
Abstract
The purpose of this study was to determine the predictive value of sonography in identifying the receptor status of breast cancer. Sonograms were performed on 73 patients with breast cancer by two experienced sonologists, and the sonographic features such as tumor size, shape, margins, vascularity, posterior acoustic features, and architectural distortion of surrounding tissues were studied. These were then correlated with the receptor status, that is, triple negative versus non-triple negative. Triple-negative breast cancer was associated with large size, circumscribed margins, posterior acoustic enhancement, high vascularity, and lack of architectural distortion. Non-triple-negative breast cancer tumors revealed smaller sizes with spiculated margins, posterior shadowing, lower vascularity, and architectural distortion of surrounding tissues. Sonography revealed a high sensitivity and specificity (84.0% and 81.2%, respectively) on multivariate analysis for identifying receptor status prospectively. Interobserver agreement was also good. In conclusion, sonography may play a valuable role in prospectively predicting the receptor status in breast cancer and can serve as a potential tool for detecting triple-negative cancer.
Breast cancer is the most common cancer among women in the world, with a rising incidence. 1 It is a heterogeneous disease with a varied morphologic appearance, molecular features, behavior, and response to treatment. Currently, clinical management of breast carcinoma patients depends on pathologic prognostic and predictive factors that enable decision making among various treatment options for these patients. 2
Breast cancer patients are subcategorized into hormone receptor (estrogen receptor [ER]/progesterone receptor [PR]) positive, human epidermal growth factor receptor 2 (HER2) positive, or both hormone receptor and HER2 negative. The treatment offered varies accordingly; the patients who are ER/PR positive show good response to hormonal therapy, whereas HER2-positive patients show good response to trastuzumab (Herceptin). Triple-negative breast cancer (TNBC) is a subcategory that lacks expression of all three receptors, that is, ER, PR, and HER2. This group of tumors is associated with a poorer prognosis. They usually present at a younger age, exhibit higher histologic grade, have larger size, have higher chances of distant metastasis, and have higher recurrence rates as compared with non-TNBC.3,4 Therefore, early identification of the receptor type of breast cancer has important prognostic relevance and management implications.
In recent years, some studies have focused on the imaging of breast carcinoma with modalities like mammography, fluorodeoxyglucose positron emission tomography, sonography, and magnetic resonance imaging and have correlated them with the pathologic prognostic factors with encouraging results. It has been found that the typical features of malignancy may not appear on mammography in some TNBC patients,5,6 thus highlighting the need for an alternate and adjuvant imaging tool that can help in an early, accurate diagnosis in these patients. The pathologic analysis of ER/PR and HER2 status requires biopsy followed by laboratory testing. However, biopsy is invasive and these sophisticated tests may not be readily available in all countries. In comparison, sonography is a noninvasive, readily available, cost-effective modality.
Few recent studies have found sonographic features such as tumor size, margins, echotexture, and posterior acoustic parameters to vary significantly between TNBC and non-TNBC cases.7–12 All the previous studies, to the best of our knowledge, are retrospective in nature. This study prospectively correlates the various ultrasound features of breast cancer with estrogen, progesterone, and HER2 receptor status.
Materials and Methods
After receiving approval from the institutional ethical committee and informed consent from all participants, we undertook this prospective study at a tertiary care hospital in Delhi, India, between November 2013 and March 2015. Seventy-three female patients with histologically proven breast cancer were included in the study. Patients with a history of breast biopsy, surgery, or neoadjuvant chemotherapy and patients refusing to give consent were excluded.
The clinical data regarding patient age, presenting symptoms, duration of symptoms, and location of lump were recorded. All patients were clinically examined by a surgeon and details of location, size, and consistency of mass were documented.
Sonography
High-resolution real-time scanning was performed independently by two well-trained breast sonologists using a linear broadband 7.5- to 10-MHz transducer on an ATL HDI 5000 ultrasound machine (Philips Ultrasound, Bothell, WA, USA), an HD7 XE color Doppler ultrasound system (Philips Ultrasound), and a SONOLINE Antares ultrasound machine (Siemens, Munich, Germany). Both sonologists examined each patient independently, preferably on the same day or at best the next working day. Multiple images were obtained in both longitudinal and transverse planes through all breast lesions by keeping the patient in supine and oblique positions. The maximal longitudinal and transverse dimension was recorded for each lesion. In cases where multiple lesions were present, the largest lesion was examined. This lesion was then marked just prior to surgery to ensure histopathologic correlation from the same.
The tumor characteristics were assessed using the BIRADS sonography lexicon. 13 The following sonographic characteristics were considered:
The vascularity of a lesion was assessed on color Doppler imaging by using the smallest possible gate and a low pulse repetition frequency. It was subjectively classified into four categories:
These features were analyzed and rated by two sonologists independently. In case of interobserver disagreement, a consensus was developed by a joint second reading of both sets of images, and the patient was recalled in only two cases where no consensus could be reached. The sonologists were blinded to the clinical and pathologic analysis findings.
Pathologic Analysis
All patients underwent surgery (lumpectomy/modified radical mastectomy) depending on the stage of the tumor and the discretion of the operating surgeon, and the surgical specimen was sent for histopathologic analysis. Formalin-fixed and paraffin-embedded tissue samples were analyzed for tumor grade and presence of hormone receptors ER, PR, and HER2.
Tumor grade was classified according to the Nottingham combined histologic grading system 14 for invasive cancers on the basis of gland and tubule formation, nuclear pleomorphism, and mitotic index. Grades 1 and 2 were labeled as low grade, and grade 3 was taken as high grade for the purpose of this study.
Estrogen and progesterone receptor and HER2 expression status was assessed by immunohistochemistry (IHC). Standard techniques were followed. Briefly, sections were boiled in citrate buffer for antigen retrieval and treated with methanol and hydrogen peroxide for quenching endogenous peroxidase activity prior to primary antibody application (ER: clone SP1, PR: clone SP2, both dilutions 1:200; HER2: clone SP3, dilution 1:100; all antibodies were rabbit monoclonal). The reaction was detected using a horseradish peroxidase polymer-based universal kit and DAB chromogen.
For interpretation of IHC, guidelines recommended by the College of American Pathologists were followed. 14 Estrogen and progesterone receptors are immunolocalized in tumor nuclei (Figure 1a, b). Their expression was evaluated by Allred score, 14 which takes into account both intensity of staining and proportion of tumor cells. Total scores of 0 and 2 were considered negative and 3 to 8 were interpreted as positive.
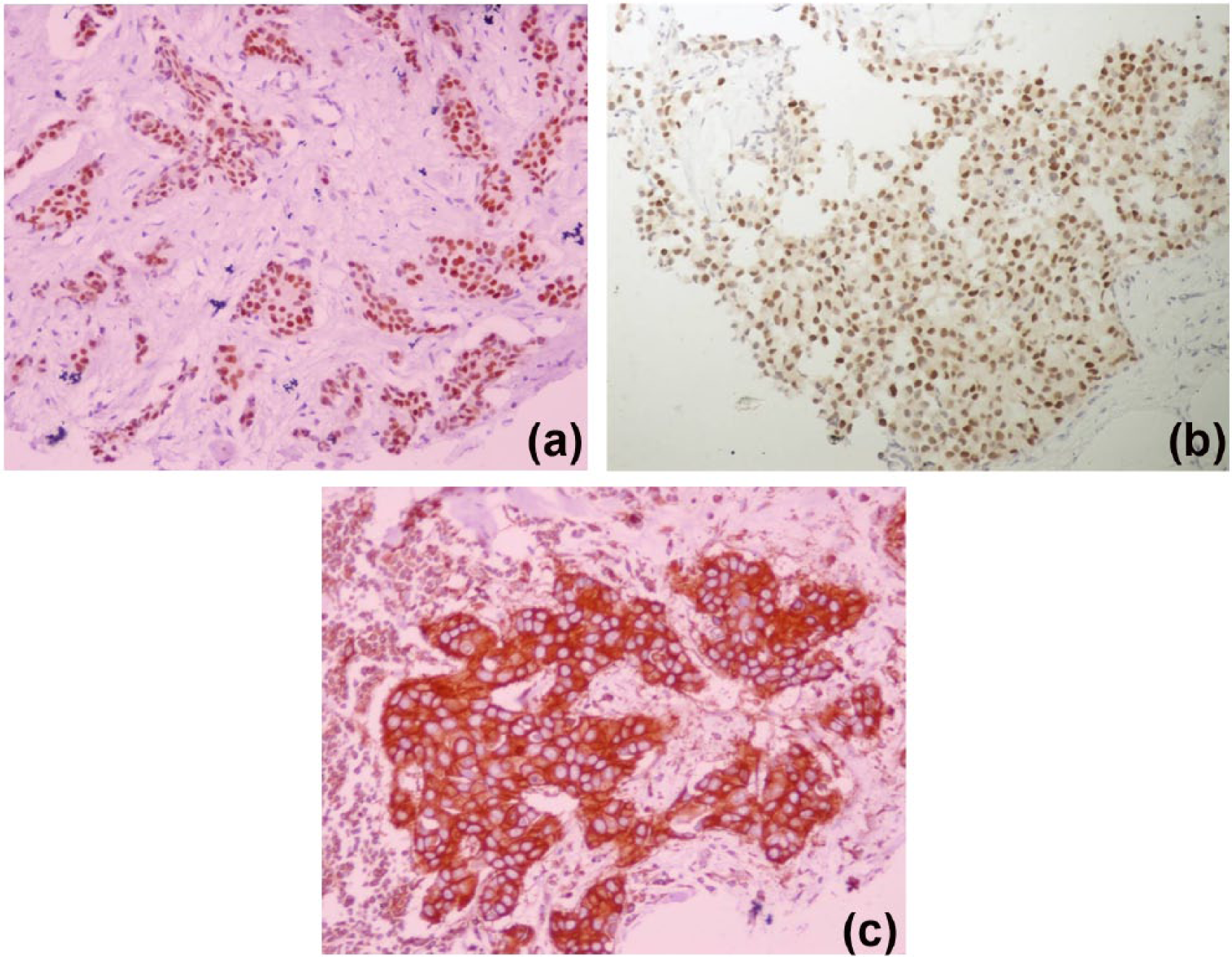
(a) Positive estrogen receptor immunohistochemistry with an Allred score of 8 due to strong nuclear staining (score 3) in almost all tumor cells (score 5) (200×). (b) Positive progesterone receptor immunohistochemistry with an Allred score of 7 due to moderate nuclear staining (score 2) in almost all tumor cells (score 5) (200×). (c) Positive human epidermal growth factor receptor 2 immunohistochemistry. There is complete and intense membranous staining in almost all tumor tissue.
HER-2 immunostaining was observed in tumor cell membrane. Cases with complete, intense circumferential membrane staining in > 10% of invasive tumor cells were considered positive (Figure 1c). For the purpose of this study, cases with equivocal results were considered negative.
Statistical Analysis
The sonographic and pathologic features of all the patients were tabulated. The comparison of data was done and the relation between the sonographic and pathologic data was expressed in the form of percentages.
The interobserver agreement for reliability of ultrasound measures was assessed by using Cohen Kappa statistics. Kappa values exceeding 0.75 represented excellent agreement, values between 0.40 and 0.75 represented fair to good agreement, and values less than 0.40 represented poor agreement. Group differences for continuous characteristics were assessed using a Wilcoxon rank sums test, and for categorical characteristics, a normal (Pearson) chi-square test was used. Fisher exact test was applied to calculate the P value of various parameters and thus to define the level of significance. Odds ratios (ORs) of the significant parameters were calculated and the corresponding sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), where possible, were calculated.
Multivariate analysis was done for calculation of combined sensitivity and specificity of significant parameters. A receiver operating characteristics (ROC) curve was plotted using the SPSS software, and area under the curve was used to evaluate the diagnostic value of combined parameters and thus to decide the cutoff value. The logistic regression model was used to combine the results from multiple tests to increase the diagnostic accuracy.
Results
Out of 73 cases, 21 (28.8%) were ER/PR positive, HER2 negative (luminal A type); 22 (30.1%) were ER/PR positive, HER2 positive (luminal B type); 5 (6.8%) were ER/PR negative, HER2 positive (HER2 type); and 23 (34.0%) were basal type (triple negative). Thus, 48 (66%) had one or more positive receptors (termed as non-TNBC) and 23 (34%) were triple negative (termed as TNBC). All parameters were compared between these two groups.
The age range of the study sample was 25 to 84 years with a mean age of 48 years. There was no significant difference between the ages in the two groups. The presenting symptoms included lump in the breast, heaviness in the breast, nipple discharge, or pain in the breast. The majority of the patients (63%) presented only with a painless lump in the breast. The most common site was in the right outer upper quadrant (Table 1).
Clinical and Histopathologic Data of Triple-Negative Breast Cancer (TNBC) and Non-Triple-Negative Breast Cancer (Non-TNBC) Groups.
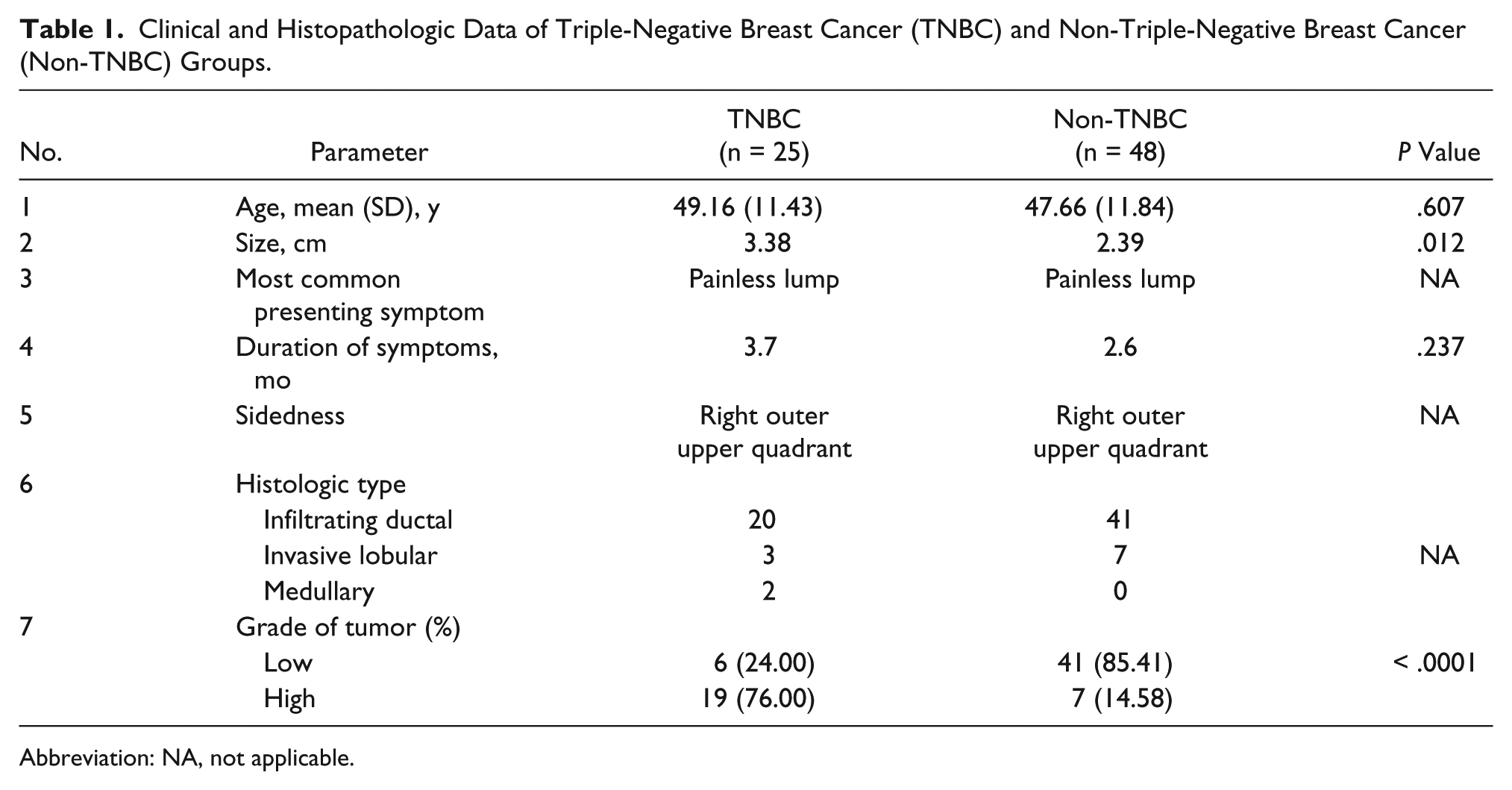
Abbreviation: NA, not applicable.
The average duration of symptoms was slightly longer among TNBC cases (3.7 vs 2.6 months), but the difference was not statistically significant (P = .237). The mean tumor size estimated by ultrasound was larger in TNBC cases as compared with non-TNBC cases (3.38 vs 2.39 cm, P = .012) (Table 1). The majority of TNBC cancers (76%) were high grade as opposed to non-TNBC, of which 86% were low grade on histology.
Correlation of the sonographic findings between the two groups (TNBC vs non-TNBC) is illustrated in Table 2. An oval or round shape was seen in the larger number of TNBC cancers than non-TNBC (72% vs 58% for oval and 20.0% vs 12.5% for round), whereas an irregular shape was more common in non-TNBC cases (29% vs 8%), although this difference was not statistically significant (P = .857) (Figures 2, 3). Overall, horizontal orientation was found in 43.8%, whereas vertical and indifferent orientation was seen in 26.0% of cases. No significant difference was seen between the two groups.
Distribution of Sonographic Parameters in Triple-Negative Breast Cancer (TNBC) and Non-Triple-Negative Breast Cancer (Non-TNBC) Groups.
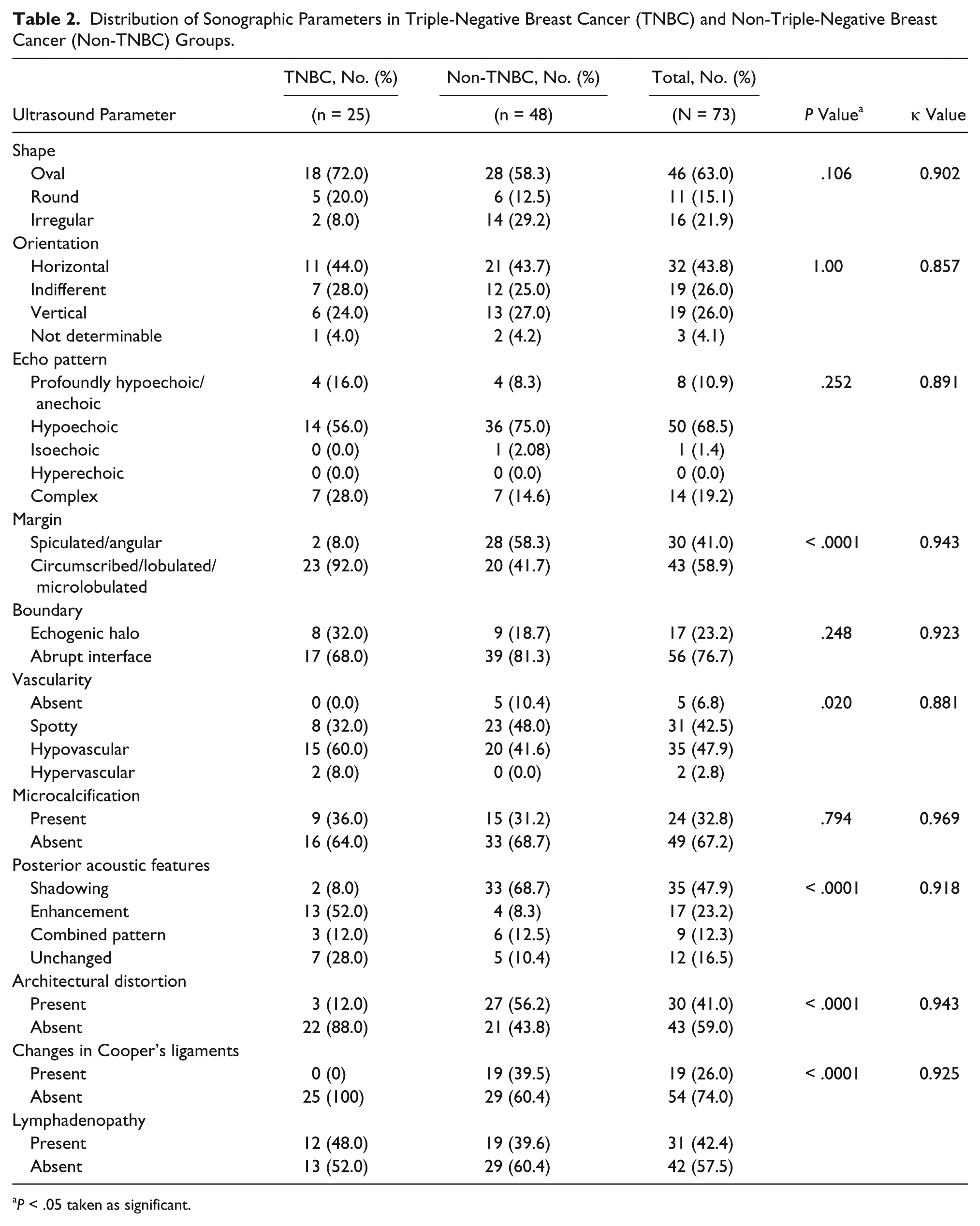
P < .05 taken as significant.
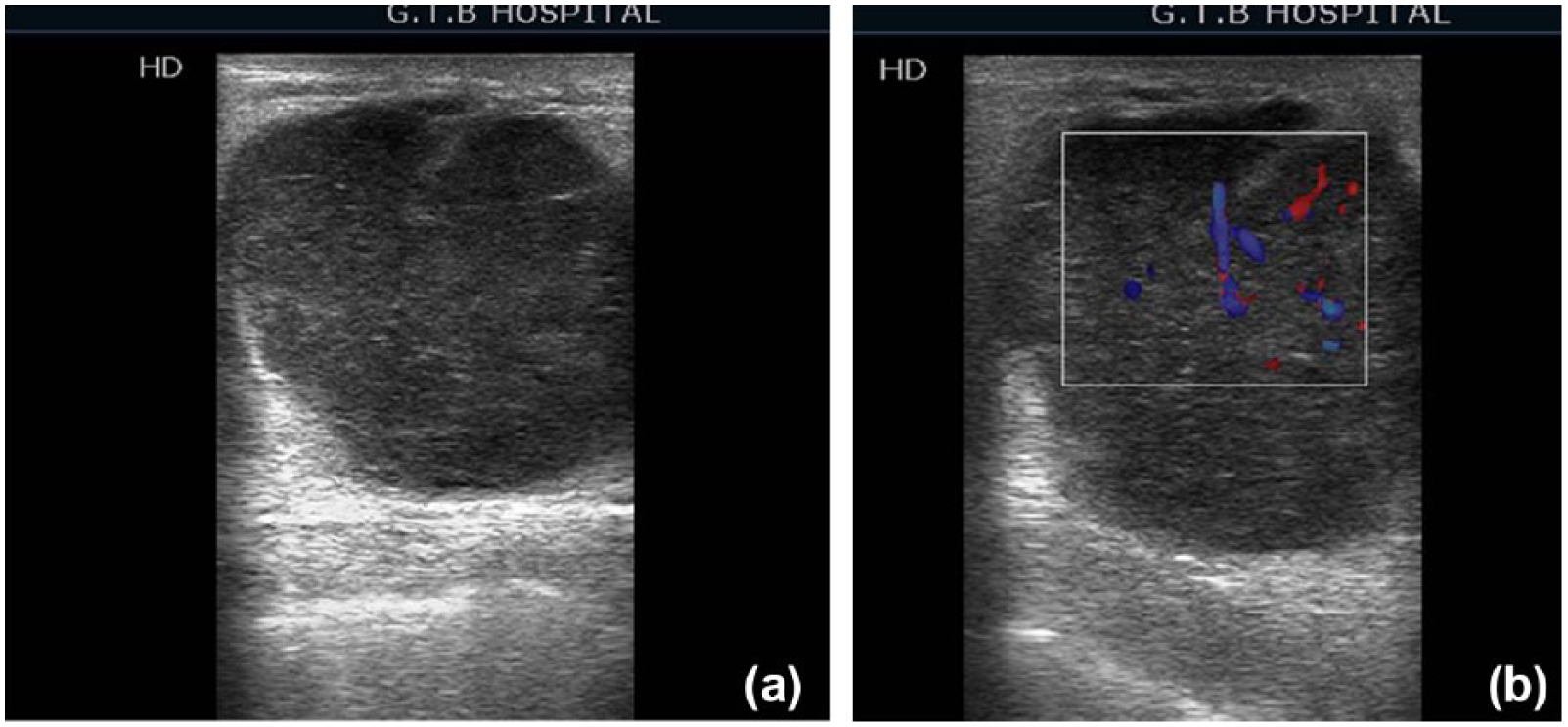
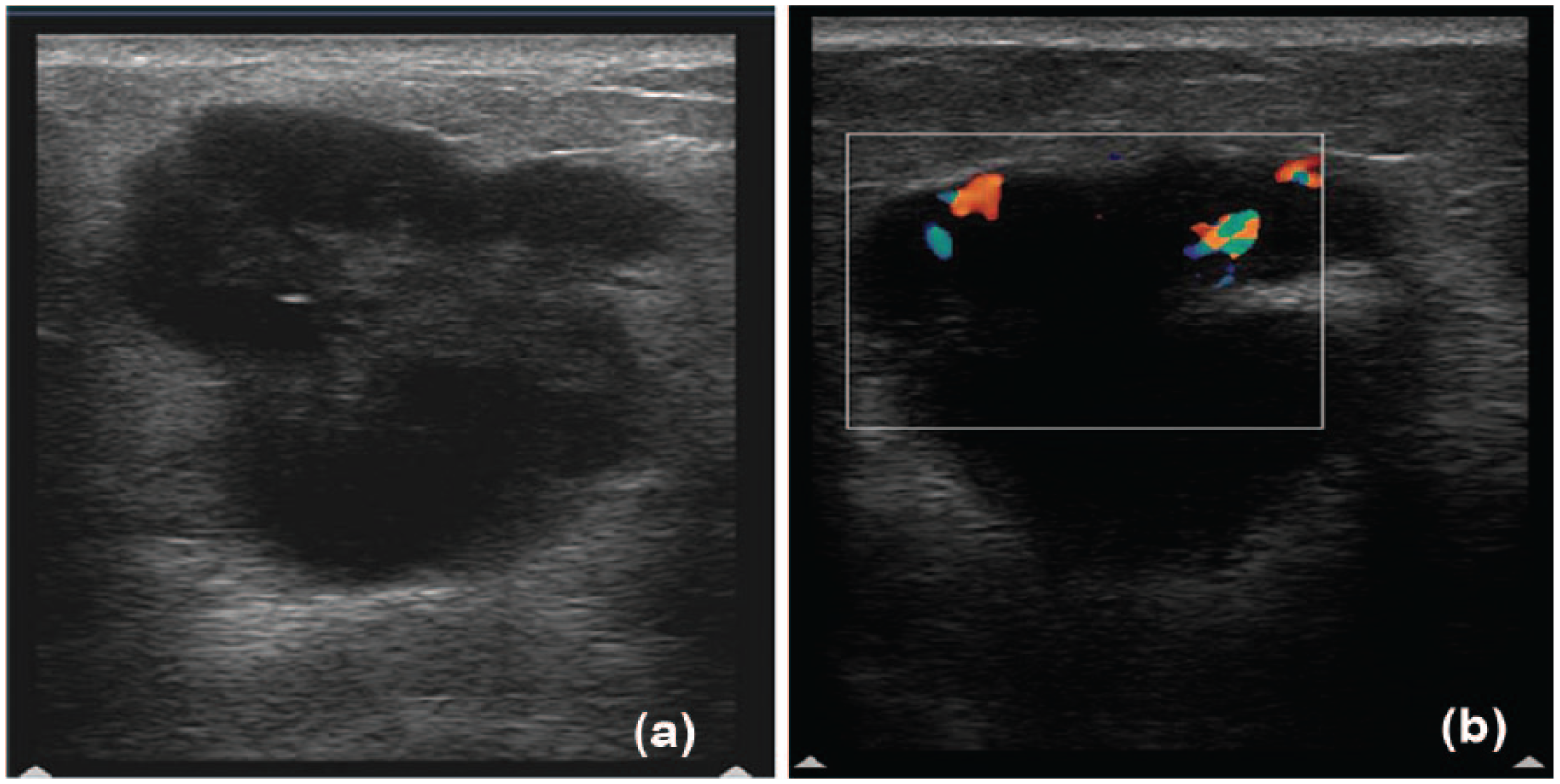
Triple-negative breast cancer. (a) Sonography shows a round hypoechoic mass with well-circumscribed margins, posterior enhancement, absence of architectural distortion of surrounding tissues, and no Cooper’s ligament changes. (b) Lesion shows high vascularity with color Doppler imaging.
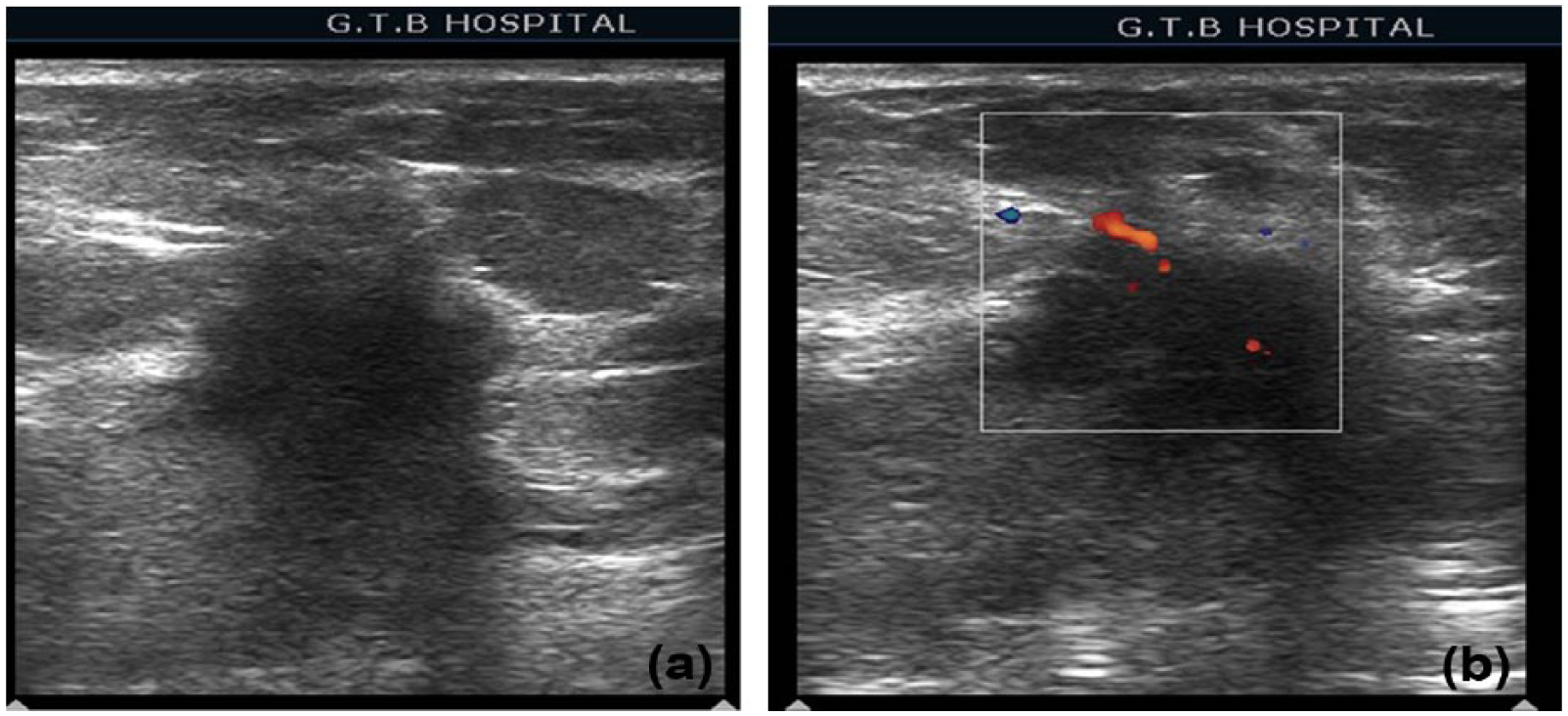
Triple-negative breast cancer. (a) Sonography demonstrated a profoundly hypoechoic mass with lobulated margins and unchanged posterior features (lack of posterior shadowing). (b) Lesion shows moderate (20%) vascularity with color Doppler imaging.
Around 68% of cancers demonstrated a hypoechoic pattern on the sonogram, 20% were complex appearing, and none were hyperechoic. Although the echogenicity could not distinguish TNBC from non-TNBC, profoundly hypoechoic (16% vs 8%) and complex patterns (28% vs 14%) were seen in a higher number of TNBC cases compared with non-TNBC cases (Figures 2-5).
Estrogen receptor/progesterone receptor and human epidermal growth factor receptor 2 positive case (nontriplenegative breast cancer). (a) Sonography shows an irregular hypoechoic lesion having spiculated margins, causing posterior acoustic shadowing, architectural distortion of surrounding tissue, and Cooper’s ligament disruption. (b) Lesion demonstrates spotty vascularity (< 20%) on color Doppler imaging.
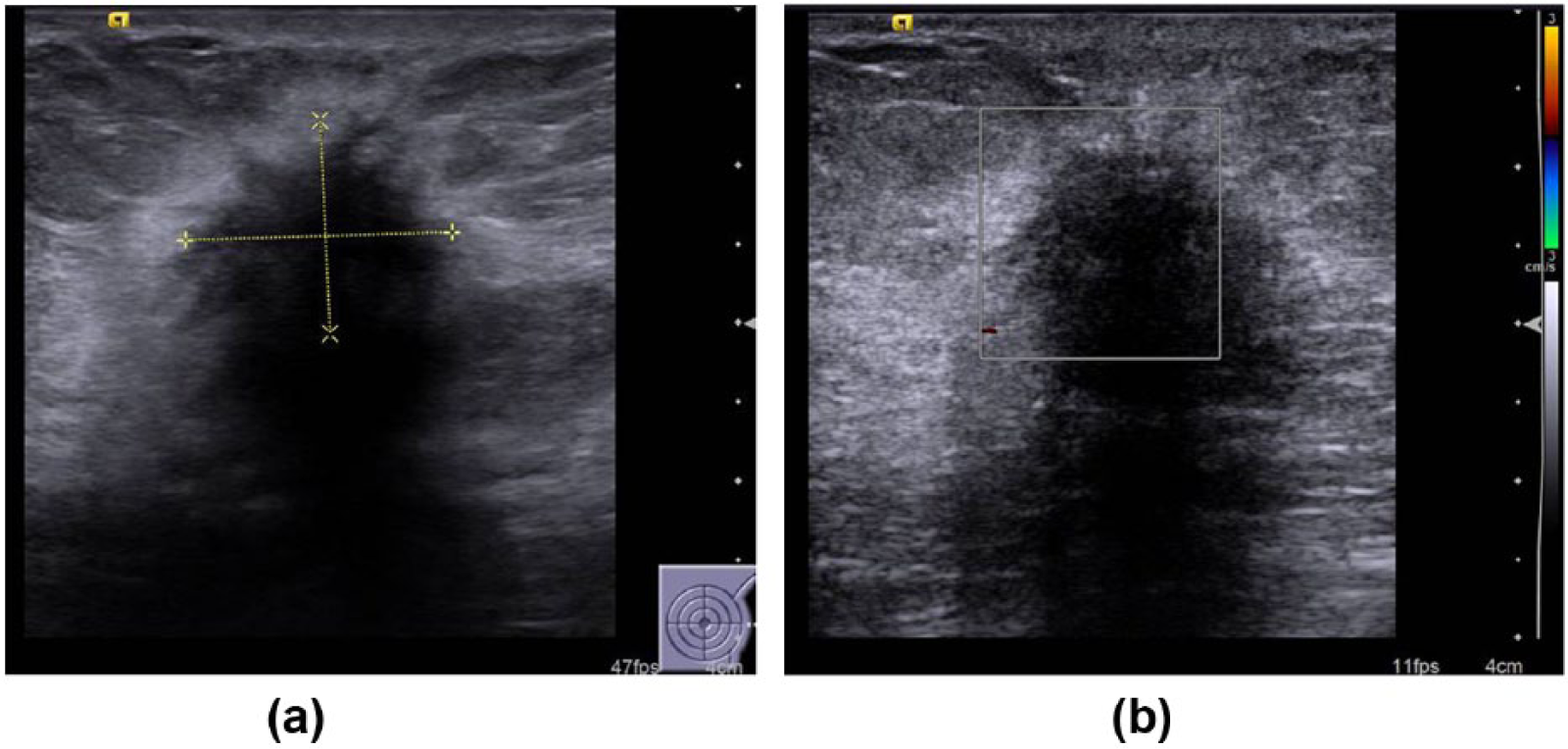
Estrogen receptor/progesterone receptor positive human epidermal growth factor receptor 2 negative case (nontriplenegative breast cancer). (a) Sonography reveals a hypoechoic, spiculated mass lesion with dense posterior acoustic shadowing, architectural distortion of surrounding tissues, and an echogenic halo. (b) Lesion appears avascular with color Doppler imaging.
The margin is said to be circumscribed if there is an abrupt transition between the lesion and surrounding tissue. There was a trend for circumscribed or microlobulated margins in TNBC compared with non-TNBC (92% vs 42%). On the other hand, spiculated margins were significantly associated with non-TNBC cases and were rarely seen in TNBC (93% vs 7%) (P < .0001). Tumors with circumscribed margins were calculated to have 16 times more likelihood of being TNBC (sensitivity = 93%, specificity = 53%, and OR = 16), whereas tumors with spiculated margins had 21 times the likelihood of being receptor positive (sensitivity = 53%, specificity = 93%, and OR = 21) (Tables 2-4 and Figures 2-6).
Significant Parameters That Are Positively Associated With a Triple-Negative Breast Cancer Receptor Status on Univariate Analysis.
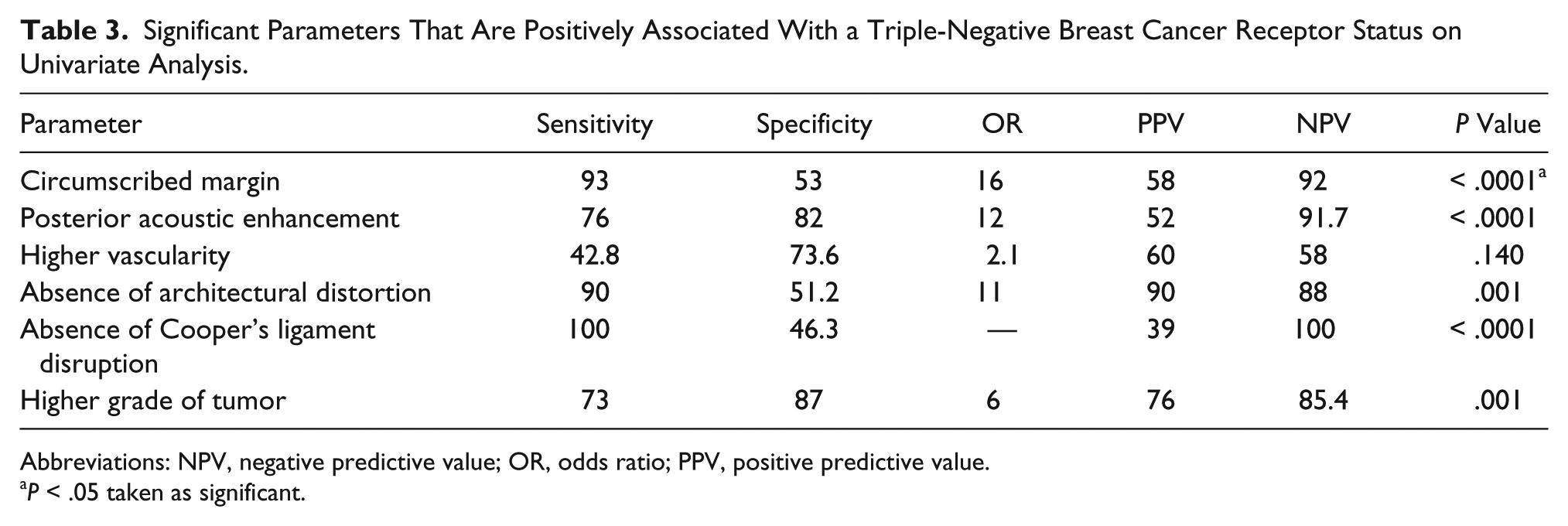
Abbreviations: NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value.
P < .05 taken as significant.
Significant Parameters That Are Positively Associated With a Non-Triple-Negative Breast Cancer Receptor Status on Univariate Analysis.
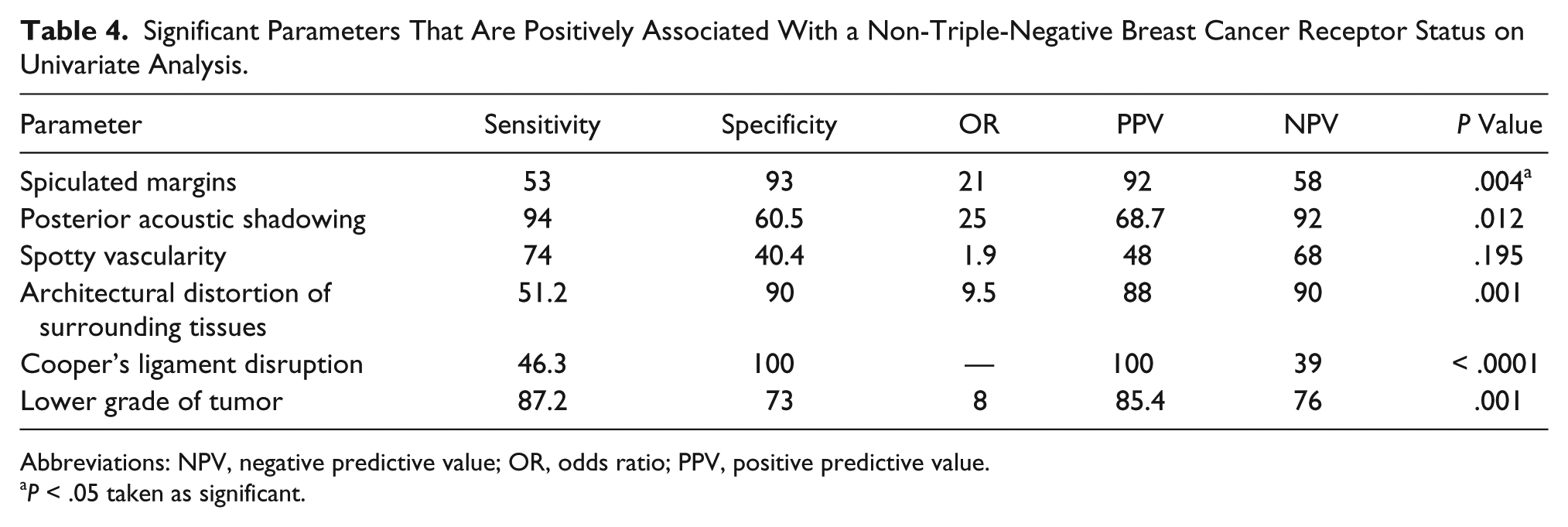
Abbreviations: NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value.
P < .05 taken as significant.
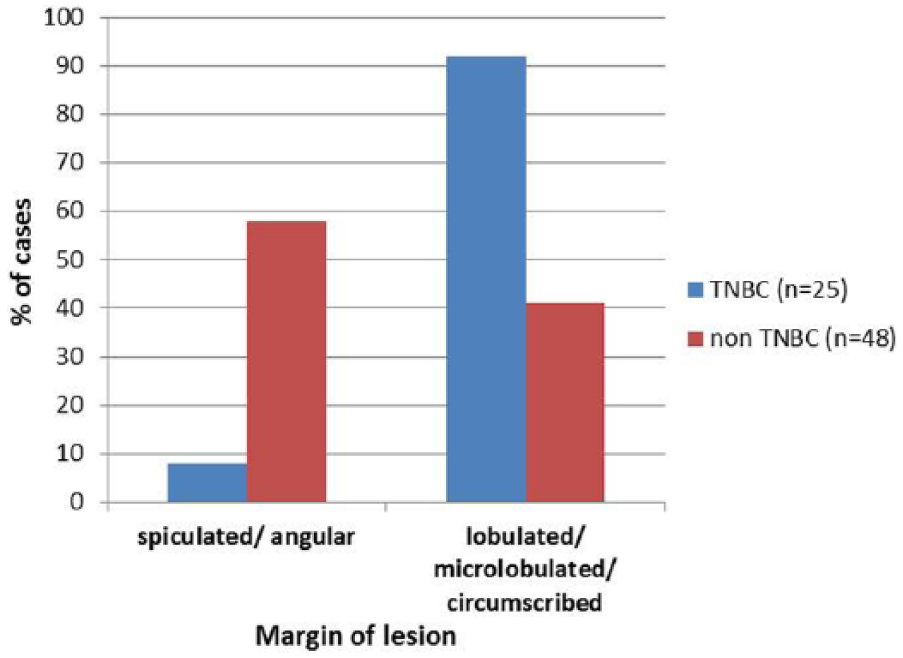
Bar graph showing the relationship of tumor margin on sonography and receptor status. TNBC, triple-negative breast cancer.
The analysis of the posterior acoustic features revealed a highly significant association with receptor type. The presence of posterior acoustic enhancement was much higher in TNBC compared with non-TNBC cases (52.0% vs 8.3%, P < .0001). This parameter showed a high sensitivity and specificity for presence of TNBC status (76% and 82%, respectively; OR = 12) (Tables 2, 3).
Moreover, posterior shadowing was found to have a strong negative association with TNBC (8% TNBC vs 69% non-TNBC); only two patients with TNBC status revealed mild posterior shadowing. Although unchanged posterior acoustic features were more common in TNBC (28.0% vs 10.4%), combined posterior features were seen equally in the two groups (Table 3 and Figures 4, 5). Shadowing demonstrated 94% sensitivity for receptor-positive status (OR = 25, P = .012) (Tables 2, 4 and Figures 2, 3, 7).
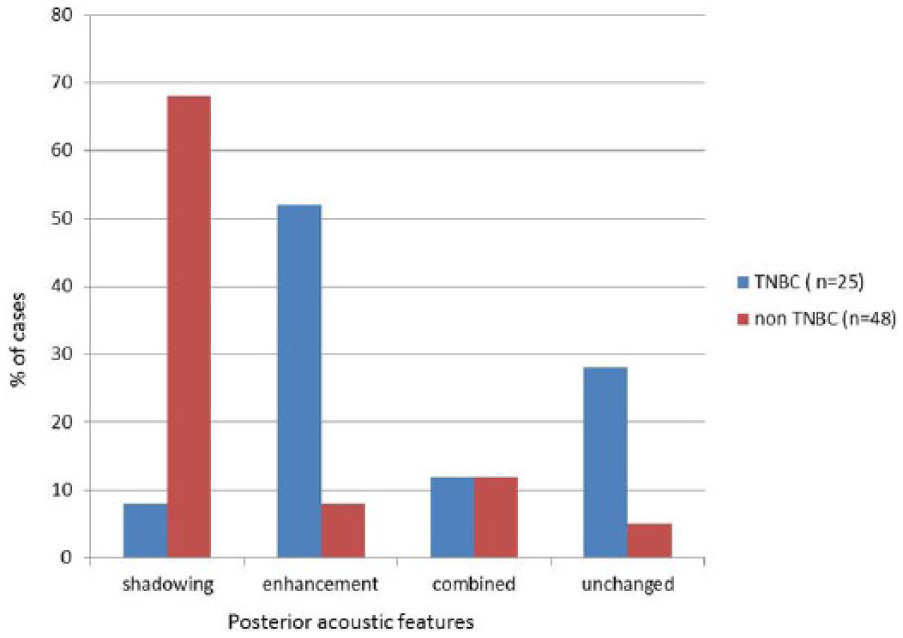
Pictorial depiction of the relationship between posterior sonographic features and receptor status. TNBC, triple-negative breast cancer.
Architectural distortions, described as an irregularity, loss of parenchymal pattern, and skin changes on the sonogram, were significantly different between both groups (P < .0001). Distortion was much more common in the non-TNBC group, seen in 57% cases, whereas only 12% of TNBC cases revealed the same. It was seen to be highly specific for non-TNBC status, although not very sensitive (Table 4 and Figures 2, 3, 8).
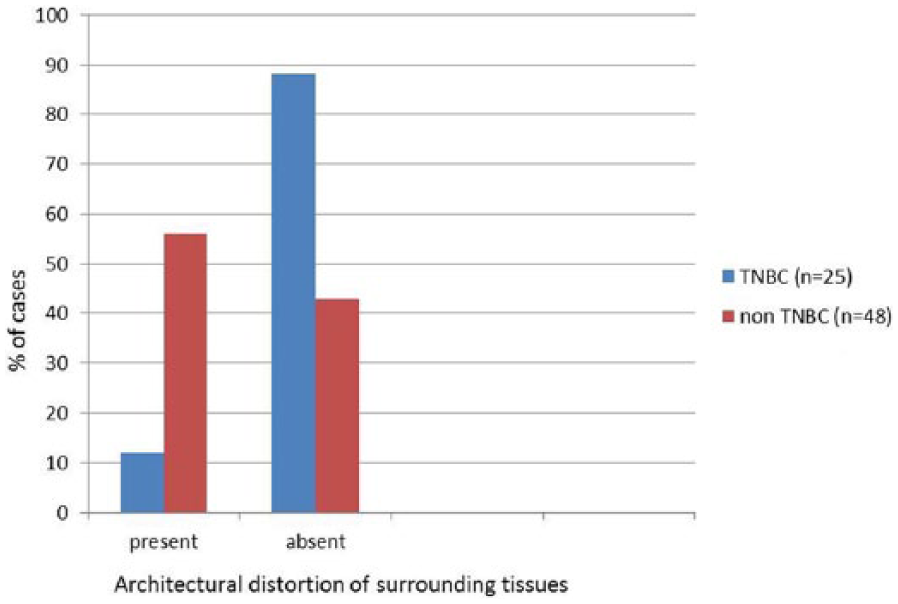
Bar graph depicting the status of architectural distortion in triple-negative breast cancer (TNBC) cases versus non-TNBC cases.
Furthermore, Cooper’s ligament distortion was almost exclusively seen in non-TNBC cases (39.5%) and in none of the TNBC cases in this study, thus revealing 100% specificity for receptor positivity (Tables 2, 4 and Figures 2, 3). An echogenic halo was more common in TNBC (32.0%) than in non-TNBC (18.7%) cases. With regard to presence of microcalcification and axillary lymphadenopathy, both groups had similar patterns.
Triple-negative breast cancer lesions revealed a higher vascularity than non-TNBC (P = .020). In the majority of TNBC cases, 60% were hypovascular (having flow in 20%-50% of lesion) and 8% were hypervascular (> 50% mass showing vascularity), whereas most non-TNBC had spotty (< 20%) vascularity (Tables 2-4 and Figures 2-5).
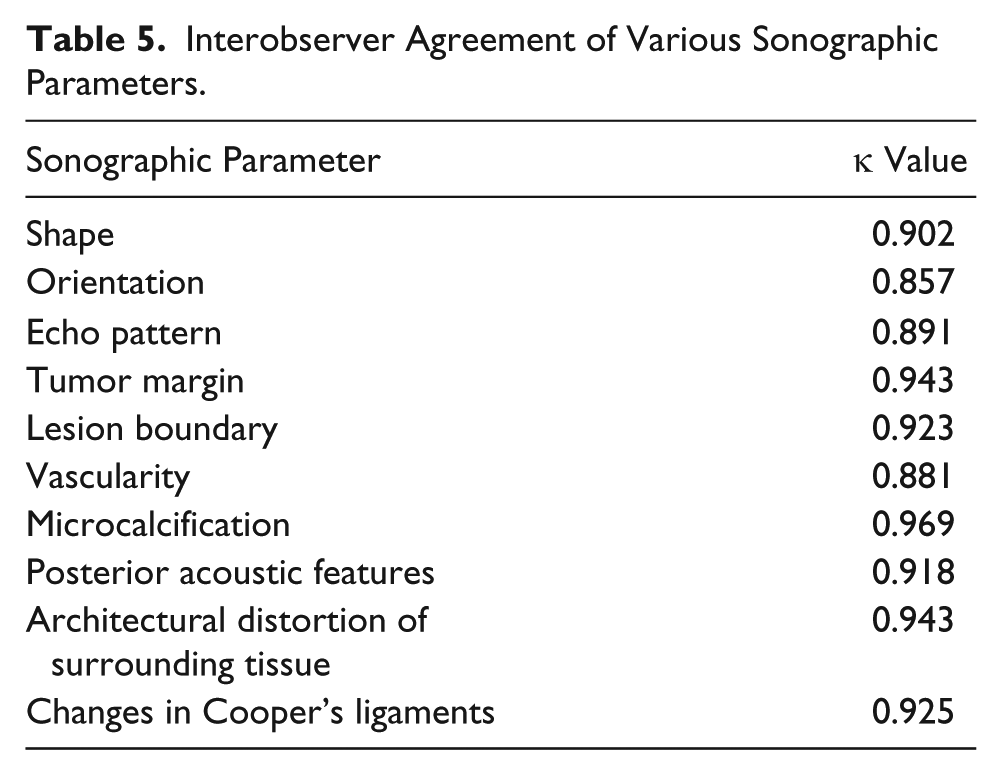
On applying logistic regression (multivariate analysis) for calculation of combined sensitivity and specificity, the three best parameters were margin of the tumor, posterior acoustic feature, and grade of the tumor for differentiation between TNBC and non-TNBC groups. The combined sensitivity was 84.0%, specificity 81.2%, PPV 82.0%, and NPV 79.0%. A ROC curve was plotted using the SPSS software; the area under the curve was 0.885 (95% confidence interval, 0.800-0.971), which seems to be excellent (Figure 9). Excellent interobserver agreement was seen for all parameters (κ > 0.75) (Table 5).
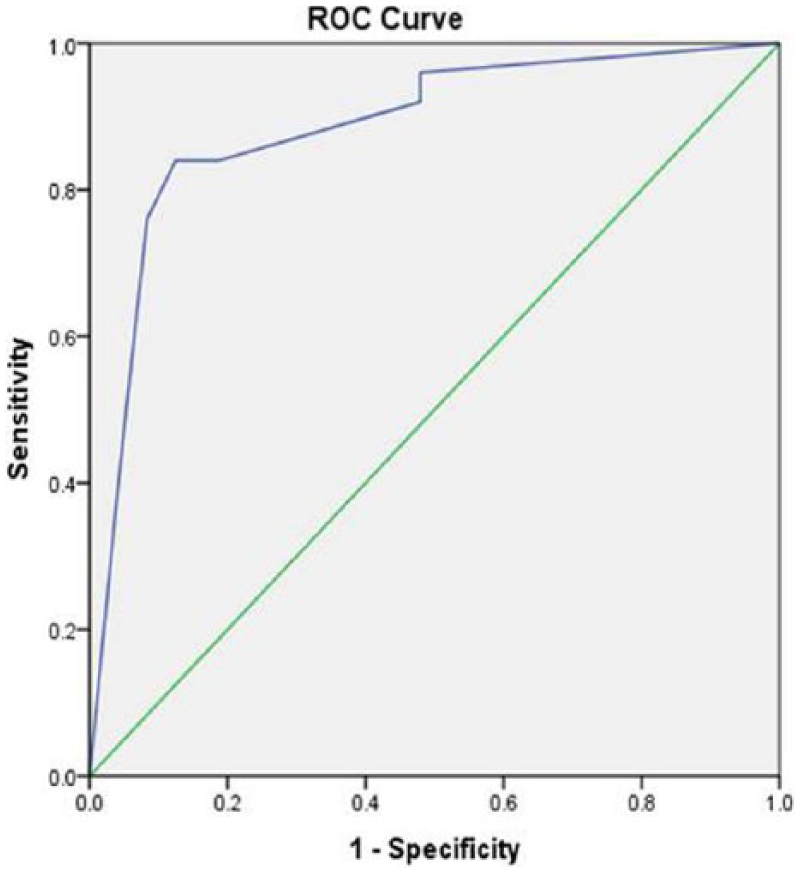
Receiver operating characteristics (ROC) for multivariate analysis for significant sonographic parameters (margin, posterior acoustic features) and tumor grade. Area = 0.885 (0.800-0.971).
Interobserver Agreement of Various Sonographic Parameters.
Discussion
Clinically, breast cancer is a molecularly heterogeneous disease that can be categorized into four distinct types: luminal A (ER/PR positive and HER2 negative) (30%-70%), luminal B subtype (ER/PR and HER2 positive) (10%-20%), HER2 type (ER/PR negative and HER2 positive) (5%-15%), and the basal-like subtype (15%-20%). The tumors of this basal-like breast cancer group frequently lack ER and PR and lack ERRB and HER2 over expression. These tumors are also called triple-negative tumors. Basal-like cancers, however, are not synonymous with TNBC, but often there is an overlap; also, both basal-like and TNBC show a strong association with the BRCA gene mutation.12,15,16
The TNBC subtype of breast cancer remains an extraordinary challenge for the oncologists/surgeons who treat these patients. Triple-negative breast cancer often occurs in younger women, who present with a larger tumor and are more likely to have distant visceral metastasis and an early relapse, making the overall outcome poor. To make matters worse, the endocrine treatment for ER/PR receptor-positive disease and HER2-directed treatment in cases of HER2 overexpression are ineffective for patients with TNBC; thus, chemotherapy remains the only viable option for these patients.12,16,17
It is important to identify these biological markers (ER, PR, HER2), as they can be applied for prognostication, for determining the most effective treatment strategy, and for prediction of clinical response to treatment. As in any other cancers, tumor grade on histology is also a prognostic factor for breast cancer. In the present study, the majority of TNBC cancers were high grade on histology, whereas most non-TNBC cancers were low grade, a finding similar to other studies.12, 15–17
This prospective study revealed strong correlations between sonographic parameters like posterior acoustic features, lesion margins, lesion vascularity, architectural distortion of surrounding tissues, Cooper’s ligament changes, histologic grade, and receptor status (TNBC vs non-TNBC). The shape, orientation, echo pattern of the tumor, and presence of microcalcification did not reveal any significant association with tumor type.
On applying logistic regression (multivariate analysis) for calculation of combined sensitivity and specificity, margin of the tumor, posterior acoustic features, and grade of the tumor emerged as the three best parameters for differentiation between TNBC and non-TNBC groups with a moderately high combined sensitivity and specificity. Most of the previous studies were retrospective and only a single study has prospectively used logistic regression models and reported that the efficiency of a single feature to estimate the molecular status was low and the efficiency substantially improved by combination of the ultrasound features. 16 Another study used the ensemble decision approach to identify the sonographic features of various molecular subtypes. 7
Triple-negative breast cancer cases were associated with larger tumor size at presentation in comparison with ER/PR positive cancers, a correlation reported by other authors.11, 15–17
A majority of lesions demonstrating posterior acoustic enhancement on sonography were found to have TNBC status on IHC in this study, which could make it an important sonographic parameter for identifying TNBC. The likelihood of having a TNBC receptor status in cases showing posterior enhancement was 12 times higher. On the other hand, presence of posterior shadowing was highly suggestive of a non-TNBC or receptor-positive status; lesions with posterior shadowing had 25 times higher likelihood of receptor positivity. This is in concurrence with the findings of Irshad et al., 8 who reported that tumors with posterior shadowing have greater than 9 times the odds of having ER positive status and tumors with posterior enhancement have greater than 8 times the odds of having at least one negative receptor. Other authors also reported similar trends, although the percentages were variable.11,12, 15–17
Margin contour was another important ultrasound criterion. In the present study, 92% of TNBC cases had circumscribed margins and only 8% had spiculated margins. The likelihood of having TNBC status was 16 times higher if the lesion had circumscribed margins on sonography. Irshad et al. 8 reported a likelihood of 5.21 with circumscribed margins. This parameter, however, had a high sensitivity for TNBC status; the specificity was moderate. On the other hand, presence of spiculated angular margins was highly specific for non-TNBC status. Of the lesions with spiculated margins, 93% had positive receptor status. The likelihood of having a receptor-positive status was 21 times higher with spiculated margins on the sonogram. These results comply with previous retrospective studies where circumscribed margins had been reported to have a high likelihood of being associated with TNBC cases and the presence of spiculated margins increased the likelihood of non-TNBC cases.11, 12, 15–17
Overall, the vascularity was found to be higher in lesions having TNBC status in comparison with non-TNBC lesions. Most of the non-TNBC lesions showed vascularity of less than 20% of the lesion, whereas the majority of TNBC cases had vascularity involving 20% to 50% of the lesion. In a solitary study on this parameter, 10 in 88 triple receptor negative (TRN) cases assessed, hypovascularity was reported to be more common (41%). It is possibly a limitation of our study that the vascularity was assessed on color Doppler, and not power Doppler or with contrast-enhanced sonogram, and also that the evaluation was done subjectively without using any objective tools. This is an area that deserves further research.
Lesions demonstrating architectural distortion of surrounding tissues on sonograms were found to have 9.5 times higher likelihood of having a positive receptor status. This parameter, thus, was highly specific for non-TNBC status, with a high PPV and NPV, but had a moderate sensitivity. Similarly, Cooper’s ligament changes were seen almost exclusively in non-TNBC cases and revealed a 100% specificity and PPV for non-TNBC status. In comparison, Wojcinski et al. 15 and Choi et al. 11 reported nonsignificant differences in architectural distortion in the two subgroups. However, they found significant differences in Cooper’s ligament changes between these groups. Cooper’s ligament displacement was more often seen than disruption in the TNBC group. These variations might be due to the high subjectivity in evaluation of these parameters.
The possible explanation for differences in sonographic parameters between the receptor groups is hypothesized that since TNBC lesions more commonly are high grade, are more cellular, and grow rapidly, they get less time to incite a desmoplastic reaction. They often present more commonly as a large, soft, and cystic/profoundly hypoechoic mass with circumscribed margins, posterior enhancement, higher vascularity, and less architectural distortion and Cooper’s ligament disruption. On the other hand, non-TNBC lesions are lower grade, grow less rapidly, are less cellular, and thus incite a desmoplastic reaction, thus appearing as a hard lump, with hypoechoic to isoechoic echo pattern, posterior acoustic shadowing, and spiculated margins, causing architectural distortion of surrounding tissue and Cooper’s ligament disruption.
The findings of this study could have practical implications for community health. Receptor status detection is done worldwide using IHC and other sophisticated laboratory tests; these invasive tests can cause patient discomfort and postprocedure complications. Breast sonography, being noninvasive, has a distinct advantage. Furthermore, although these tests are readily available in developed nations, in many countries, they are neither readily available nor affordable to most of the population. On the other hand, sonography is a relatively inexpensive modality with wide availability. Knowing the predictive value of various sonographic parameters can help radiologists noninvasively triage patients into likely receptor-positive and triple-negative tumors. The likely receptor-positive cases could be started empirically on hormone therapy; on the other hand, likely triple-negative cases, which are much more aggressive, could be selectively referred to higher centers for receptor testing and more aggressive management and chemotherapy. This could help in early detection of aggressive triple-negative tumors and in judicious use of available resources.
The limitations for this prospective study include a relatively small convenience sample of patients and lack of a control group. Also, it was conducted at a tertiary care hospital that caters to mainly lower and middle socioeconomic strata of an urban population, which is a subset of the general population. Larger, multicenter studies that replicate this work are needed to corroborate these results.
Conclusion
Breast sonography using multiple parameters, in isolation and in combination, was found to have a high predictive value for noninvasively predicting the receptor status in breast cancer and in identifying the triple-negative cases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.