
Abstract
Intrahepatic portosystemic venous shunt is a rare vascular anomaly that can occur congenitally or iatrogenically, leading to hyperammonemia and neurological complications such as hepatic encephalopathy. This report presents the case of a woman in her early 70s who developed recurrent episodes of altered consciousness following hepatobiliary surgery. Subsequent magnetic resonance angiography revealed an intrahepatic portosystemic venous shunt, and the patient underwent successful treatment with percutaneous transhepatic portal vein embolization. After treatment, her symptoms resolved completely, and she remained asymptomatic during an 8-month follow-up period. This report underscores the importance of considering intrahepatic portosystemic venous shunt in the differential diagnosis of postoperative neurological symptoms. Our findings suggested that percutaneous transhepatic portal vein embolization was effective in managing this case, leading to symptom resolution and sustained improvement during follow-up. Although this approach appears promising, further investigation is needed to establish its broader applicability. Early detection and appropriate management may help improve patient outcomes in selected cases.
Keywords
Introduction
The portal venous system plays a critical role in systemic metabolism and normal liver function. Aberrant shunting in this system can lead to severe consequences. Intrahepatic portosystemic venous shunt (IPSVS) is a rare pathological condition that can occur congenitally or iatrogenically, characterized by abnormal vascular communication that allows portal blood to bypass the liver and enter the systemic circulation directly. 1 This bypass compromises the liver’s ability to detoxify substances such as ammonia, potentially resulting in hyperammonemia and related neurological symptoms, including hepatic encephalopathy.2,3
Clinical studies have highlighted hyperammonemia as a major factor in hepatic encephalopathy, particularly in the presence of abnormal portal venous shunting.2,3 Despite advancements in understanding its pathophysiology, IPSVS is often overlooked due to its asymptomatic or nonspecific presentation, especially in patients with comorbid hepatobiliary diseases. This can lead to misdiagnoses such as psychiatric or neurological disorders. 4 Therefore, accurate diagnosis of portal venous anomalies in patients with postoperative recurrent episodes of altered consciousness is crucial for determining the etiology and optimizing treatment.
This report discusses the pathophysiology, diagnostic approach, and treatment strategies for iatrogenic IPSVS based on the case of a patient with a portosystemic shunt. This report emphasizes the therapeutic efficacy of percutaneous transhepatic portal vein embolization (PTPVE) and provides insights into the clinical management of iatrogenic IPSVS.
Case report
A woman in her early 70s with a history of acute cholecystitis, cholelithiasis, type 2 diabetic nephropathy, and hypertension was admitted to The First People’s Hospital of Linhai, Zhejiang, China, in May 2024. She underwent laparoscopic cholecystectomy and common bile duct exploration with stone removal 10 months ago due to acute cholecystitis and choledocholithiasis with acute cholangitis. Two months postoperatively, she developed progressive cognitive impairment, characterized by decreased alertness, apathy, difficulty communicating, and bilateral upper limb tremors.
Examination and diagnosis
Upon admission, the patient was disoriented and exhibited asterixis. Laboratory tests revealed elevated blood ammonia levels (89 μmol/L; normal range: 15–45 μmol/L), indicative of hyperammonemia. Brain computed tomography showed no significant abnormalities. Contrast-enhanced magnetic resonance angiography of the portal vein revealed abnormal communication between the hepatic and portal veins, with early enhancement of the hepatic veins, confirming the diagnosis of IPSVS (Figure 1). Initial medical management, including a low-protein diet, lactulose, and ornithine aspartate, temporarily alleviated the symptoms.
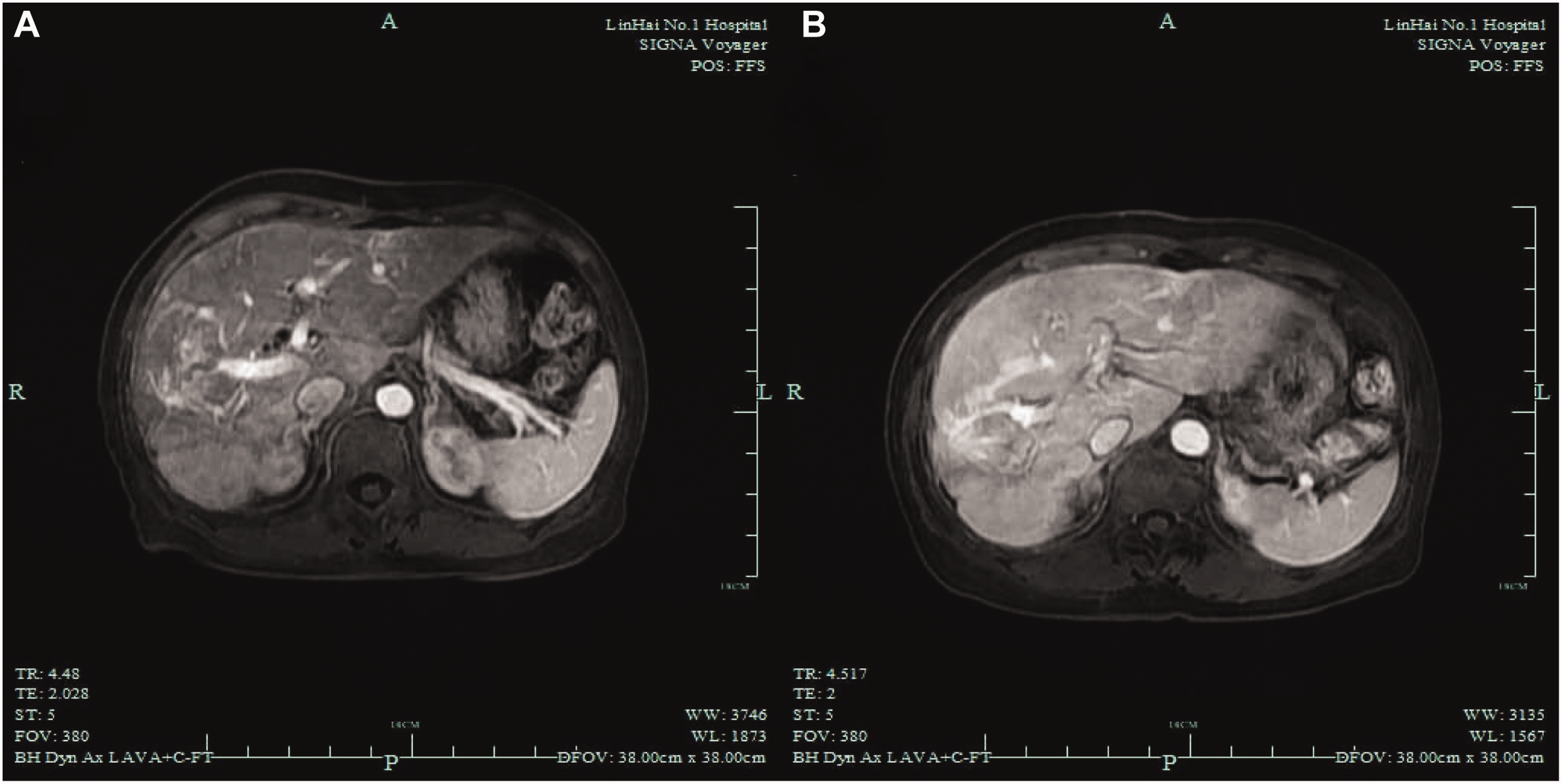
Enhanced magnetic resonance angiography of the portal vein. Imaging showing a tortuous vascular cluster between the two branches of the right portal vein and the right lower lobe hepatic vein, suggesting the presence of abnormal vascular shunting.
Intervention and treatment
The patient’s symptoms recurred after hospital discharge, and she showed persistently elevated ammonia levels. Further imaging revealed the precise location and distribution of the shunt, prompting the decision to perform PTPVE. Informed consent was obtained from the patient.
She underwent PTPVE under local anesthesia, performed by an experienced interventional surgeon with over 20 years of expertise in hepatobiliary and vascular interventions. The procedure was conducted under ultrasound and fluoroscopic guidance to ensure precise vascular access. An 18G puncture needle was carefully advanced into the main portal vein, and dark red blood was aspirated upon withdrawal of the stylet, confirming successful entry into the portal venous system. A 0.035-inch guidewire was then introduced and advanced under fluoroscopy guidance, followed by the exchange placement of a 5F vascular sheath to facilitate subsequent intervention. Venography revealed multiple portal venous–hepatic venous shunts, leading to a substantial diversion of portal blood flow. Using a microcatheter system, four abnormal portal branches were selectively cannulated. Coil embolization was performed using Cook Medical LLC’s Retracta® Detachable Embolization Coils (Bloomington, IN, USA), with a total deployment of eight 10 mm × 140 mm, four 8 mm × 140 mm, four 6 mm × 140 mm, and five 6 mm × 2 mm coils. The embolization strategy was designed based on the operator’s extensive experience in treating portal venous anomalies, ensuring optimal occlusion of the shunts while maintaining sufficient hepatic perfusion. Postembolization venography demonstrated a considerable reduction in portal venous shunting, with the restoration of normal intrahepatic blood flow.
Following the procedure, the patient’s symptoms improved considerably, and blood ammonia levels returned to normal during the 8-month follow-up period.
Discussion
Iatrogenic IPSVS is a rare yet potentially severe pathological condition with congenital and acquired etiologies. Studies have indicated that portal hypertension and liver cirrhosis are commonly reported, whereas iatrogenic IPSVS is less frequently reported.1,5 Portal venous shunting causes hyperammonemia through the following mechanism: toxic metabolites, such as ammonia, bypass hepatic detoxification and directly enter the systemic circulation, leading to neurological manifestations, including hepatic encephalopathy. 6 In the current case, the presence of recurrent episodes of altered consciousness following hepatobiliary surgery strongly suggested iatrogenic portal venous shunting.
IPSVS, which is defined as an abnormal communication between the portal and hepatic veins, is classified into four morphological types. 7 Type I, the most common type of IPSVS, involves a single large vessel connecting the right portal vein to the inferior vena cava. Type II involves one or more communications between the peripheral branches of the portal and hepatic veins. Type III involves aneurysmal connections between the veins, whereas Type IV includes multiple communications between the portal and hepatic veins across both liver lobes. In the current case, the clinical presentation and imaging findings of the patient suggested the diagnosis of iatrogenic IPSVS secondary to hepatobiliary surgery.
PTPVE has emerged as a minimally invasive and effective therapeutic approach that restores normal hemodynamics by occluding abnormal fistulas associated with congenital IPSVS, demonstrating promising clinical outcomes.8,9 Alvi et al. 10 reported the case of a 73-year-old woman with congenital IPSVS who was successfully treated with lactulose and rifaximin, suggesting that conservative management is adequate for mild symptomatic cases. In contrast, our patient required embolization due to persistent symptoms and progressive impairment. Chun et al. 11 described the case of an infant with IPSVS who was successfully treated with percutaneous embolization, highlighting the importance of early intervention. Although their case involved arterioportal fistulas, our study focused on venous shunting. Despite these differences, both cases underscore the effectiveness of embolization. In our study, the patient underwent successful embolization, resulting in complete resolution of symptoms and normalization of blood ammonia levels, with no recurrence observed during an 8-month follow-up period. These findings indicate that embolization is a viable treatment strategy for iatrogenic IPSVS. However, potential complications, such as elevated portal pressure and incomplete occlusion, necessitate careful preoperative assessment and vigilant postoperative monitoring.11,12 Therefore, clinicians must carefully evaluate the risks and benefits and ensure intraoperative precision. Long-term follow-ups with serial blood ammonia levels and imaging studies are essential to assess treatment durability and shunt closure.
Several reports have indicated that portosystemic shunting should always be considered in the differential diagnosis of hyperammonemia.6,13 Regular laboratory evaluation following diagnosis is critical, as prolonged hyperammonemia increases the risk of irreversible neurological impairment. 7 In this case, successful PTPVE not only demonstrated the efficacy of embolization for IPSVS but also emphasized the importance of postoperative vigilance. For patients presenting with recurrent neurological symptoms and hyperammonemia, routine imaging should be performed to identify possible portal venous anomalies. Early diagnosis and intervention for IPSVS are essential for preventing hepatic encephalopathy progression and improving the quality of life of the affected patients.
Conclusion
Iatrogenic IPSVS is a rare but potentially reversible vascular anomaly that can lead to hyperammonemia and neurological symptoms. This study demonstrates that PTPVE is a feasible treatment approach for managing IPSVS-related complications. In this case, PTPVE resolved neurological symptoms and normalized blood ammonia levels. Although this approach was effective in our patient, further research is needed to establish standardized treatment protocols and evaluate its long-term efficacy. Clinicians should consider IPSVS in the differential diagnosis of unexplained postoperative neurological symptoms, as timely intervention may improve outcomes.
Footnotes
Acknowledgements
Not applicable.
Author contributions
Weiting Chen, Yaling Jin: Thesis writing and editing;
Yaling Jin, Yuguang Wang: Data collection and organization;
Hui Wang: Manuscript revision and editing.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author upon reasonable request.
Competing interests
The authors declare that they have no competing interests.
Ethical approval
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. The case report has been de-identified by removing all personal details to ensure the patient’s privacy. The patient provided written informed consent for the publication of this case report, including the use of clinical data and images. The reporting of this study adheres to the Case Report (CARE) guidelines. 14
Funding
None.