
Abstract
Intrahepatic portosystemic venous shunts with associated aneurysms are extremely rare anomalous communications between intrahepatic portal veins and systemic veins through intrahepatic venous channels. Intrahepatic portosystemic venous shunts are usually asymptomatic but can be the cause of hepatic encephalopathy and hypoglycemia, especially when a high degree of shunting exists. The sonographic incidental finding of an aneurysmal vascular connection between the left portal vein and left hepatic vein as diagnosed by sonography is presented and discussed. When evaluating patients with suspected symptoms of hepatobiliary disease, sonographers and radiologists should carefully scan and meticulously assess the liver for signs of abnormal venous communications.
Introduction
Intrahepatic portosystemic venous shunts with associated aneurysms are exceptionally rare disorders characterized by abnormal communications between branches of the portal veins and systemic veins.1–5 Intrahepatic portosystemic venous shunts were first reported by Doehner et al. 6 in 1959 and later described by Raskin et al. 7 in 1964.
Accurate evaluation and classification of intrahepatic portosystemic venous shunts can be accomplished with sonography. A case of an asymptomatic, incidental, and congenital intrahepatic portosystemic venous shunt with an abnormal aneurysmal communication between the left portal vein and left hepatic vein and its sonographic features is presented in this case study.
Case Report
A morbidly obese 43-year-old man presented to the emergency department with an acute onset of excruciating lower back and abdominal pain. His medical history was remarkable for B-cell lymphocytic leukemia, thrombocytopenia, arthritis, smoking, and diabetes. Physical examination on admission was unremarkable except for abdominal tenderness. The patient denied any trauma, surgery, or biopsy. The patient was referred for a sonographic examination to rule out cholelithiasis.
Sonographic examination of the abdomen using a C5-2 curved linear array transducer (GE Logic 9; GE Healthcare, Waukesha, WI) revealed multiple, mobile gallstones without gallbladder wall thickening, diffuse fatty infiltration of the liver, and hepatomegaly. The gray-scale sonographic examination revealed a 1.1 × 0.9 × 0.8 cm anechoic, round cystic structure connected to branches of the left portal vein and left hepatic vein in the left lobe of the liver (Figure 1). Color and power Doppler sonography demonstrated flow in these structures (Figure 2). On Duplex sonography, the aneurysmal shunt between the portal vein and hepatic vein branches demonstrated a low-velocity helical flow (Figure 3). The involved left portal vein branch demonstrated a normal-velocity flow with cardiac modulation of the spectrum (Figure 4). In addition, the left hepatic vein demonstrated turbulent flow in a short segment adjacent to the aneurysm (Figure 5). These sonographic findings were consistent with an aneurysmal intrahepatic portal venous shunt.
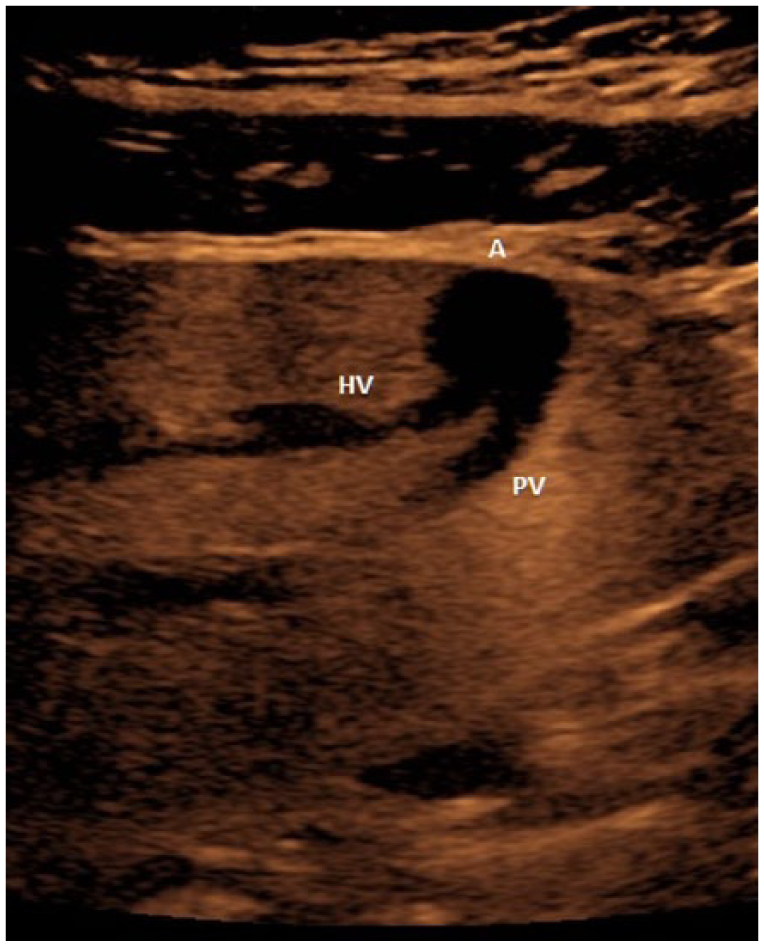
Longitudinal sonogram of the left lobe of the liver demonstrating the aneurysm appearing as an anechoic, round cystic structure (A) connecting the left portal vein branch (PV) and the left hepatic vein branch (HV).
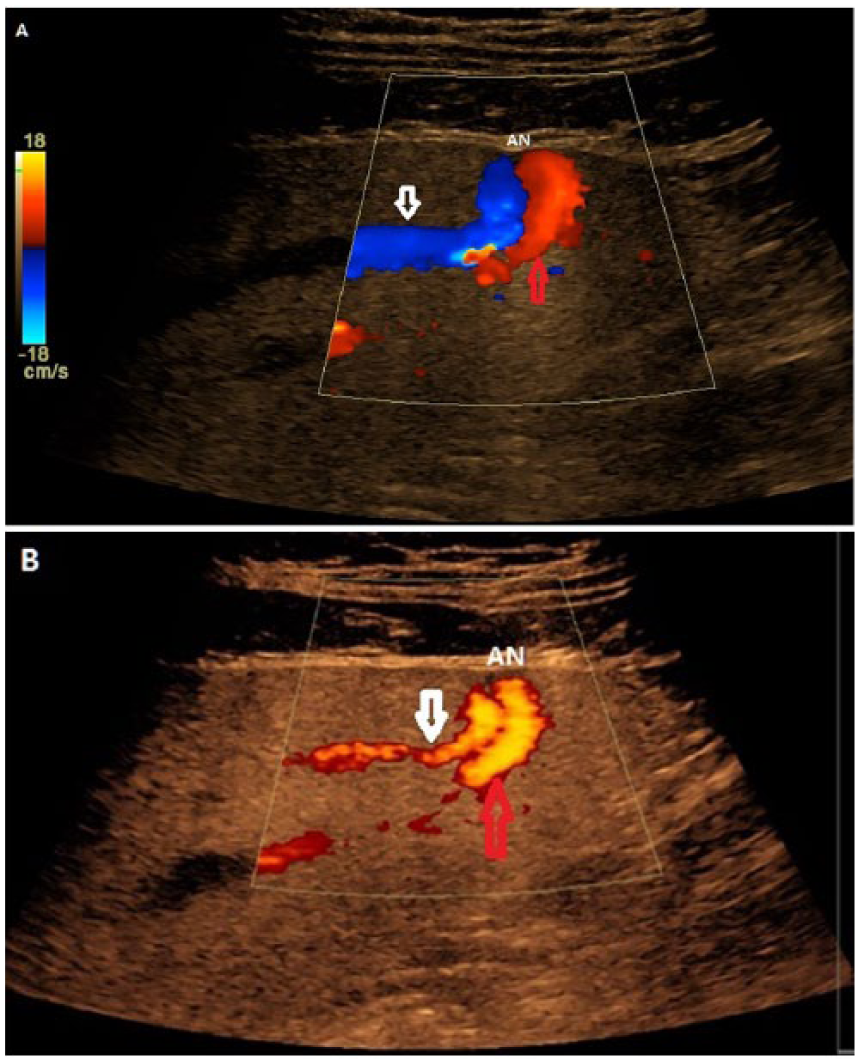
Longitudinal color (A) and power (B) Doppler images of the left lobe of the liver demonstrate vascularity (flow) within the connecting aneurysm (AN), the left portal vein branch (red arrow), and the hepatic vein branch (white arrow).
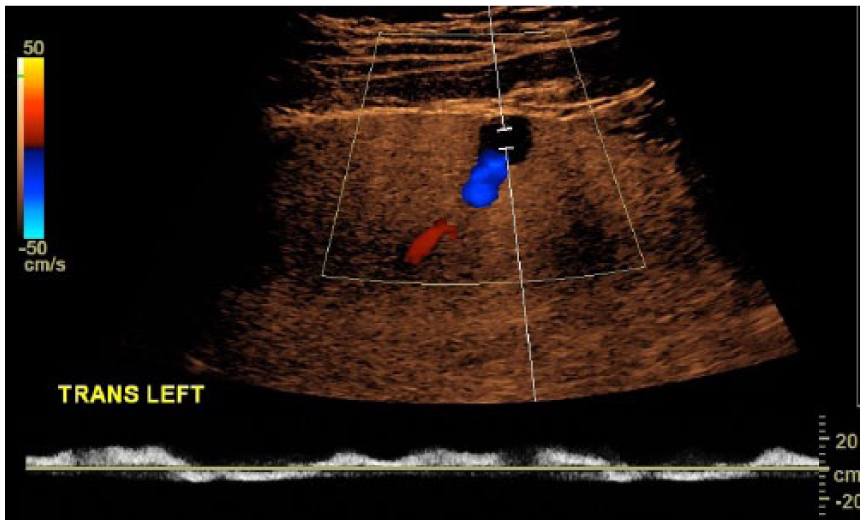
Transverse spectral Doppler image of the connecting aneurysm demonstrates a low-velocity, helical waveform within it.
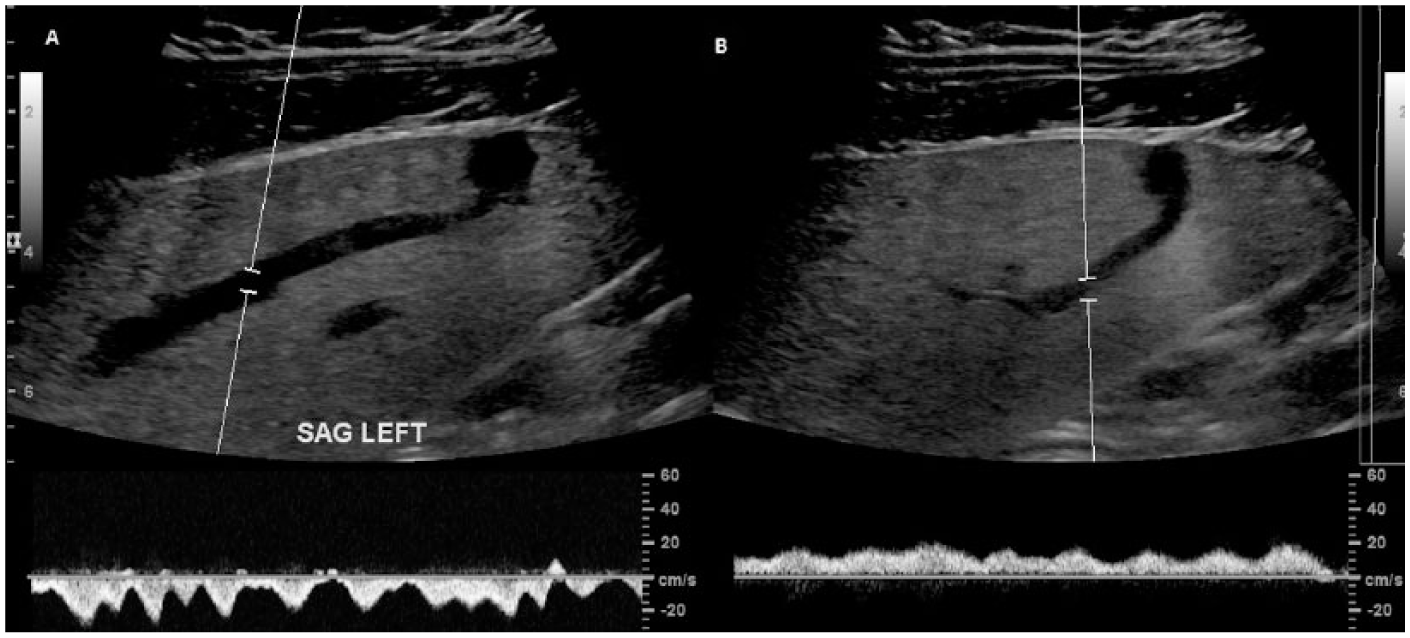
Longitudinal spectral Doppler images demonstrate (A) a “multiphasic” waveform in the left hepatic vein branch and (B) a slightly pulsatile waveform in the left portal vein branch due to the transmission of cardiac motions from the hepatic vein to the portal vein through the shunt.
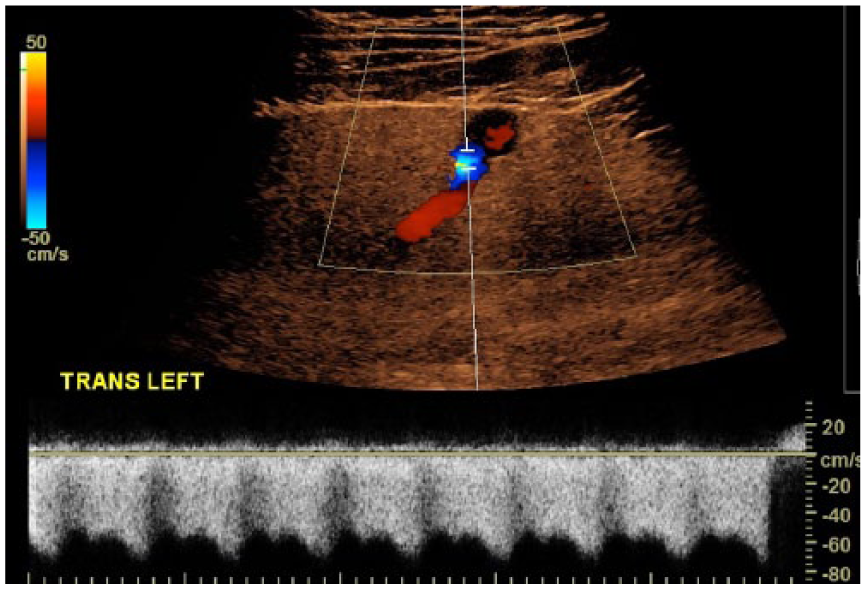
Transverse color and spectral Doppler image shows a high-velocity, turbulent flow in the left hepatic vein branch near the connecting aneurysm.
A computed tomography examination of the abdomen confirmed the sonographic findings. Due to the lack of trauma, surgery, or biopsy, this finding was assumed to be congenital and no treatment or intervention was indicated at the time of the diagnosis.
Discussion
Intrahepatic portosystemic venous shunts are rare vascular abnormalities that are characterized by an anomalous communication between the intrahepatic portal vein and systemic venous system through an intrahepatic venous channel.1–5,8 To the best of our knowledge, fewer than 50 cases have been reported in the world literature.5–7,9–18
Extrahepatic portal venous aneurysms have been described in the literature.19–23 However, peripheral intrahepatic portosystemic venous shunts with aneurysms are extremely rare1–5,13,24 and incidentally discovered.2,13 In a study of nine cases involving intrahepatic portosystemic venous shunts, De Gaetano et al. 4 found that 56% of the cases, without any clinical evidence of liver disease, were incidentally discovered. Moreover, it has been reported that the duration from the formation of the shunt to its diagnostic recognition can range from hours to years.5,25
The exact nature or embryogenesis of this abnormality is controversial. 26 Some researchers consider intrahepatic portosystemic venous shunts to represent a rare congenital anomaly that results from either persistent vitelline veins or a variety of persistent sinus venosus.5,26 Others believe them to be iatrogenic, posttraumatic, or a result of portal hypertension associated with cirrhotic livers or hepatic infections.15,17,26–28 In this particular case, it is likely to be congenital as there was no associated evidence of chronic liver disease or any history of liver trauma. Furthermore, other authors have postulated that the rupture of a portal vein aneurysm into the hepatic vein is the cause.4,28–31
Since intrahepatic portosystemic venous shunts were first described in the literature in 1959 by Doehner et al., 6 many systems have been developed to categorize intrahepatic portosystemic venous shunts—first by Park et al. 27 and later by Chevallier et al. 3 Park et al. 27 categorized intrahepatic portosystemic shunts into four different morphologic types: Type I, the most common, involves a single tube with a constant diameter connecting the right portal vein to the inferior vena cava, including patent paraumbilical veins; Type II involves a localized peripheral shunt in which a single communication or multiple communications between peripheral branches of portal and hepatic veins in one hepatic segment are present; Type III, the rarest, involves an aneurysmal communication between a peripheral portal and a hepatic vein; and Type IV, although similar to Type III, involves diffuse and multiple communications between peripheral portal and hepatic veins in several hepatic segments or lobes.
By comparison, Chevallier et al. 3 classified intrahepatic portosystemic venous shunts into four categories based on their clinical and anatomic features: Type I includes paraumbilical veins, such as those encountered in portal hypertension; Type II involves a connection between a portal branch and hepatic vein in adjacent liver segments; Type III comprises portal and hepatic vein connections between nonadjacent liver segments; and Type IV includes any connection between the right portal branch and inferior vena cava. In the case presented, the findings were consistent with the Type III shunt per Park et al. 27 and the Type II shunt per Chevallier et al. 3
The clinical significance of intrahepatic portosystemic venous shunts is a matter of differing opinions. Some researchers have reported the potential for development of hepatic encephalopathy.2,4,7,27,28,32–39 Uchino et al. 40 reported 12 of 51 cases having hepatic encephalopathy at the time of diagnosis. Others suggested that the prognosis and rate of hepatic encephalopathy are associated with shunt size and age.5,41 It has been reported that the rate of hepatic encephalopathy increases with age due to the decrease in tolerance of the brain to toxic metabolites, and this may explain the delayed clinical manifestations.7,32,41,42 In addition, large intrahepatic portosystemic venous shunts have been believed to be more responsible for hepatic encephalopathy than smaller ones due to the higher degree of shunting. 43
Furthermore, some authors have reported that intrahepatic portosystemic venous shunts increase the risk of health complications such as hyperinsulinism with secondary hypoglycemia resulting from the liver’s inability to degrade glucose, hepatic fibrosis due to long-standing diversion of portal flow away from the liver sinusoids, and pulmonary hypertension.5,15,17,29,32,33,44
The use of imaging modalities such as sonography has enhanced the diagnosis of intrahepatic portosystemic venous shunts.1,4,17,25,27,45 Gray-scale sonography demonstrates anechoic or tubular structures with or without an aneurysm communicating between branches of portal and hepatic veins, consistent with one of the morphologic types of intrahepatic portosystemic venous shunts described by Park et al. 27 and as seen with previous reports of intrahepatic portosystemic venous shunts.1–5,13
Color Doppler sonography can further identify the presence of the intrahepatic portosystemic venous shunt, the type, and the direction of flow in the identified vessels, which can be essential for proper diagnosis and follow-up therapy, if needed.46–48 De Gaetano et al. 4 have reported low velocity, bidirectional, or helical flow in the aneurysm on Doppler sonography. In our case, Doppler sonography has demonstrated similar findings.
Furthermore, many of the spectral Doppler findings that have been documented and reported with intrahepatic portosystemic venous shunts include biphasic waveform patterns in the hepatic vein branch and monophasic to pulsatile waveforms in the portal vein branch by which the pulsatile waveform patterns are believed to be caused by the cardiac oscillations transmitted from the hepatic vein to the portal vein branches.4,5,13,25,26,31,42,49,50
Other Doppler sonographic findings such as shunt ratios (total blood flow volume in the shunt divided by the total blood flow in the portal vein) of greater than 60% have been reported and associated with an increased risk of hepatic encephalopathy and can be indicative for corrective treatment or appropriate management specific to each patient.4,5,41,49–53
The optimal therapy for intrahepatic portosystemic venous shunts remains controversial. For those patients who are asymptomatic, having small shunts and demonstrating low shunt ratios (< 30%), intervention is not necessary and may reasonably be followed up due to the increased risk of hepatic encephalopathy.51,54,55 In a study of 134 cases of intrahepatic portosystemic venous shunts, Dessouky et al. 56 found that 42% of the asymptomatic cases did not require any intervention.
However, symptomatic patients are placed on dietary restrictions with limitation of protein intake and administration of lactulose to achieve nitrogen balance and, consequently, clinical improvement in the encephalopathy.5,26 In cases where the dietary management and modifications fail to control the symptoms of encephalopathy, surgical intervention, transcatheter embolization, shunt ligation, and/or hepatic resection may become warranted.27,42,56–60 Overall, the treatment of intrahepatic portosystemic venous shunts must be tailored to each patient and the severity of the abnormality and symptoms.
Conclusion
Intrahepatic portosystemic venous shunts with associated aneurysms are extremely rare vascular abnormalities that may be incidentally discovered in asymptomatic patients. Given the advancement and improvement in sonographic imaging, the visualization and evaluation of these shunts are very possible. Sonography has provided sonographers and radiologists the potential to directly visualize, identify, and evaluate various types of intrahepatic portosystemic venous shunts. An intrahepatic portosystemic venous shunt with an associated aneurysm as a connection may be suspected during sonography when a round anechoic (cystic) structure bridging a branch of the portal vein with a branch of the hepatic vein is identified. The sonographic characteristics previously mentioned not only may assist in recognition of this rare vascular abnormality, in the asymptomatic patient, but could also aid in the treatment planning, management, and long-term monitoring of the symptomatic patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.