
Abstract
Recently, there have been significant advancements in sonography in diagnosing cervical insufficiency and monitoring the effect of cerclage therapy. 1 These advantages have been driven by the increasing use of transvaginal sonography and the incidental diagnosis of a short cervix, which has been used as an indication for cerclage placement.2–5 There are few data regarding the prediction of preterm versus term delivery after cerclage placement, despite studies demonstrating that transvaginal sonography is a precise method of serial evaluation of the cervix after cervical cerclage placement.4–8 In cases of cervical insufficiency, there is a significant correlation of progressive cervical change, often as much as 5 mm per week, measured by transvaginal sonography and the likelihood of preterm birth. 3 Hedriana et al. 8 performed serial sonographic assessment of cervical lengths after cerclage. This study has two significant findings. First, there was a striking increase in overall cervical length after the McDonald procedure. This is similar to the increase in cervical length after cerclage described by other studies.5–7 Second, it has been found that the length of the cervix left above the cerclage at 24 to 28 weeks was the best predictor of preterm delivery. 8
The study addressed another poorly understood issue of the outcomes of a cerclage procedure—the significance of the location of the stitch within the cervix.
Materials and Methods
The authors conducted a retrospective cohort study analyzing gestational ages at delivery in 72 consecutive patients who underwent placement of a cervical cerclage between June 2010 and January 2015. Patients’ ages varied from 21 to 37 years, with a median of 26 years.
The following inclusion criteria were used: (1) singleton gestation; (2) history-based cerclage due to cervical insufficiency (which includes two or more consecutive prior second trimester pregnancy losses, with painless cervical dilation, in which other causes of pregnancy loss or preterm birth have been excluded); and (3) patients who elected to have a cerclage based on obstetric history, followed by serial sonography in the authors’ facility. Patients with emergency cerclage placement for prolapsed fetal membranes, fetal anomalies, and presence of maternal medical conditions at risk for preterm delivery were excluded from the study. The study met exemption conditions for institutional review board approval because the collection of data is derived from existing records. All patients had a formal maternal-fetal medicine consultation. Risks and benefits of cerclage were discussed and the options for elective cerclage placement or serial transvaginal sonography were offered to the patients. Elective cerclage was placed between 11 and 15 weeks’ gestation after an ultrasound examination for fetal viability, fetal anatomy, and cervical length.
All the procedures were McDonald cerclage using 5 mm Mersilene tape (Ethicon, Somerville, NJ). Patients were placed in lithotomy position. The cervix was grasped at 6 o’clock with a ring forceps, and traction was applied caudally to expose a posterior fornix. Then, a purse- string suture was inserted with bites of the needle deep enough to suture it to the cervical stroma. Four to 6 bites of the needle were required to encircle the cervix, depending on its thickness. All patients were seen one week after cerclage placement by sonographers to assess the integrity of the cerclage. The cervical length was evaluated using transvaginal sonography with Voluson 730 Expert (GE Healthcare Inc., Milwaukee, WI). Cervical length was measured on the sagittal view from the internal to external os, divided by 3. The upper third of the cervix was defined as a portion from the internal os to one third of the total length of the cervical canal (Figure 1). The lower third was defined as a portion from the external os to the total length of the cervical canal (Figure 2); the mid-portion was in between (Figure 3). All sonographers were certified as completing a cervical length education and review (CLEAR) program. The location of the stitch was determined during real-time scanning by a sonographer and confirmed retrospectively by a maternal-fetal medicine specialist. All patients were managed as recommended by the American College of Obstetricians and Gynecologists by using progesterone supplementation and pelvic rest.
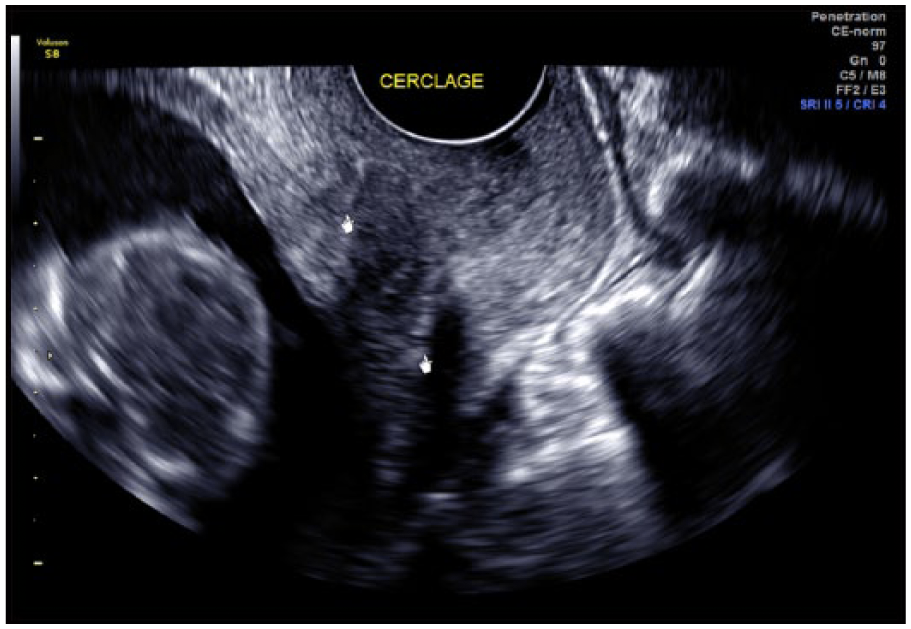
Cerclage suture is located in the upper third of the cervix.

Cerclage suture is identified in the lower third of the uterine cervix.
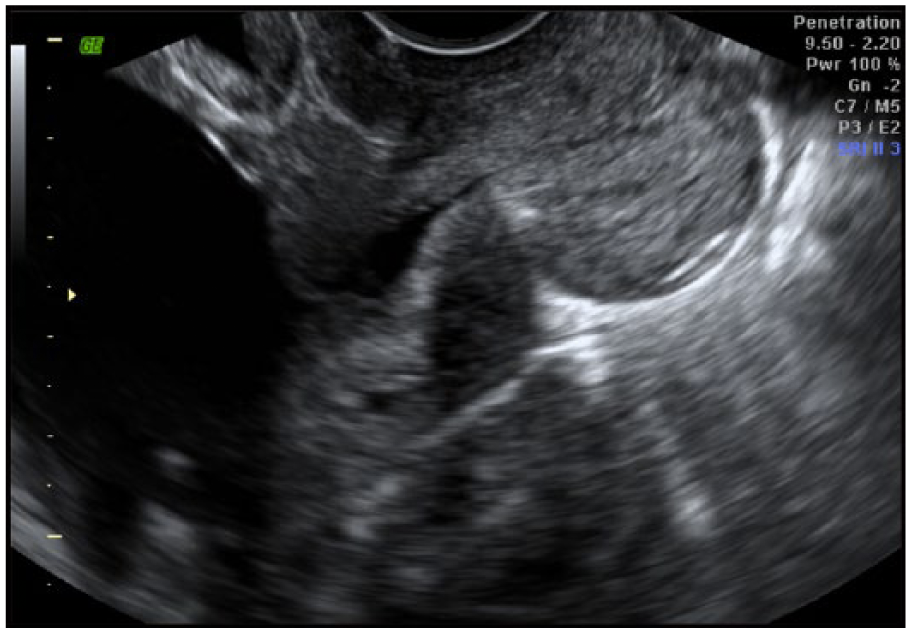
Cerclage suture is identified in the middle portion of the cervix.
Statistical Analysis
Statistical evaluation was made using SPSS for Windows Version 15.0 (IBM Corporation, Armonk, NY). Data were shown as frequency (percentage) or mean ± standard deviation.
Results
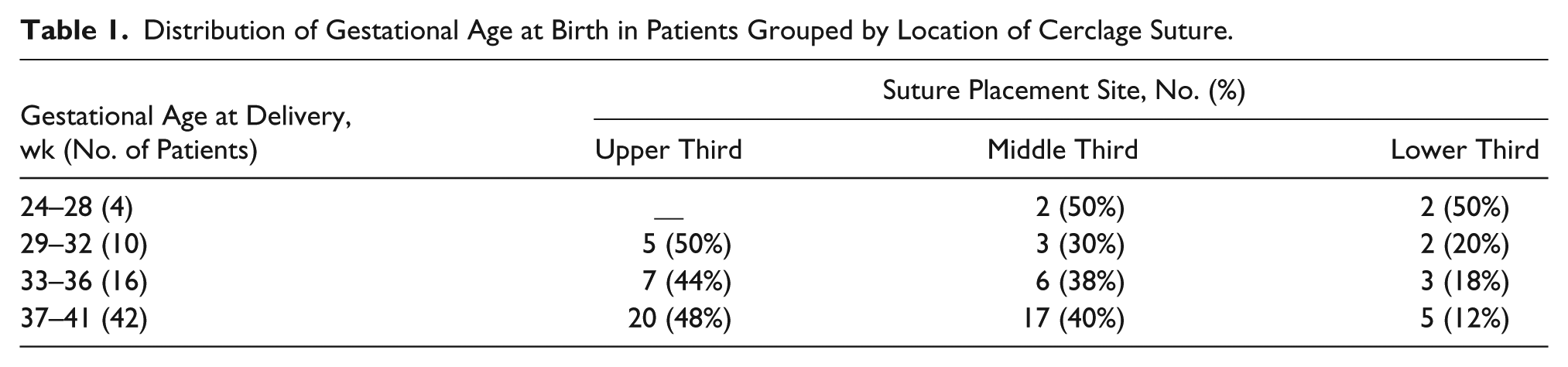
Table 1 references gestational age at delivery time on one axis and the location of the cerclage suture on the other axis.
Distribution of Gestational Age at Birth in Patients Grouped by Location of Cerclage Suture.
Mean and standard deviation of gestational ages at delivery in three subgroups of patients depending on the location of cerclage suture: group 1—suture in close proximity to the internal os (Figure 1), group 2—suture in the midportion of the cervix (Figure 2), and group 3—suture in the lower third of the cervix (Figure 3) (Table 2).
Gestational Age at Delivery in Patients Grouped by Location of Cerclage Suture.
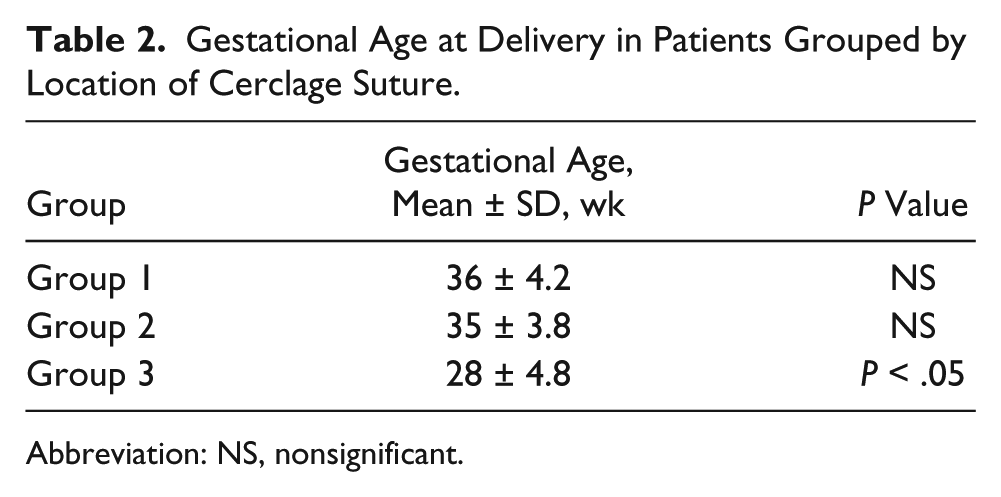
Abbreviation: NS, nonsignificant.
Patients were divided into three groups based on the location of the cerclage suture detected by transvaginal sonography. Patients in whom the cervical cerclage suture was located in the vicinity of cervical os or upper to mid-portion of the cervix gave birth at a mean ± standard deviation of 36 ± 4.2 and 35 ± 3.8 weeks of pregnancy, respectively, versus 28 ± 4.8 weeks for patients in whom the cervical suture was identified in the lower third of the cervix. The difference was statistically significant.
Discussion
The term cervical insufficiency is used to describe the inability of the uterine cervix to retain a pregnancy in the absence of labor. Based on current data, the sonographic finding of a short cervical length in the second trimester is associated with an increased risk of preterm birth. 1 The pathophysiology of cervical insufficiency is poorly understood. Proposed etiologies have included congenital mullerian anomalies and deficiencies in cervical collagen and elastin, among others. 1 Meta-analyses of multiple randomized trials that compared cerclage versus no cerclage in patients with short cervical length during the second trimester concluded that cerclage is associated with significant decreases in preterm birth as well as improvements in neonatal morbidity and mortality. Therefore, cervical cerclage should be considered in women with this combination of history and sonographic findings.9,10 However, as in any surgical procedure, the outcome of cervical cerclage depends, among other factors, on the strong adherence to the proper surgical technique, including choosing the appropriate site of suture placement. This is not always achievable. Placing a sonographically indicated cerclage at a cerclage height (distance from the external os) of 18 mm or greater was associated with a lower incidence of spontaneous preterm birth compared with placing the cerclage closer to the external os. 11 Whereas several randomized studies have assessed the efficacy of sonographically indicated cerclage,12,13 there is a paucity of data on technical aspects of the procedure, which is something the surgeon can sometimes control. The authors analyzed gestational ages at birth in 72 patients in whom cervical cerclage sutures were located in different areas of the cervix.
The strength of our study is that all study participants were carefully selected and limited to singleton pregnancies. No emergency cerclage patients were included. The weakness of the study is that this is a convenience sample and has a relatively small number of patients in each subgroup of patients.
In conclusion, it appears that location of the cerclage may have played a role in the clinical outcome of our limited cohort study. Location of cervical cerclage should be considered in future studies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.