibal et al. 13 (14.9 [10.0] and 28.8 [16.0] kPa, respectively). The heterogeneous appearance of the liver lesions may explain the disagreement as higher lesion heterogeneity (39% of HCC and 86% of metastases) was observed in the Guibal et al. 13 study. Besides, the small sample size in this study (18 HCC and 10 metastatic lesions) compared to the Guibal et al. study (16 HCC and 43 metastatic lesions) might also contribute to the disagreement above.
In accordance with the earlier reports,16,17 the elasticity values of HCC and metastatic lesions were significantly higher than the elasticity values of the normal liver tissue. However, the elasticity values of HCC were found to be essentially similar to the value of metastatic lesions, matching closely with the findings published earlier.13,15 In view of the above, the elasticity value might be useful to differentiate the focal liver lesions from the normal liver tissue; however, it might not be useful to differentiate HCC from metastatic lesions. Using ROC analysis, a diagnostic cut-off value of 18.25 kPa could be used to differentiate malignant focal liver lesions from normal liver tissue, with both sensitivity and specificity achieved at 100% in this study. However, a larger sample size and multicenter study are needed to verify this finding.
The elasticity value is known to be affected by two factors: obesity (high BMI) and active liver inflammation.18–23 Obesity is a common limitation of all ultrasound-based elastography methods, as reported by various studies.18–20 The patient’s high BMI is often associated with the inability to obtain reliable liver stiffness measurements using SWE.24,25 The negative effect of obesity on the SWE measurement relates to the limited depth of shear wave penetration. The effective depth for SWE measurement is up to 8 cm from the transducer, according to the manufacturer’s specification (Aixplorer; SuperSonic Imagine). However, Wang et al. 26 reported that a higher success rate and accuracy were achieved at a 3- to 5-cm penetration depth, although the effective depth as claimed by the manufacturer is up to 8 cm. In addition, the presence of a thicker layer of subcutaneous fat surrounding the liver might reduce the accuracy of the elasticity measurement. Different acoustic characteristics and tissue composition of the fat from the liver parenchyma as well as the presence of several interfaces in the fatty tissue could have altered the shear wave’s pattern and thus affected the accuracy of the measurements. 27
Furthermore, active liver inflammation has been reported to increase liver stiffness value.21–23 Hepatic necroinflammation could lead to an accumulation of extracellular matrix protein, thus altering the hepatic architecture by forming hepatic fibrosis with abnormal collagen deposition. 28 These changes in the hepatic architecture could have induced a higher value of liver stiffness, leading to false-positive results. 29 Serum ALT level has served as a hepatic inflammatory marker that could be used to monitor liver inflammation. A higher ALT level in serum could reflect more severe hepatic necroinflammation. 23 It is surprising that there was no significant correlation observed between the elasticity values and ALT levels or the BMI of the patients. The small sample size of this study might be responsible for the above observation.
There were several limitations found within this study. First, the patient population in each group (HCC, liver metastasis, and control groups) was relatively small and not standardized and, hence, might affect the power of the statistical tests. Since the SWE measurement could not be performed on some patients due to lesion-related factors or patients could not hold their breath adequately, the patient selection bias became a limitation in this study and might have affected the statistical analysis results. Next, the histologic proofs of the patients diagnosed with liver metastases were not obtained from pathologic specimen analysis, as this would require an invasive biopsy procedure. Although the heterogeneity nature of the lesion might affect the overall stiffness value, the lesions with heterogeneous appearance were still included in this study. Despite hepatic inflammation and obesity (as reflected by the serum ALT level and BMI), elasticity measurement using SWE might also be affected by other hepatic diseases such as cholestasis, hepatic congestion, steatosis, infiltrative diseases, and benign tumors.30,31 However, these factors were not evaluated in this study. Further study will be needed to investigate the influence of these parameters on the accuracy of SWE measurement.
Conclusion
SWE is a noninvasive, quantitative, and nonradiating method that provides additional information to characterize HCC and metastatic liver lesions based on the tissue elasticity. A statistically significant difference (P < .05) was found between the elasticity values of the HCC or metastasis group and the control group; however, no statistically significant difference (P > .05) was found between the HCC and metastasis groups. A cut-off value of 18.25 kPa is suggested to differentiate between focal liver lesions and normal liver tissue, whereby elasticity values above 18.25 kPa were considered as a malignant tumor (either HCC or liver metastasis). Although a preliminary conclusion has been reached, further research with a larger cohort is required to confirm the findings and to assess the diagnostic role of SWE in malignant and benign focal liver lesions assessment.
Footnotes
Acknowledgements
The authors would like to thank the sonographers (Sook Sam Leong and Johanna Wong) and the medical officer, Dr Fui Ting Pang, for their technical support in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Postgraduate Research Grant (P0017-2012B) sanctioned by the University of Malaya, Kuala Lumpur, Malaysia.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.