
Abstract
Musculoskeletal pain and resulting injury is a growing concern for sonographers. Statistics substantiate the rising trend of sonographers in pain, but prevention methods are not currently established as part of the education process or in the clinical environment. A systematic review of the literature was performed to determine whether sonographers taught to use proper body mechanics, stretching, and/or therapeutic techniques experience less pain. The results suggest that education workshops and stretching techniques have the potential to benefit sonographers. Sonographers who incorporate stretching into the work day may experience a reduction in pain. Education workshops may improve the long-term outcomes for sonographers. Additional research is necessary to determine the outcomes of the various therapeutic methods. Those methods that are proven valuable should be adopted into the sonography profession by educators and clinical sites. Managers, supervisors, physicians, and sonographers should be provided information regarding research outcomes in order to advocate for evidence-based practice changes.
Introduction
Sonographers have struggled with occupational pain for many years. In 1997, Pike et al. 1 performed one of the earliest surveys to evaluate pain perception by sonographers and concluded that 81% of sonographers in the United States reported pain while performing their jobs. Over the past decade, additional research has been performed to explore explanations for the growing number of sonographers who experience debilitating or career-ending pain.
A large part of a sonographer’s work day involves providing diagnostic images of body structures in cardiac, obstetric, gynecologic, abdomen, small parts, or musculoskeletal specialties. 2 Obtaining these images requires steady, applied pressure on the transducer by the sonographer, and use of varied hand and finger, wrist, elbow, and shoulder positions is required to provide optimal viewing angles and maintain contact with the patient.2–4 During each scan, the sonographer must look at a display monitor and evaluate the image, making optimization adjustments and annotations with the nonscanning hand while simultaneously creating the viewable images with the scanning arm. Excessive force and strain may be required to obtain optimal images, especially in the case of obese patients. 5 Although advances in ergonomics have improved the design of tables, chairs, and equipment to ease the burden of musculoskeletal injury to sonographers, repetitive and awkward movements and positions are unavoidable since the sonographer needs to be connected to the patient and the equipment simultaneously.5–7
An ergonomic workstation is only as effective as the person using it, 5 and increased patient volume with lack of rest breaks for sonographers between examinations has exacerbated the problem.2,5 Sonographers under time pressure often take shortcuts, choosing not to readjust rooms or equipment instead of considering their own safety.2,6 Sonographers with dual modality abilities or who have more than one subspecialty within a modality may be expected to perform even more studies during their shifts. 7 Roll et al. 7 reported that the average number of examinations performed per day by each sonographer was between 9 and 11 and that the examinations can last 20 to 45 minutes each. Some sonographers scan for up to 90 minutes at a time for one case. 3 Research has shown that sonographers performing more than 100 studies per month are at risk for developing musculoskeletal disorders.6,8 If sonographers are scanning an average of ten patients per day, then over a 1-month period excluding weekends and call, sonographers could be scanning roughly 230 patients, equivalent to more than double the risk each month.
Musculoskeletal pain and injury is multifactorial, and the perception of pain is subjective and, therefore, difficult to adequately assess.9,10 Vibrations, overuse, excessive force and strain, forceful or awkward movements, poor posture/improper positioning, repetitive motion, and duration of pressure are examples of physical factors that the Occupational Safety and Health Administration (OSHA) has determined to be causes of musculoskeletal injury. 5 Sonographers experience all of the above, except vibrations, during a routine work day. 5 In 2008, the Society of Diagnostic Medical Sonography (SDMS) worked with OSHA to create online toolkits for sonographers and their employers, and the SDMS developed industry standards in 2003, which are also available on the SDMS website.11,12
Increasing evidence suggests that a second set of factors, referred to as psychosocial hazards, may be equally responsible for musculoskeletal injury and pain. 10 These include heavy workloads, night shift hours, poor supervisor support, rapid work pace, overloaded schedules, and overall lack of job contentment. 10 Sonographers corroborate the existence of psychosocial factors, listing increased patient volume, decreased breaks, poor posture, and lack of reporting due to fear of resentment and negative response from their supervisors as reasons for their musculoskeletal injury and pain.2,6 Research has shown that roughly 84% of upper extremity injury developed in workplaces could be connected to psychosocial hazards.10,13–15 Although these findings were not specific to sonography, the relationship is interesting to note, since sonographers experience the majority of their pain in the neck, shoulders, elbows, wrists, and hands. 5 The complex causality of musculoskeletal pain may explain why injury prevention training in sonography education and clinical settings is infrequent. Student sonographers reported that the major focus of their education was scan technique and ergonomics; however, task management, muscle strengthening, and reporting of injury were overlooked in both university and clinical settings. Risk of injury was primarily discussed in the education setting and little mentioned in the clinical environment. 2 Approximately 19% of students did not receive any instruction on musculoskeletal injury. 2
By understanding the psychosocial aspects involved in the development of musculoskeletal pain and resulting injury, sonographers may be able to address potential triggers in their work lives. Sonographers have long held the belief that pain is part of the job; however, sonographers have more control over this aspect of work life than they may have previously realized. The profession as a whole should have greater confidence in promoting prevention and intervention, since musculoskeletal pain and injury are not only career ending in many cases but have also been linked to decreased quality of imaging, which may lead to the increased possibility of medical errors.2,16
The purpose of this research is to determine whether sonographers who are taught to use proper body mechanics, stretching, and/or therapeutic techniques experience less musculoskeletal pain. Specific research questions are as follows:
Does therapy, stretching, posture, or body mechanics have an effect on pain experienced by sonographers?
Do these interventions improve how sonographers use equipment?
Are sonographers who employ these techniques able to return to or continue to work with reduced pain or no pain at all?
Do these therapies need to be continued daily, weekly, quarterly, or annually?
Are sonographers able to maintain these techniques throughout the work day?
Methods
A systematic review was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 Literature searches of electronic databases including PubMed, Scopus, Google Scholar, CINAHL, and Lexicomp were performed between October 2015 and March 2016 using the following search terms: work related musculoskeletal injury, repetitive strain ultrasound, ultrasound ergonomics, work related musculoskeletal disorders, work related musculoskeletal disorders sonographer, work related musculoskeletal disorders ultrasonographer, work related musculoskeletal disorders ultrasound, sonographer stretching, work related musculoskeletal injury rehabilitation, sonographer body mechanics, ultrasound body mechanics, body mechanics for sonographers, and stretching for sonographers.
The search results were screened to determine eligibility. Relevant articles that met the following criteria were selected for inclusion in this review: research articles that addressed methods of therapy and/or body mechanics techniques providing relief from occupational musculoskeletal pain in general, cardiac, and vascular sonographers. Exclusion criteria included: articles not written in English, articles more than 5 years old, and articles about musculoskeletal pain relief therapies used by workers in other professions (Figure 1). The included articles were critically appraised and their significant findings were extracted into an evidence table including primary author, date of publication, research design, study location, population and sample, type of intervention, body parts treated, outcomes, inclusion/exclusion criteria, risk of bias, and limitations. The studies were analyzed qualitatively and results reported in a narrative fashion.
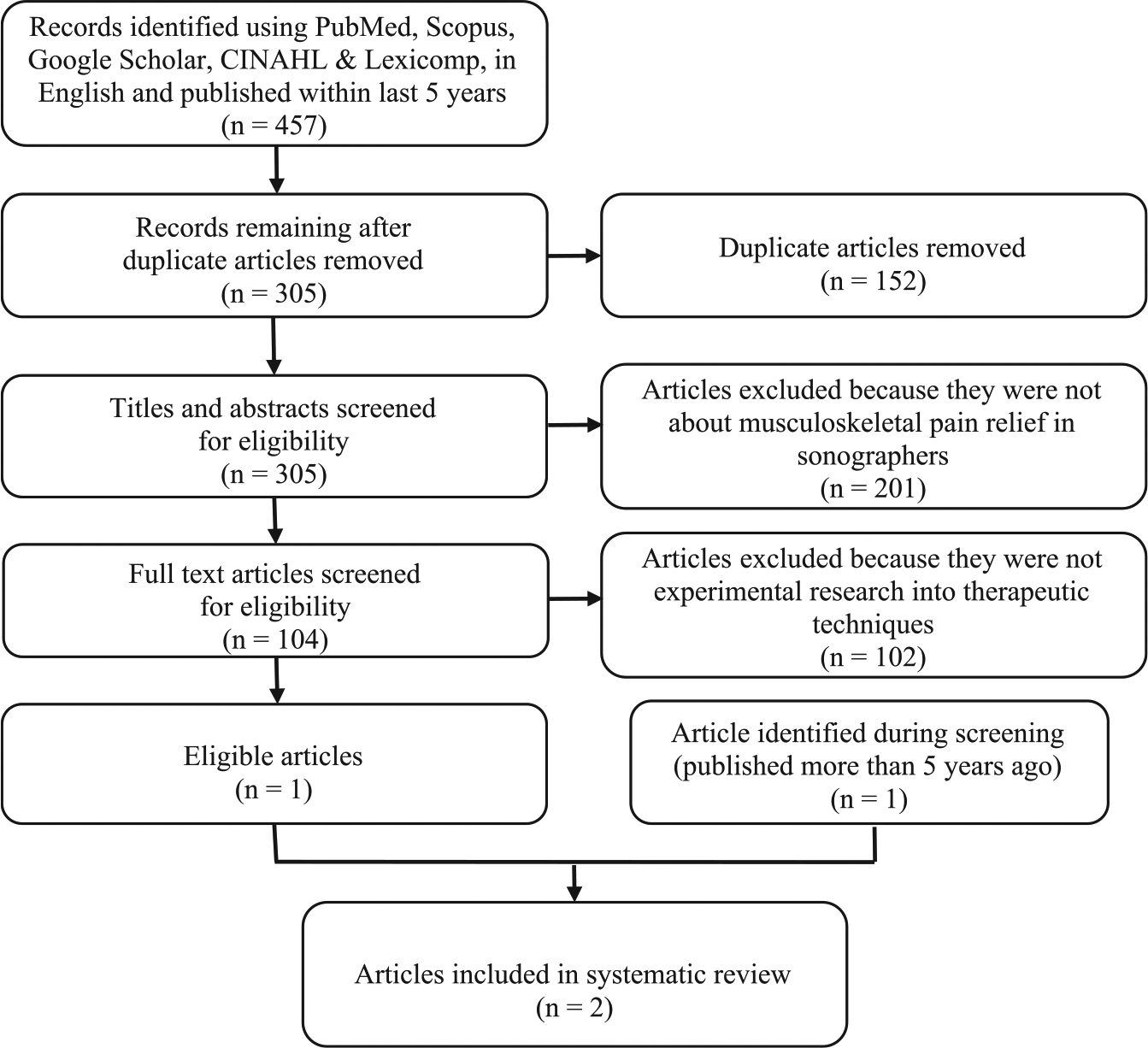
Literature search and article eligibility strategy based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17
Results
Figure 1 shows the search results and process of selecting the included articles. A total of 457 articles was returned from the search terms that were published in English within the past 5 years. After removal of duplicates, 305 articles were screened for titles, abstracts, and/or full texts, and only one article was found suitable for the review. However, during the screening process, a second suitable article was located outside the 5-year publication window, and this article has also been included in the review. Characteristics of and relevant data from these two articles are summarized in Table 1. One article (Christenssen) described musculoskeletal pain reduction in echocardiographers through the use of stretching. 4 The other article (Gibbs and Young) described musculoskeletal pain reduction in sonographers following training in the Alexander technique (AT). 6
Information Relevant to Research Purpose Found in Systematic Review of Available Literature.
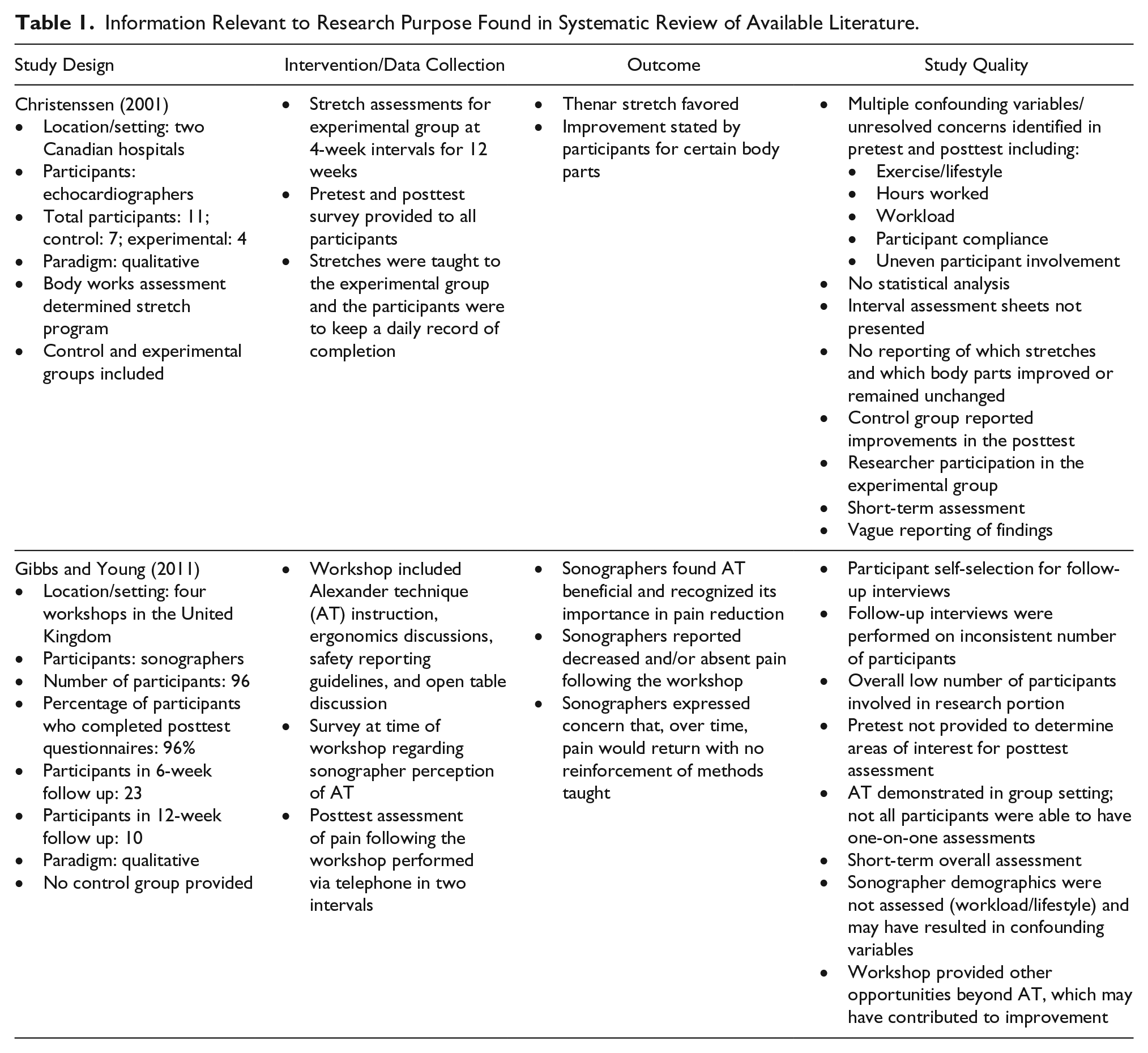
Christenssen’s single blind trial had 11 participants working at two Canadian hospitals—4 in the experimental group and 7 in the control group. 4 With the assistance of a body-works consultant, a 12-week stretching regimen was designed to target specific muscles identified to cause pain during echocardiography. Both groups of participants completed questionnaires at the beginning and end of the 12-week period. The experimental group was instructed to perform and track compliance with the stretching regimen and was interviewed, in a group, by the researcher and body-works consultant every 4 weeks. According to Christenssen, participants in the experimental group reported improvement in musculoskeletal pain after performing stretching exercises for 12 weeks; however, participants found the exercise regimen too time consuming, so they chose their favorite stretches and adapted the schedule to suit their individual needs. Stretching of the thenar muscles of the hands was found to be particularly beneficial, with 75% of the experimental group preferring this exercise. 4
In the United Kingdom, Gibbs and Young hosted workshops to teach sonographers action awareness strategies, known as the Alexander technique, to help prevent or reduce musculoskeletal pain. 6 There were 96 participants over the course of four separate workshops, and 96% of participants completed postworkshop questionnaires. Twenty-three workshop participants received follow-up telephone interviews by the researchers 6 weeks after the workshop, and 10 participants received phone interviews 12 weeks after the workshop. Gibbs and Young reported that 82% of questionnaire participants recognized the relevance of AT, and 85% found it relevant to the practice of ultrasound. More than half of the participants stated that the session was useful, and 37% stated that they could apply it to their work (Table 2). 6 Eighty-seven percent of the sonographers interviewed after 6 weeks stated that their musculoskeletal symptoms had either resolved or decreased, and 80% of the sonographers interviewed at 12 weeks remained symptom free. 6
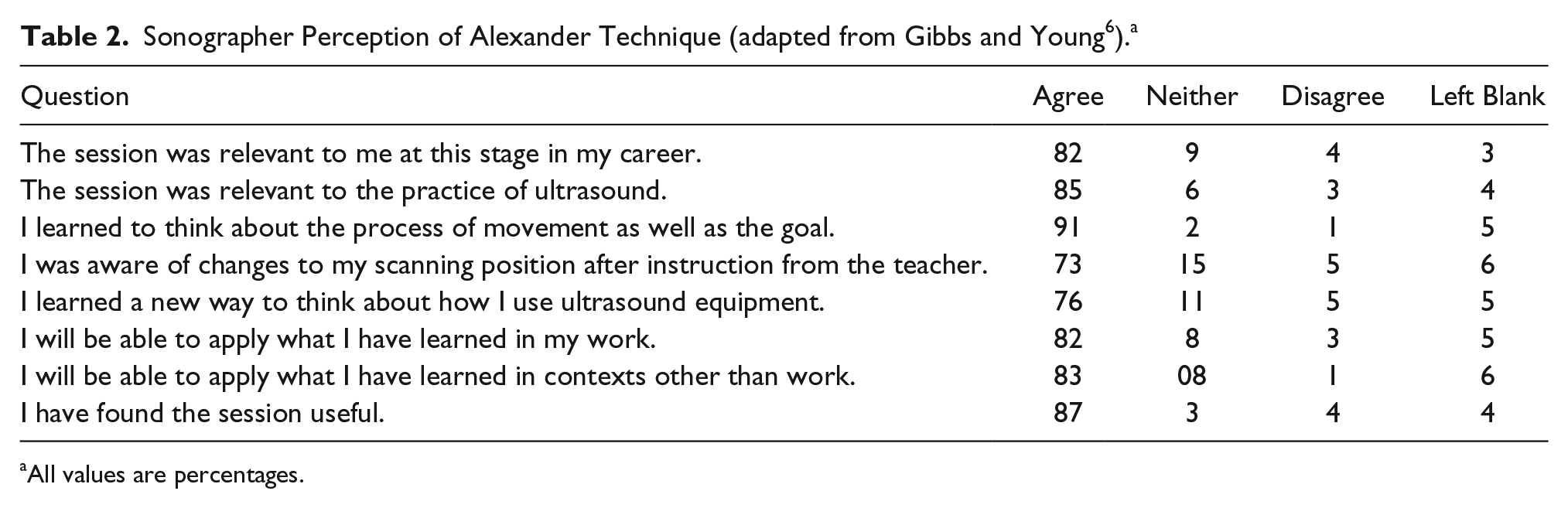
All values are percentages.
Discussion
Considering the high number of published articles describing the incidence of musculoskeletal pain and injury in sonographers, the paucity of research on intervention methods is surprising. Programs designed to promote balance, posture, and positional awareness may reduce pain in sonographers. The AT addresses a wide range of topics including relaxation techniques, stress reduction, reaction control, and improved well-being, which correlate with psychosocial factors attributed to upper extremity pain and injury. The AT improves self-awareness, alters patterns of behavior to improve habits, and redirects negative actions with a hands-on approach and verbal guidance from an instructor. 18 It is likely that sonographers provided the opportunity to participate in an AT workshop or session would benefit from posture awareness. 6 Sixty-eight percent of student sonographers educated on the risks of musculoskeletal pain and injury from poor posture stated that they would be considerate of posture and ergonomics while performing sonograms. 2
Gibbs and Young recommended the AT to combat bad habits in posture, such as alternating between sitting and standing to avoid stuck positions, reducing unnecessary stretching or reaching by asking the patient to move closer, and improving core muscle stability. 6 Sonographers participating in Gibbs and Young’s workshops used the AT to identify and correct behaviors that had previously led to compromised posture, both in overall room set-up and during the process of performing an examination. Relaxation techniques taught in the workshops led to reduced tension in the sonographers when challenged by heavy workload, poor supervisor support, and other work-related stressors. 6 Awareness of posture, relaxation, and corrected bad habits after the workshops reduced the pain that sonographers were experiencing; however, the relief was short lived. Under the pressure of heavy workloads, it did not take long for sonographers to revert to bad habits. 6 Alexander technique sessions can show positive results with as little as six meetings; however, the recommended number of sessions is 30,6,19 and sonographers participating in Gibbs and Young’s study attended only one short group session and lacked one-on-one attention from the instructor. 6 However, the potential exists for sonographers who attend the recommended number of meetings to experience long-term improvement.
Use of stretching received a positive response from echocardiographers in Christenssens’ study. 4 The thenar stretch (Figure 2), where the thumb is stretched away from the hand, proved to be most beneficial and offer the most relief. 4 Echocardiographers use a transducer with a small footprint, and research has shown that the smaller the transducer, the more force is required, and that the greatest force and pressure is in the thumb. 3 Incorporating stretches into the work day may reduce both the severity of pain and the number of body parts that are in pain, as well as improve overall posture and ergonomic use of equipment. 3
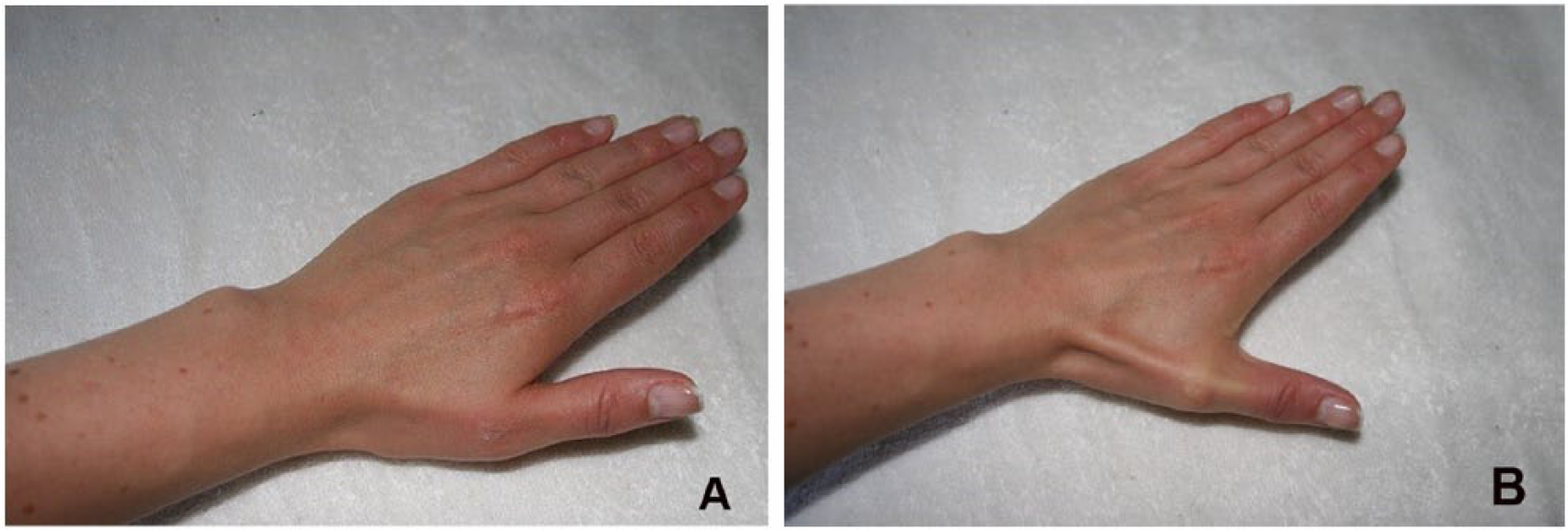
Hand at rest (A). Demonstration of active thenar stretch (B).
This systematic review demonstrates that sonographers who are taught to use musculoskeletal pain prevention techniques may be willing to put those techniques into practice. The result could be that pain decreases or resolves entirely for a short period of time. However, the techniques described provided only a short-term solution for most sonographers, since lack of understanding from employers and overloaded work schedules created a difficult environment for routine incorporation of prevention techniques into the work day.2,4,6 In addition, this review found that sonographers used good body mechanics and equipment ergonomics more readily when its importance was fresh in their minds. Eventually, the pressing nature of psychosocial factors caused the sonographers to resume rushing through processes, forgetting about posture, stretching, or ergonomics and falling back into their old habits.4,6
This systematic review was limited by the small number of relevant publications available in the literature. It is difficult to know whether the results of only two research studies should be generalized to the entire sonographer population. Musculoskeletal pain relief therapies used by workers in other occupations were initially considered for inclusion in this review based on their potential crossover into pain management for sonographers. For example, the profession of information technology may be considered similar to the field of sonography, since both use monitors and keyboard panels; however, the similarities stop there. The focus of this research was to encompass therapies that address the continued, repetitive strain and force and overuse of the scanning arm beyond the use of a computer screen and keyboard panel.
Additional factors limiting the value of the evidence presented in this review are related to the quality of the two included research articles. Both studies contain considerable bias inherent to their methodology and lack objectivity, which makes it difficult to replicate the research or implement the findings in practice. For example, Christenssen was a participant in the experimental group of her own research study, the control and experimental groups were not the same size, and confounding variables such as workload were not controlled. 4 Other instances of sampling and data collection bias may also exist, as the reported methodology was insufficiently detailed. Gibbs and Young used an AT instructor during their workshops. 6 The workshops were abbreviated, with multiple sonographers vying for attention from the AT instructor, and there is no information in the reported methodology addressing how the instructor assessed the individual sonographers’ situations and needs. Gibbs and Young used no control group and only postintervention data collection, which severely limits the validity of their findings. 6 Neither study appears to include reliability or validity testing of the questionnaires, which means that the dependability and credibility of the work is questionable. Overall, for both research studies, it is difficult to determine whether the reported musculoskeletal pain relief was specifically due to the imposed therapeutic techniques.
Conclusion
The results of this systematic review suggest that sonographers who are taught to use proper body mechanics, stretching, and/or therapeutic techniques experience less musculoskeletal pain. Sonographers trained in the AT or in the use of stretching exercises appear to experience reduced or no work-related, musculoskeletal pain. In addition, they are more aware of the importance of good body mechanics and optimized ergonomic arrangement of equipment. However, this review indicates that sonographers need to incorporate the therapeutic techniques into their daily routines so that they become an automatic part of work activities and are not skipped in order to accommodate heavy workload and other psychosocial factors.
There seems to be disconnect between the employer’s and employee’s understanding of the psychosocial aspect of work-related musculoskeletal pain and injury. Online toolkits providing access to assessments of workplace injury, incidence, and follow-up; performance improvement projects; and recommendations for position and body mechanics in relation to performing job duties and supplying consultation would promote a supportive environment.
It is clear that additional research is necessary, taking into consideration the large number of variables and factors that contribute to the complex nature of the problem. This systematic review adds to the overall knowledge base available and may be helpful to managers, physicians, sonographers, and educators in the academic and clinical environments.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.