
Abstract
A male patient was referred to radiology with scrotal pain and swelling. Prior to diagnosis, the patient had three sonograms for scrotal swelling, which progressed to a discharging scrotal sinus. At the second scan, a risk factor of past history of pulmonary tuberculosis (PTB) was noted. The first sonogram showed findings suggestive of left epididymitis, the second sonogram showed possible primary testicular tumor or epididymal tuberculosis (EPTB), the third sonogram showed epididymal pathology extending to involve the tunica vaginalis and scrotal wall leading to a sinus tract formation, and the fourth sonogram was normal. This case highlights the sonographic findings during progression of EPTB and the differential diagnosis to consider in such cases. It is a useful educational aid for radiologists and sonographers when evaluating the role of sonography in the management of a patient with scrotal swelling and discharging scrotal sinus.
Tuberculosis (TB) is common worldwide disease. Extrapulmonary tuberculosis (ETB) accounts for 20% to 25% of the total burden of the disease, of which genito-urinary tuberculosis (GUTB) accounts for 4%, with renal involvement being the most common. 1 Epididymal TB is an uncommon entity, hence it can present with diagnostic difficulties.
The aim of this case report is to evaluate the role of diagnostic medical sonography (DMS) in the management of a patient who presents with scrotal swelling, pain, and a discharging scrotal wall sinus. The case report will be useful for continuing professional development for radiologists, sonographers, and referring clinicians. The clinical presentation, sonographic findings, and differential diagnosis in a case of EPTB are discussed.
Case Report
A 34-year-old male of Asian origin presented to the family practitioner (FP) with left scrotal swelling and pain. The patient had no relevant history of sexually transmitted diseases or any family history of testicular or epididymal disease. The patient was started on antibiotics for a presumed diagnosis of epididymo-orchitis. The patient had an urgent scrotal DMS examination in radiology one week after the FP appointment to exclude other pathologies such as testicular tumor. The DMS was performed by a consultant radiologist with more than 15 years of relevant clinical experience. The examination was performed on a Philips HDI5000 (Philips Healthcare, Guilford, UK) ultrasound machine with a high frequency (12-5 MHz) linear array probe in longitudinal and transverse planes with the use of color Doppler (CD). Sonographic findings included an enlarged, mixed echogenicity (heterogeneous) left epididymal tail, which was not hyperaemic (Figure 1A and 1B). The patient improved on antibiotics, and the DMS conclusion was resolving infection (epididymitis). The patient was referred back to his FP with the proviso of repeating the sonogram in four to six weeks if the symptoms did not resolve.
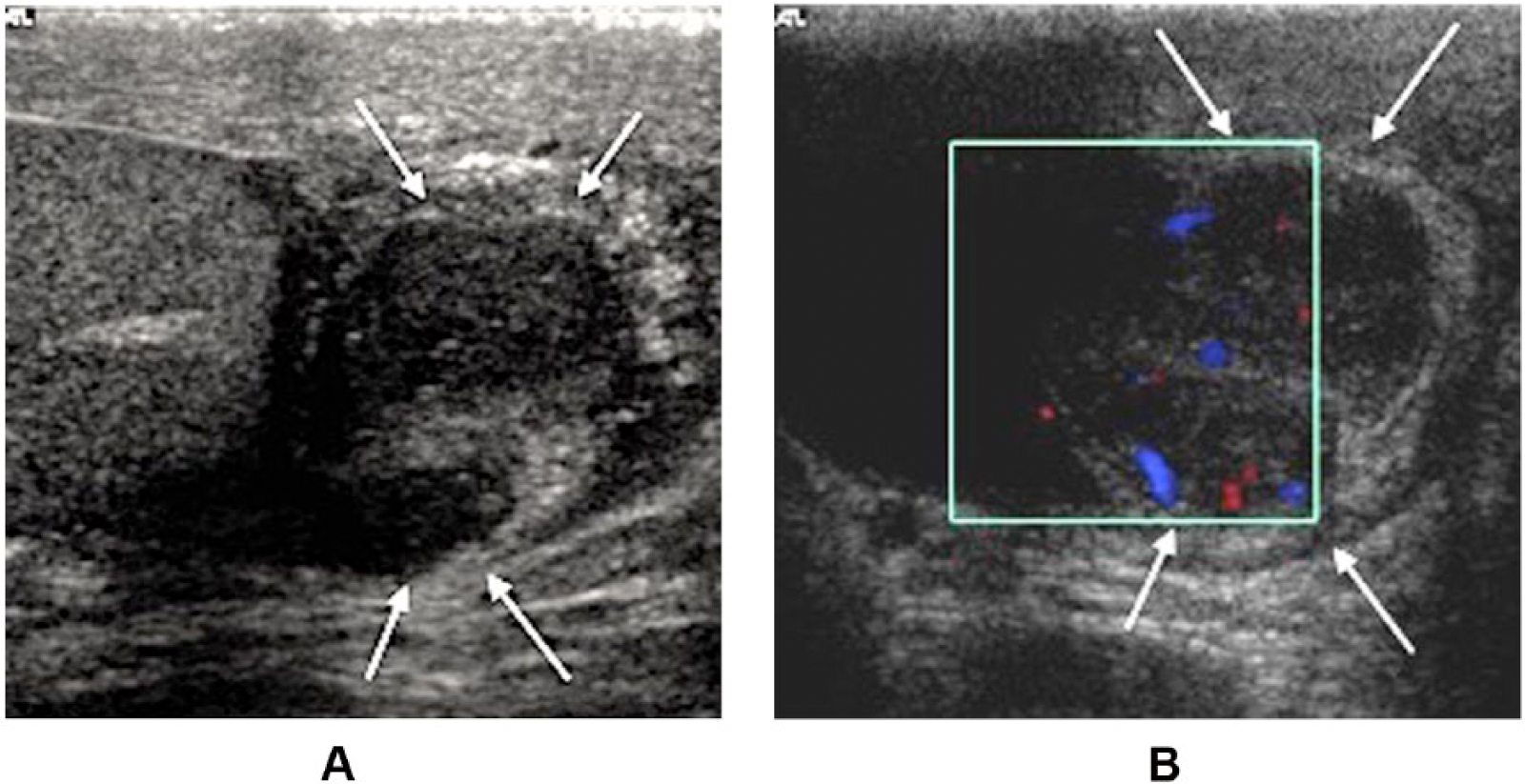
(A) Abnormal left epididymis. Arrows pointing to the enlarged mixed echogenicity of the left epididymal tail. (B) Abnormal left hemiscrotum. Arrows pointing to the left epididymal tail color Doppler, blue (flow away from the probe) and red (flow toward the probe), shows normal blood flow in the left epididymis.
Six weeks later, the patient was referred from the FP for a second DMS as the swelling was persistent and during this period it became apparent that the patient had pulmonary TB 18 months ago and had finished a 6-month course of anti-tubercular treatment. So there was a year’s gap between the patient finishing treatment for PTB and this presentation. The DMS was again performed by a consultant radiologist with more than 15 years of experience. The examination was completed using a Philips HDI5000 (Philips Healthcare, Guilford, UK) ultrasound machine with a high frequency (12-5 MHz) linear array probe. Sonographic findings included an echo poor soft tissue mass in the region of the left epididymal tail, which had increased in size with a suggestion of invasion into the left testis, either due to tumor or EPTB (Figure 2)
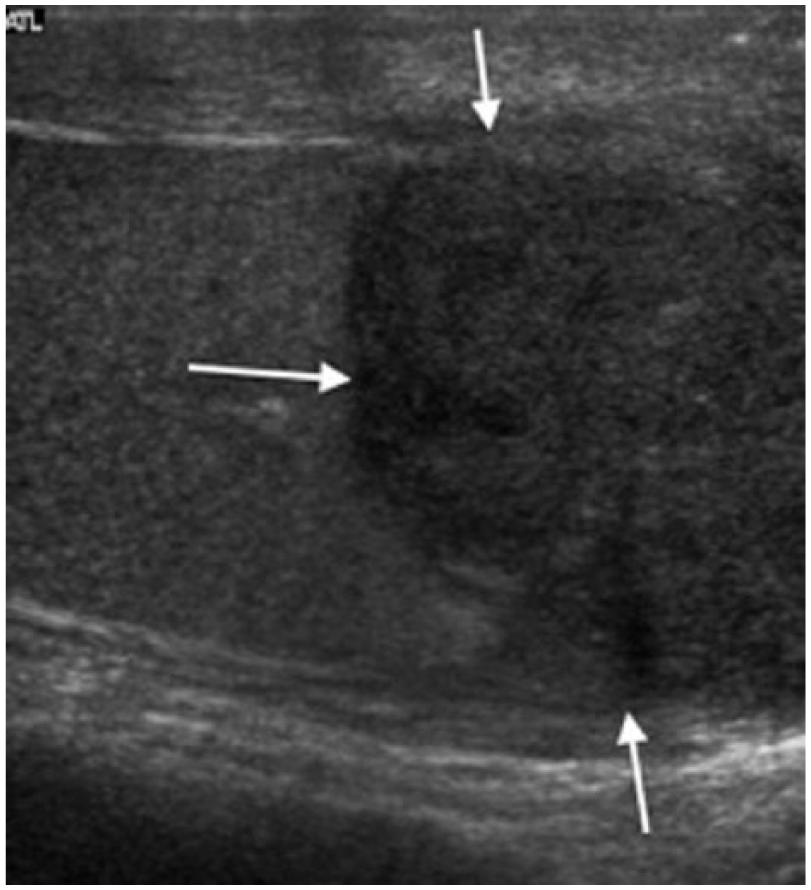
Left testis and epididymis. Arrows pointing to the soft tissue mass in the region of left epididymal tail and lower pole of the testis.
An urgent referral to a urologist was suggested. The patient was seen in the urology clinic, and the evaluation was initiated in the form of tumor markers, semen analysis, and early morning urine sample for acid-fast bacilli (AFB). Discussion at the infectious disease multidisciplinary team (MDT) meeting was arranged, which advised a computed tomography (CT) scan of the chest to look for reactivation of PTB. The tumor markers, semen analysis, CT scan, and early morning urine samples for AFB were all negative. The patient had no treatment during this period.
Eight weeks later, the patient presented to the urology clinic with acute pain, increased scrotal swelling, and a discharging sinus from the scrotal skin. An urgent DMS was performed on the same day, by a sonographer with more than 15 years of experience. The examination was completed using a Siemens Antares Sonoline (Siemens Healthcare, Erlangen, Germany) ultrasound machine with a high frequency (13-5 MHz) linear array probe. Sonographic findings included thickened and hyperaemic left epididymal tail (Figure 3A), epididymal pathology extending to involve the tunica vaginalis, and scrotal wall leading to a sinus tract formation (Figure 3B).
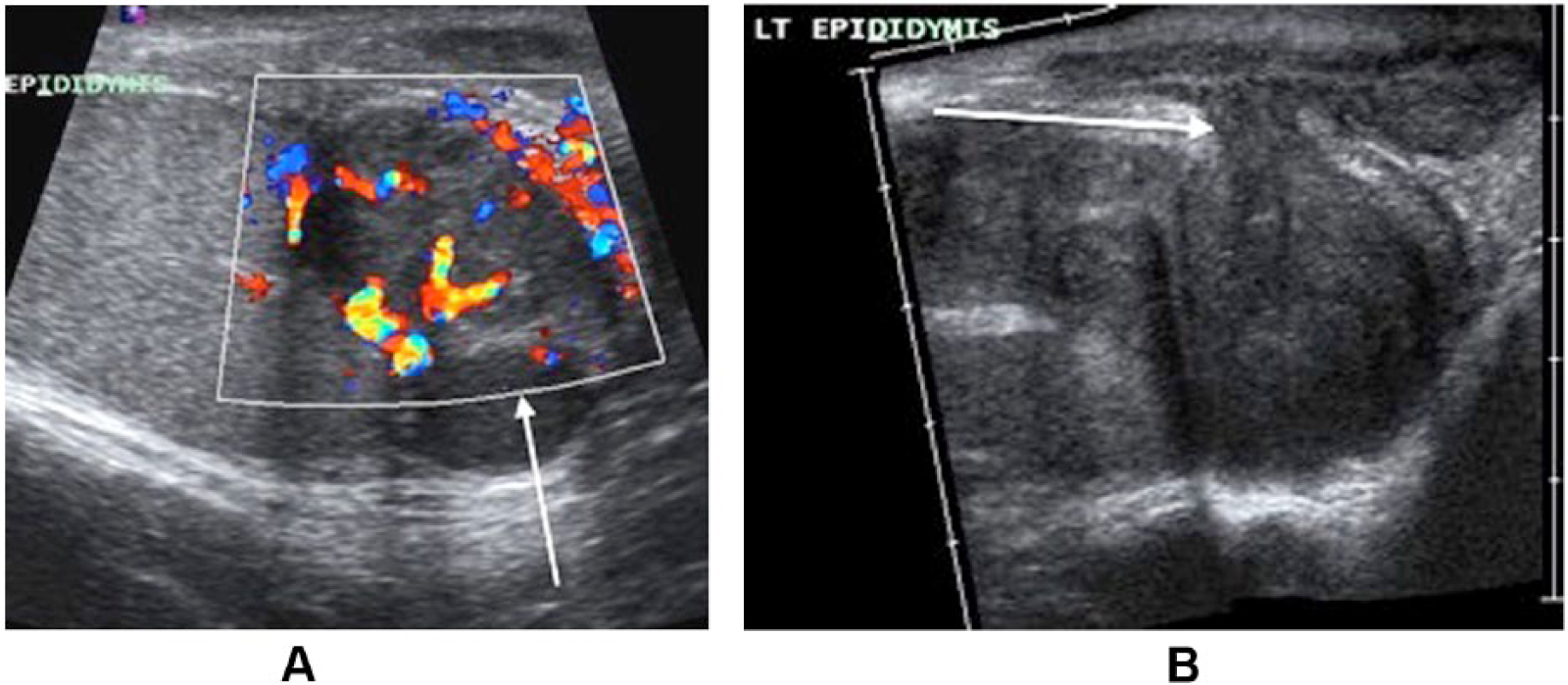
(A) Left testis and epididymis. Arrow pointing to the thickened and hyperemic left epididymis. (B) Extended field of view of the abnormal appearances of the left hemiscrotum. This shows progression of the epididymal tuberculosis from appearances in Figure 2. Arrow pointing to the left epididymal pathology extending to involve the tunica vaginalis and scrotal wall.
Swabs from the discharging sinus confirmed the presence of multi–drug resistant myco-bacterium. Based on the antimicrobial sensitivity, the patient was started on anti-tubercular therapy.
After 18 months of treatment, DMS was performed by a sonographer with more than 15 years of experience. The examination was completed using a Philips iU22 (Philips Healthcare, Guilford, UK) ultrasound machine with a high frequency (12-5 MHz) linear array probe. Sonographic findings included complete resolution of the previously seen left-sided EPTB disease, normal testis, and epididymis (Figure 4).
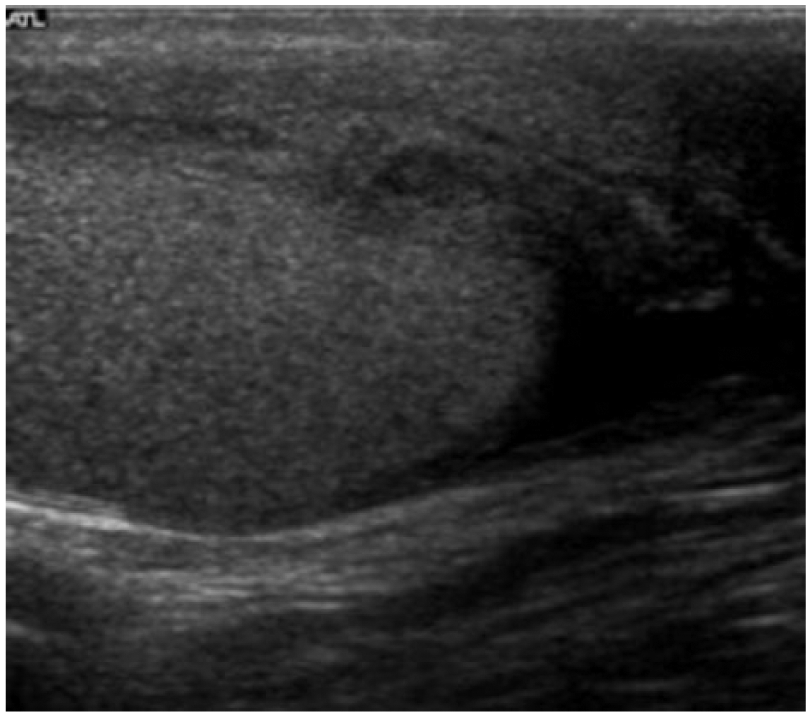
Normal sonographic appearances of the left testis and epididymis 18 months after anti-tubercular therapy.
Discussion
The testes are paired organs in the scrotum. They have a strong organ capsule (tunica albuginea testis). The testicular parenchyma is composed of 250 to 350 lobules, which drain through the mediastinum testis to the epididymis. 2 The epididymis is 5 to 10 mm thick and extends from the upper (head) to the caudal pole of the testis (tail). The epididymis can be divided in caput, corpus, and cauda. A thin capsule and the serosa of the tunica vaginalis cover the epididymis.
Epididymal tuberculosis is the TB involvement of the epididymis. It is an uncommon entity and can account for 20% of GUTB, which in itself is rare. Around 30% to 50% of patients have no history of pulmonary involvement or exposure to tuberculosis. 2
Mycobacterium tuberculosis is the causative organism in TB. The risk factors for TB are: people who live in, come from, or have spent time in a country or area with high levels of TB; are in prolonged close contact with someone who is infected; living in crowded conditions; human immunodeficiency virus (HIV); and having treatments that weaken the immune system. PTB as well as EPTB can be treated by taking several drugs for 6 to 9 months. There are 10 drugs currently approved by the U.S. Food and Drug Administration (FDA). Of the approved drugs, the first-line anti-TB agents that form the core of treatment regimens are isoniazid (INH), rifampin (RIF), ethambutol (EMB), and pyrazinamide (PZA). 3
TB spreads to the epididymis either through retrograde extension from the prostate and seminal vesicles or haematogenously. 4 Infection usually starts in the epididymal tail, as it has a higher blood supply, or it is the first part to be involved in urinary reflux, as was the case in our patient. Patients suspected of EPTB may present with clinical signs and symptoms of a scrotal swelling with or without pain, mass, and a discharging scrotal sinus. 5 The inflammatory process may either revert to an early state of the disease and heal, often with calcifications, or spread to the rest of the epididymis and eventually to the ipsilateral testis. 5
The normal testis has uniform mid-gray or medium-level echoes. The echogenicity of the testis is similar to that of the liver or the thyroid gland. The epididymis has similar or mildly increased echogenicity as compared to the normal testis (Figure 4). 6
EPTB is a difficult diagnosis to make because of the presenting nonspecific clinical symptoms. Differential diagnosis includes non-tuberculous bacterial epididymo-orchitis (EO), primary testicular tumor, or metastases. The range of DMS findings seen in these conditions are: EO-enlarged epididymis with decreased echogenicity; mixed echogenicity enlarged testis with or without scrotal wall thickening; primary testicular tumor—echo poor or mixed echogenicity lesions, which can be hyperaemic; metastases—these can be diffusely enlarged, uniform, or nodular; mixed echogenicity; or echo poor lesion usually with a history of primary elsewhere. Table 1 shows similarities and differences in the sonographic findings of these compared to EPTB.5,7,8
Similarities and Differences in Sonographic Findings for Other Differential Diagnosis Compared to Epididymal Tuberculosis; Derived From Previous Reports and This Report’s Findings.
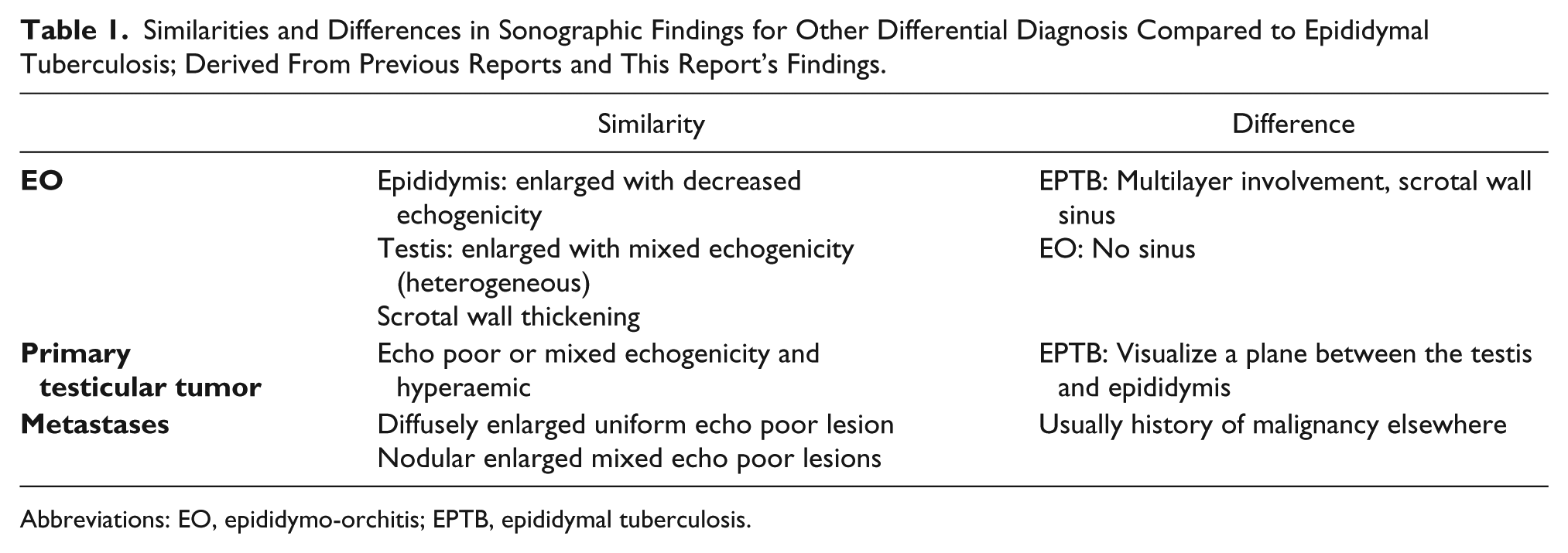
Abbreviations: EO, epididymo-orchitis; EPTB, epididymal tuberculosis.
As disease progresses, the epididymis becomes thickened and hyperaemic, and the pathology eventually extends to the tunica vaginalis and scrotal wall forming a discharging sinus (Figures 3A and 3B).
The other differential diagnosis to consider that can cause discharging scrotal sinuses includes cutaneous actinomycosis, 9 condyloma acuminata, 10 anoscrotal median raphe sinus, 11 and Amyand’s hernia. 12 Most of these conditions are rare, and specific DMS findings in each case are not well established. So a good clinical history and high index of suspicion with other investigations like microbiological swabs from the sinus are required to make the diagnosis along with DMS.
DMS is the best diagnostic imaging modality for evaluation of scrotal contents due to the excellent spatial and contrast resolution. It has 98.5% accuracy in differentiating normal from abnormal and has 99% accuracy in differentiating testicular from extra testicular pathology. 13 It is quick, reproducible, and has no radiation burden. At present, no scientific data are available to determine the validity and reliability (sensitivity, specificity, and reproducibility coefficient) of DMS in the diagnosis of EPTB.
Conclusion
This case shows different stages and progression of sonographic findings as EPTB evolves. When sonographic findings include epididymal herniation through the tunica vaginalis into the scrotal wall, thickened scrotal skin, and a scrotal sinus tract in a patient with known history of TB, the ultrasound practitioner’s decision making should include EPTB in the differential diagnosis. It is a useful educational aid for radiologists and sonographers when evaluating the role of sonography in the management of a patient with suspected EPTB.
Sonography is the gold standard for evaluation of scrotal contents, but before it is deemed as gold standard for diagnosis of epididymal tuberculosis, research is needed, specifically to further understand the disease progression and the process for herniation of the epididymis through the tunica vaginalis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.