
Abstract
Objective
The average 5-year survival rate of breast cancer (BC) patients has been significantly prolonged with new therapeutic methods. However, their effects on BC patient long-term survival rates are unclear. Therefore, this study aimed to analyze the specific clinical factors that can affect BC long-term survival.
Methods
Here, we conducted a retrospective study and analyzed long-term survival using data of 3,240 BC patients from 1977 to 2005 from the Genotype-Tissue Expression (GTEx) database using the Kaplan–Meier method.
Results
Breast tumor size and stage were negatively correlated with long-term survival, but age showed no significant correlation. Estrogen receptor (ER) and progesterone receptor (PR) expression were each positively correlated with patient survival time, while ERBB2 receptor (HER2) expression was negatively correlated with survival time. Patients with high Nottingham prognostic index (NPI) values did not benefit from available therapies. Furthermore, breast-conserving surgery is more conducive to BC patient long-term survival than mastectomy.
Conclusions
Early detection and breast-conserving surgery may support long-term survival for BC patients. Elevated expression of ER and PR were both associated with longer patient survival time, while positive expression of HER2 showed the opposite trend. The long-term survival rates of patients with high NPI values can potentially be increased.
Keywords
Introduction
Breast cancer (BC) is the most common cancer in women worldwide and the second leading cause of cancer-related death.1,2 In 2018, approximately 266,120 new BC cases were reported in the United States, along with 40,920 deaths.3,4 On average, BC treatment is very costly, with the mean monthly total health care costs per BC patient estimated to be $4421. 5 The average cost per patient is more than $85,000 in the United States, resulting in a heavy financial burden. 6 In recent decades, significant progress has been made with BC treatment methods, leading to a greatly improved 5-year survival rate.7–10 However, more work is necessary to increase survival rates to those of some other cancers. For example, the 10-year survival rate of prostate cancer patients is about 90%, while that of BC patients is still less than 60%.11–13 Therefore, this disease is worthy of further in-depth study.
An important indicator for studying the efficacy of cancer treatment is the 5-year survival rate. With improved medical standards, the survival time of cancer patients has been greatly extended. 14 In the United States, the 5-year survival rate of BC patients has increased from 60% to the current 90%. 15 However, the impact of BC is long-term. A large number of patients have a high probability of relapse after five years, and some patients will relapse even after 15 years of treatment.16–18 Therefore, it is very important to study the relevant indicators that affect the survival of BC patients for 20 years or longer. However, there are still few studies in this area.
Various prognostic indicators are associated with cancer patients, including tumor size, tumor stage, and tumor grade. The histological stratification of BC is mainly based on the expression status of the estrogen receptor (ER), progesterone receptor (PR), and ERBB2 receptor (HER2), 19 which has laid the foundation for BC classification. Previous studies have shown that these indicators have important guiding significance for determining BC prognosis.20,21 The Nottingham prognostic index (NPI) combined with BC tumor size, stage, and metastasis status may potentially be useful for predicting prognosis.22–25 We speculate that these factors are strongly related to long-term survival, and their impact deserves further study.
Methods
Data collection
The research data from a Nature article published last year were collected from BC patients from 1977 to 2005 (https://www.gtexportal.org/home/). 26 The patients were from the UK and Canada and were continuously tracked until 2015 (nearly 40 years). The study included patients with a confirmed positive histopathological diagnosis, but excluded those who had no follow-up. For all enrolled individuals, information was retrieved on age, the expression status of ER, PR, and HER2, NPI, and if breast-conserving surgery was performed. We obtained permission from the Genotype-Tissue Expression (GTEx) database to access and use the data. Our institution waived the need for ethics approval of these retrospectively obtained and anonymized data for this non-interventional study, so informed consent was not sought from the patients. All patient details were removed to follow protocols throughout the process and protect patient privacy. The reporting of this study conforms to STROBE guidelines. 27
Patient survival analysis
Survival curves were generated using the Kaplan–Meier method, then compared using log-rank tests to explore the associations between the expression levels of genes of interest and patient prognosis. All prognostic analyses were conducted using the R survival package.
Statistical analysis
All statistical analyses were performed using GraphPad Prism 6 (GraphPad Software Inc., San Diego, CA, USA) and R programming language (version 3.5.0). P-values <0.05 were considered statistically significant.
Results
Effects of age, tumor size, and stage on BC patient long-term survival
Data were collected from 3240 BC patients included in the GTEx database. To study the factors affecting the long-term survival of BC patients, we analyzed the impact of different clinical data on survival rates. As shown in Figure 1a, there was no significant difference in survival time for BC patients of different ages. Notably, patients under 55 years of age tended to have lower 10-year survival rates than those 55 years of age and older, although the difference was not statistically significant. Tumor size had an important impact on the patient survival rates (P < 2 × 10−16; Figure 1b). Patients with tumors smaller than 2 cm showed a 30% higher survival rate than those with tumors larger than 5 cm (Figure 1b). Similarly, tumor grade and stage had significant effects on long-term survival (P = 2 × 10−6 and P < 2 × 10−16, respectively; Figure 1c and 1d).
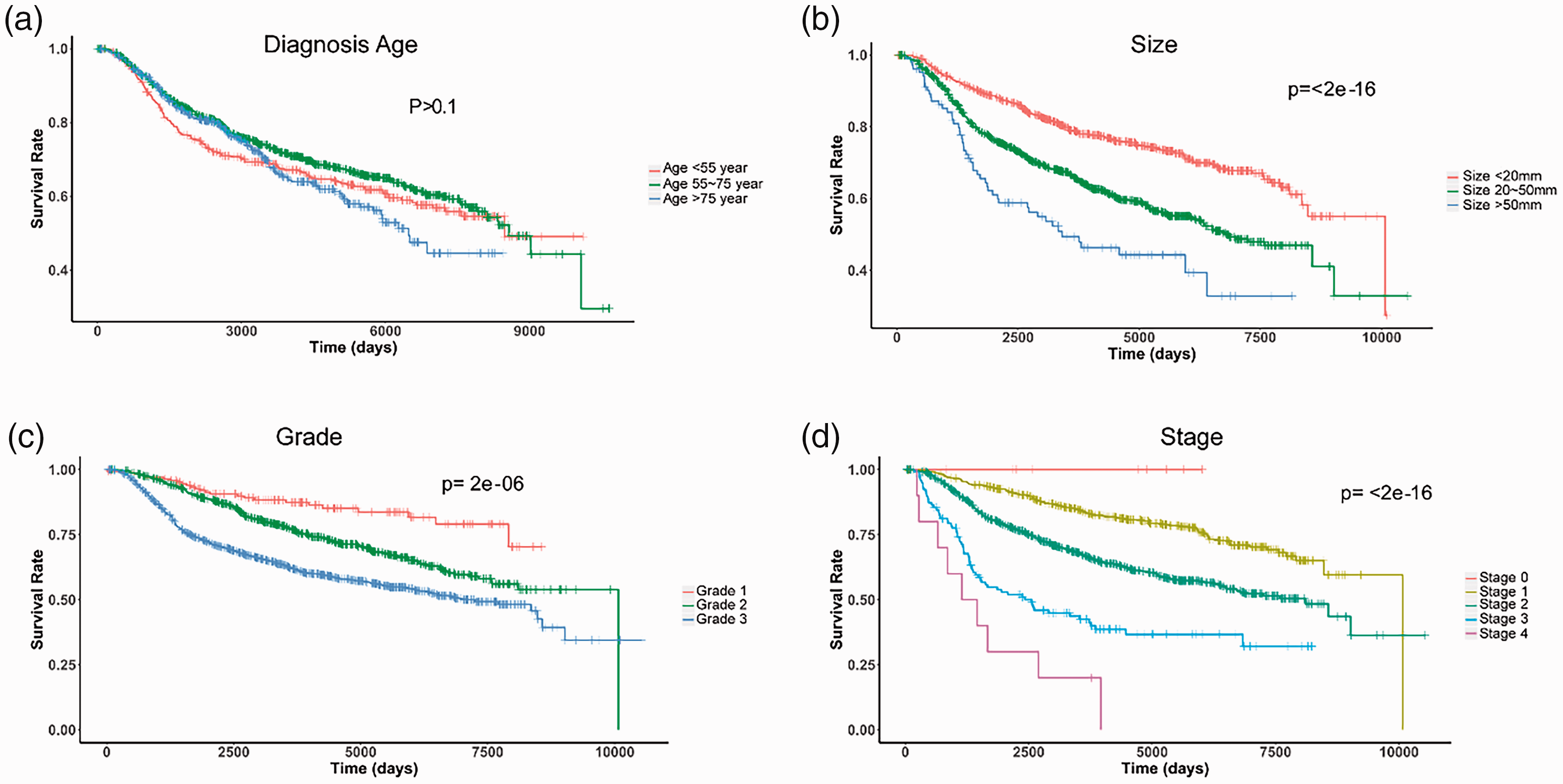
Effects of clinical characteristics on the long-term survival of breast cancer (BC) patients. Overall survival curves of BC patients with different diagnosis (a) age, (b) tumor size, (c) tumor grade, and (d) tumor stage.
Effect of ER, PR, or HER2 expression status on BC patient long-term survival
Because ER, PR, and HER2 expression status is part of the most commonly used BC classification method, we examined the impact of these three markers on the long-term survival of patients in this study. The results showed that all three markers were significantly correlated with long-term survival (P < 0.05; Figure 2). ER- and PR-positive patients had higher long-term survival rates than patients negative for these markers (P = 0.03 and P = 9 × 10−5, respectively; Figure 2a and 2b). In contrast, HER2-positive patients had lower long-term survival rates than HER2-negative patients (P = 9 × 10−6; Figure 2c).

Effects of ER, PR, and HER2 expression levels on the long-term survival of breast cancer (BC) patients. Survival ratios of BC patients with different (a) ER, (b) PR, and (c) HER2 expression levels.
The NPI is a good indicator of BC patient long-term survival
The NPI is an important indicator of BC patient prognosis. We analyzed the effect of the NPI on the long-term survival of BC patients diagnosed at different time periods. As shown in Figure 3, the NPI value was generally positively correlated with the survival rate of patients. Interestingly, in patients diagnosed with BC before 1985, the long-term survival rates (>20 years) of patients with different NPI values were not significantly different (Figure 3a). However, in patients diagnosed after 1985, the survival time of two groups of patients with NPI values <5.4 continued to improve, indicating that the overall survival curve continued to move upward (P < 2 × 10−16; Figure 3b and 3c). However, the overall change in the NPI value >5.4 group was not clear, and the gap between the three curves is large (Figure 3b and 3c).

Effects of Nottingham prognostic index (NPI) scores on the long-term survival of breast cancer (BC) patients. Overall survival curves of BC patients with different NPI scores (a) before 1985, (b) from 1985 to 1995, and (c) after 1995.
Patients with NPI < 5.4 benefit more from improved BC treatments
To further quantify the effect of different NPI values on BC patients, we measured the changes in 5-year survival, 10-year survival, and 15-year survival rates in three different time periods. The results suggest that patients with an NPI value <3.4 have had continuously improved 5-year, 10-year, and 15-year survival rates between 1985 and 1995, and their 10-year and 15-year survival rates are still increasing substantially (Figure 4a). Similar results were observed in the NPI 3.4 to 5.4 group (Figure 4b). From 1985 to 1995, their 5-year, 10-year, and 15-year survival rates have significantly improved. Surprisingly, the survival rates of patients with an NPI value >5.4 showed a downward trend (Figure 4c). These results suggest that in the past few decades, patients with lower NPI values have benefited more from improved treatment methods.

Effects of Nottingham prognostic index (NPI) scores on 5-year, 10-year, and 15-year breast cancer (BC) patient survival rates. Overall 5-year, 10-year, and 15-year survival curves of BC patients with (a) NPI < 3.4, (b) NPI 3.4–5.4, and (c) NPI > 5.4 in different age groups.
Breast-conserving surgery is more conducive to BC patient long-term survival
We next examined the effect of surgery on the long-term survival of BC patients. The results showed that the survival time of patients who underwent breast-conserving surgery was significantly longer than that of patients who had a mastectomy procedure (P = 1 × 10−13; Figure 5a). Because most BC patients undergoing breast-conserving surgery may have early-stage disease and total resection is possibly mainly performed in advanced patients, we analyzed the impact of surgery on the long-term survival of patients with different tumor stages. The results showed that the long-term survival rate of stage 2 patients with breast-conserving surgery was significantly higher than that of patients who had a mastectomy (P = 3 × 10−5; Figure 5c). Similarly, stage 0–1 and stage 3–4 patients with breast-conserving surgery tended to have higher long-term survival rates than patients with mastectomy, but these results were not statistically significant (Figure 5b and 5d). These findings suggest that BC patients undergoing breast-conserving surgery generally have a higher long-term survival rate than mastectomy patients.
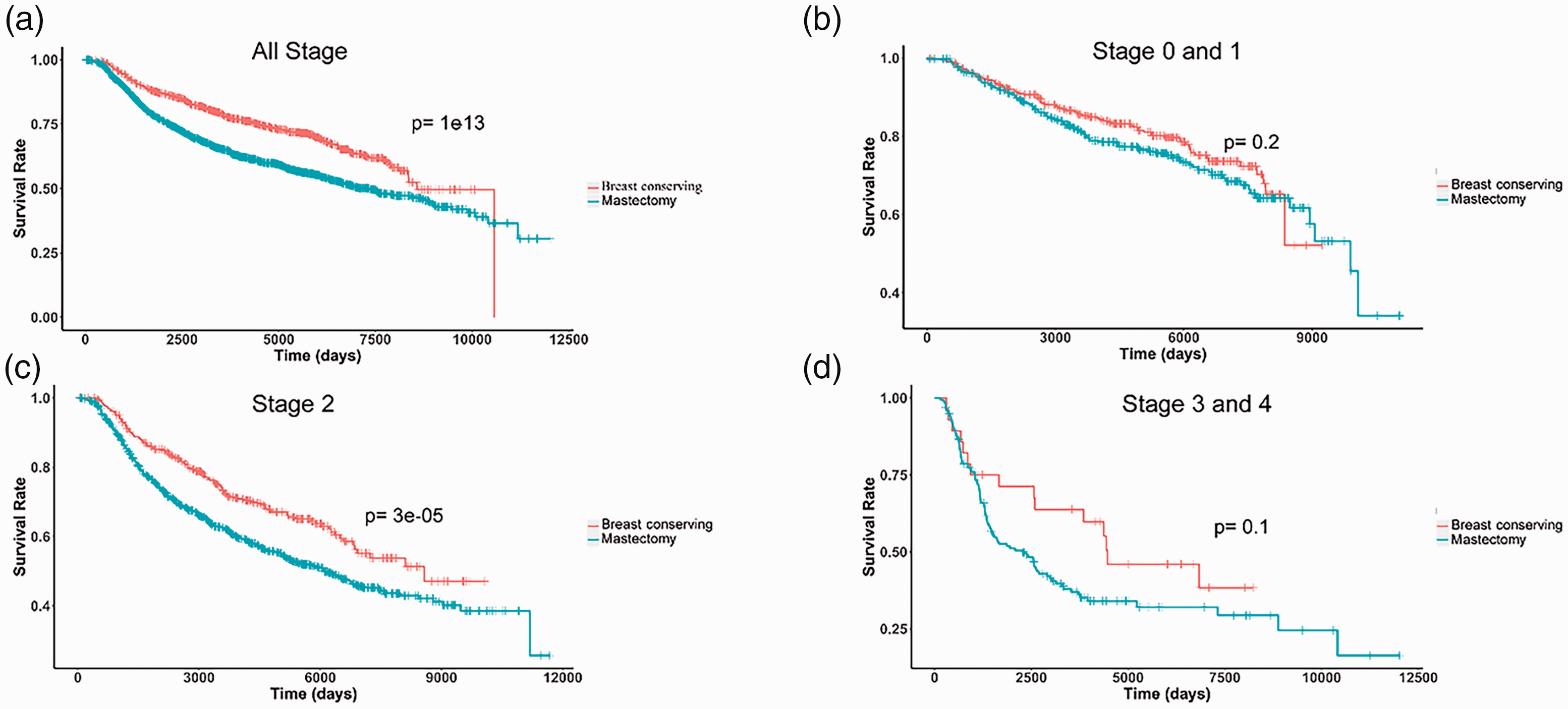
Effects of therapy with or without breast-conserving surgery on the long-term survival of breast cancer (BC) patients. The long-term survival curves of BC patients who underwent breast-conserving surgery or mastectomy with (a) all tumor stages, (b) tumor stages 0–1, (c) tumor stage 2, and (d) tumor stages 3–4.
Discussion
BC is one of the most serious tumors threatening women’s health. The NPI is one of the most important of numerous indicators that can affect BC recovery.22–24 In this study, we found that the NPI indicator values are constantly changing as technology advances. In recent years, its effect has become increasingly significant. The characteristics of such indicators will also likely change continuously with further in-depth BC research. For example, EGFR-mutated lung cancer tumors frequently metastasized, leading to poor patient prognosis. However, after the approval of small molecule inhibitors targeting EGFR, prognosis has considerably improved for patients treated with these methods.28–31 Similarly, BRCA-mutated ovarian cancer previously had a lack effective treatments, but these patients have now achieved a good prognosis with the help of targeted therapy.32–35 In the future, the development of precision medicine methods, like certain immunotherapies, may be extremely beneficial for many cancer patients.36,37
We also observed that in recent decades, the survival rates of BC patients with high NPI values did not improve, but rather decreased. There are several possibilities for this unexpected finding. For such patients, the method adopted in the early 21st century may not have improved much even by the 1980s, making it difficult to obtain better results. Additionally, the environment and dietary structure have changed for decades, leading to a generally worse prognosis for cancer patients. A third possibility is that with the progression of tumor screening methods and diagnostic technology in recent years, more tumors are being diagnosed as advanced and malignant, resulting in lower patient survival rates. The exact reasons for our results require further analysis. Because the long-term survival rate of BC patients with high NPI values is currently low, there is great potential for improvement. Therefore, our future research will focus on improving treatment effects in these patients.
Age is a relevant factor that can affect cancer survival.38–40 However, our study suggests that youth is not necessarily a favorable factor for long-term BC survival. Our data show that even younger patients had worse survival rates within 10 years of tumor diagnosis. The survival rate of the oldest group began to decline rapidly 12 years after tumor diagnosis. We hypothesize that the high mortality rate in young people may be from the strong cell viability and proliferation ability, which can lead to rapid tumor progression and recurrence. Differences between tumors in this regard are also worthy of in-depth investigation.
In this study, we used a large sample size and long follow-up period to reveal the factors affecting the long-term survival of BC patients. This work may provide a more reliable theoretical supplement for future BC research. There are some limitations to our study. First, some subjectivity is inevitable because this was a retrospective study. Second, as a result of extensive research and investment over the past two decades, there have been many new developments in BC treatment methods. BC molecular subtype is one of the most critical factors affecting the long-term survival of patients. BC subtypes have direct effects on the pathological complete response. 41 However, the molecular subtype data in this study could not be presented because the older patient data from between 1977 and 2005 did not include information on molecular subtypes. In future research, the molecular subtypes should also be given more attention.
Conclusions
Among the clinical factors potentially affecting BC patients, our data suggested that age was not significantly correlated with long-term survival. However, breast tumor size and stage may be negatively correlated with long-term survival. In addition, we found that patients with high NPI values do not show benefit from the currently available therapies. Furthermore, we showed that breast-conserving surgery is more conducive to BC patient long-term survival. Early detection and breast-conserving surgery may increase the likelihood of long-term survival. When the expression levels of ER and PR are elevated, patient survival time may be longer, while positive expression of HER2 showed the opposite trend. There is also a strong potential to increase the long-term survival rates of patients with high NPI values.
Footnotes
Author contributions
YFL and DSL conceived and designed the study. YHL and XYW managed online data collection, analyzed the data, and drafted the manuscript. JWS, LLM, KH, and CPW managed online data collection. All authors approved the final version of the manuscript.
Data availability statement
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants through the clinical discipline project of Shanghai Pudong (No. PWYgy2018-03 and PWZzk2017-31).