
Abstract
The role of cardiac sonographers, as health care professionals, comprises facilitating a cardiologist’s diagnosis of valvular lesions, coronary artery disease, and congenital defects and assessing right-side pulmonary complications and so on. Occasionally, communication of differential diagnoses across several modalities, specialties, and healthcare providers is compulsory, in order to accurately confirm or deny an appropriate diagnosis for patients with unique presentations. This case study highlights the vital role of abdominal sonography, echocardiography, venography, and computed tomography in the diagnosis of a hepatic cyst. In addition, it demonstrates the appropriate measures that cardiac sonographers can take to fully investigate these lesions, especially when they are presumed to be a thrombosed inferior vena cava.
Introduction
An inferior vena cava (IVC) thrombosis, proximal to the heart, is a rare finding with the implementation of both abdominal sonography and echocardiography. In addition to the infrequency of these clots visualized on a sonogram, other factors might hinder a confident and accurate interpretation, such as extracardiac masses. Therefore, the skill level of the cardiac and diagnostic medical sonographer must be matched to the technically difficult nature of certain patients to ensure sonographic image quality. To obtain a more accurate diagnosis of suspected venous thromboses in the IVC and reduce a differential diagnostic list, a chest computed tomogram and venogram can assist physicians with increased diagnostic precision. Knowing how to streamline a patient’s care with additional noninvasive and invasive testing is fundamental in these types of situations and can cause a diagnostically challenging impasse.
Case Study
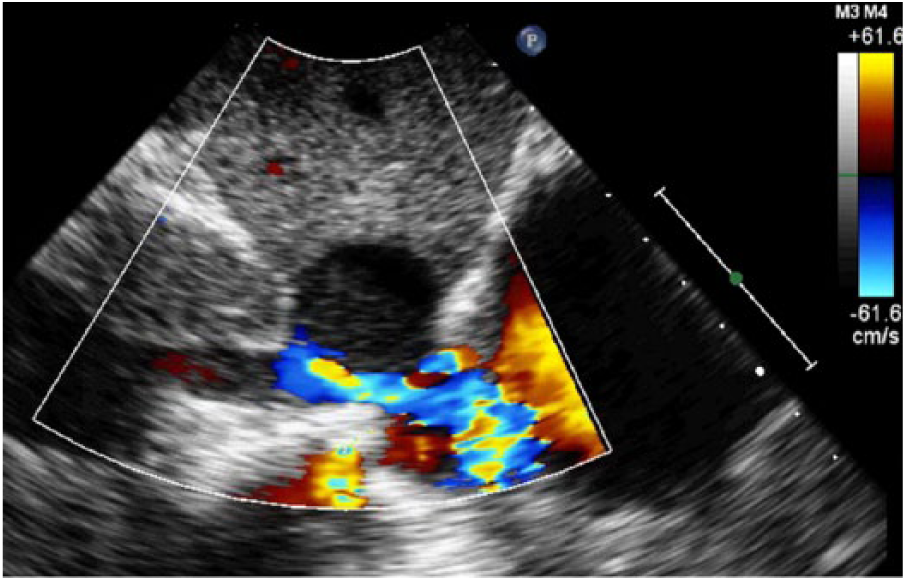
A middle-age patient with a history of tobacco abuse, dyslipidemia, diabetes, hypertension, and a Whipple procedure was referred to a cardiologist for a suspected IVC thrombosis at the confluence of the hepatic vein as detected on an abdominal sonogram (Figure 1). The limited abdominal sonogram demonstrated turbulent blood flow in the IVC as well as an approximately 3 cm nodular echogenic focus, which caused significant IVC luminal narrowing. Due to these findings, an echocardiogram was ordered to further delineate and hopefully better define the suspected lesion and adjacent cardiac anatomy. Echocardiography was implemented on a Philips iE33 ultrasound machine (Philips Healthcare, Bothell, WA) with an S5-1 MHz transducer at a frame rate of 48 Hz.
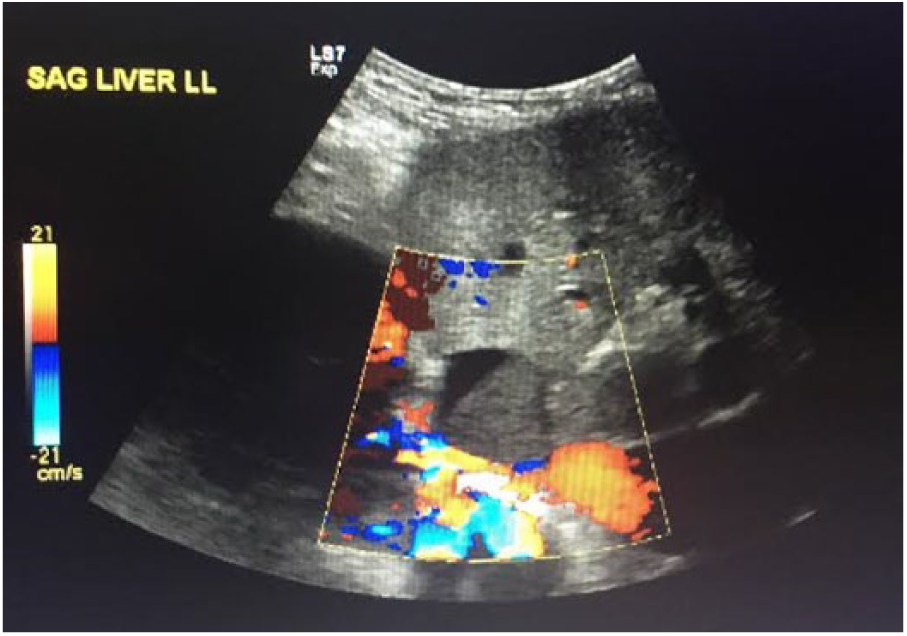
Right upper quadrant abdominal sonographic view demonstrating increased blood flow turbulence around a suspicious thrombus-like mass presumed to be in the inferior vena cava at the junction of the hepatic vein.
As with any complete, accredited echocardiography protocol, the subcostal view was scrutinized, with attention given toward the IVC and the suspected mass in the IVC (Figure 2). The results of the echocardiogram mirrored the abdominal sonogram. A partially obstructing mass/thrombus was visualized in the IVC at the junction of the hepatic vein (Figure 3). The mass measured 3.48 × 2.77 cm with echocardiography (Figure 4). Use of color Doppler demonstrated turbulent blood flow distal to the lesion leading into the right atrium (Figure 5). Pulsed wave Doppler (Figure 6) within the lumen of the IVC demonstrated a peak velocity of 1.5 m/s. Other echocardiographic findings included normal pulmonary artery pressures along with a normal right atrial area of 18 cm2 and a right ventricular dimension of 3.6 cm.
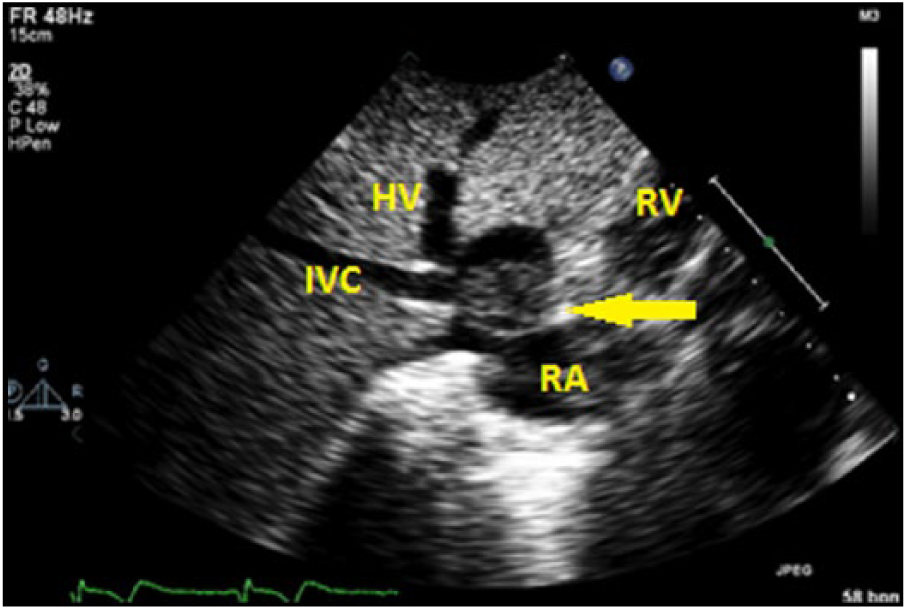
Echocardiogram without color Doppler showing the subcostal view with a suspicious mass located at the junction of the inferior vena cava (IVC) and hepatic vein (HV). The right atrium (RA) and right ventricle (RV) are also visualized.
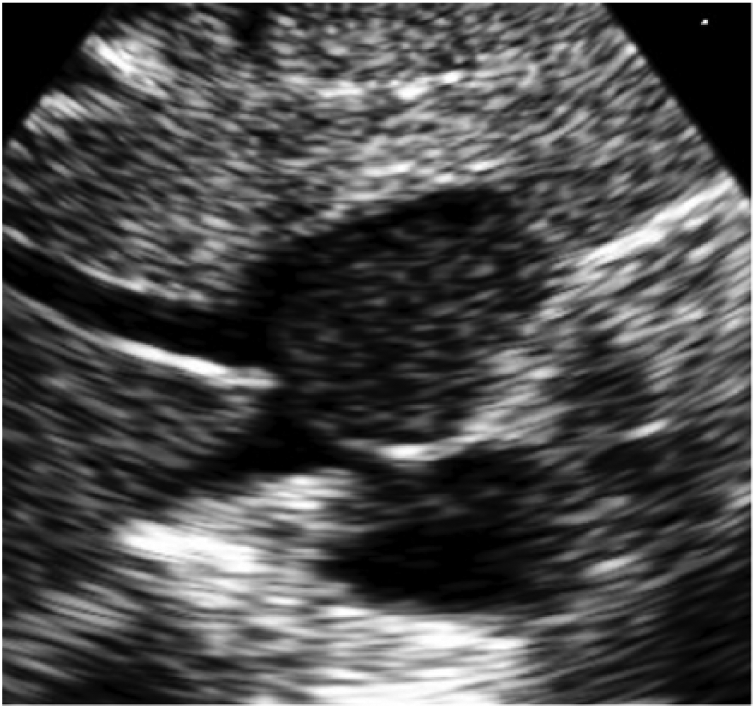
A magnified subcostal view demonstrating the heterogeneous appearance of the mass adjacent to the liver, inferior vena cava, and hepatic vein.
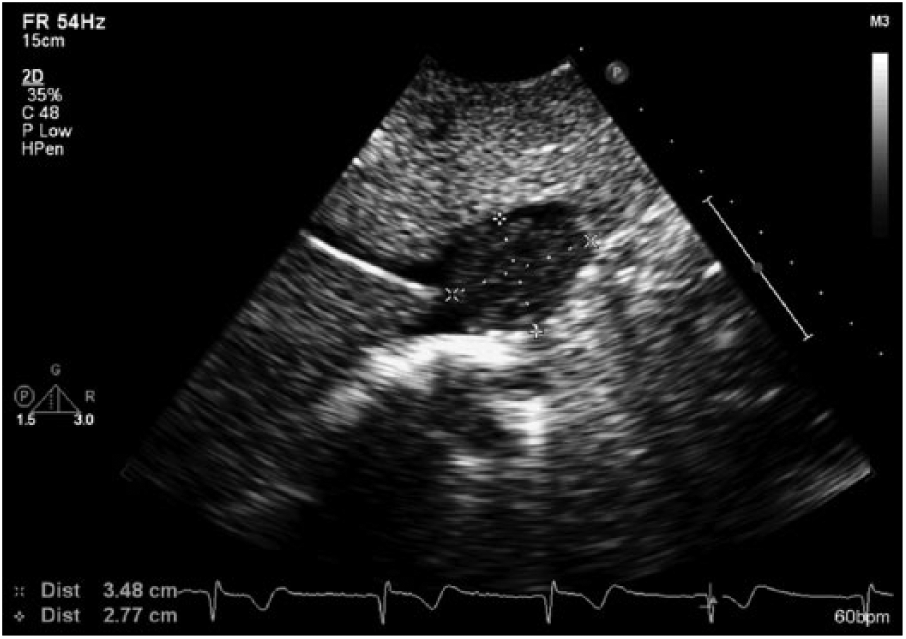
Caliper measurement of the mass at the junction of the inferior vena cava and hepatic vein.
Color Doppler illustrating turbulent blood flow around the suspicious mass in the inferior vena cava entering the right atrium.
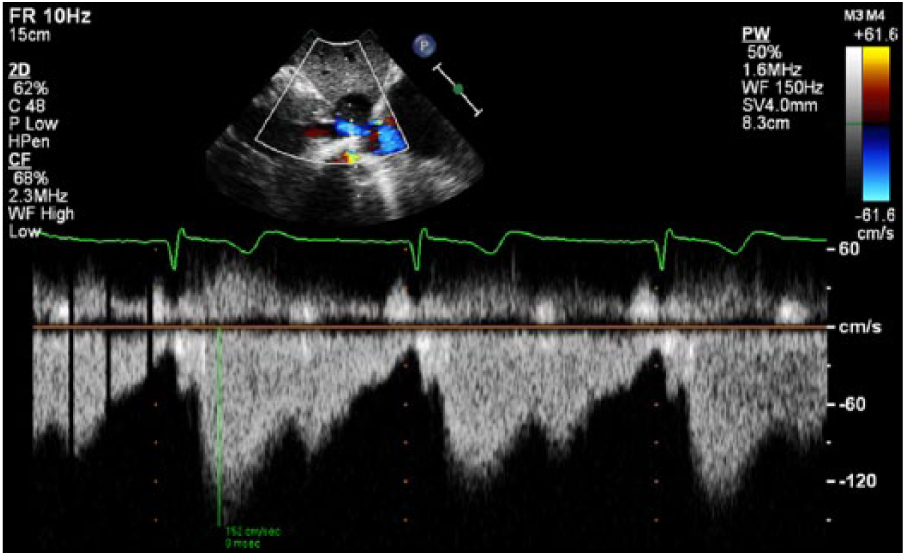
Pulsed wave Doppler of the turbulent blood flow distal to compression of the inferior vena cava. Velocity of blood flow was measured at 1.5 m/s.
A sequential venogram was then employed to rule out a thrombosis in the IVC versus an extracardiac mass. The venogram findings revealed a 3- to 4-cm filling defect within the left lateral aspect of the IVC. The borders were smooth and suggested an extrinsic compression process with unremarkably visualized hepatic veins and a lack of mobile thrombus (Figures 7 and 8). There was also brisk passage leading into the right atrium. Due to the extrinsic filling defect, a computed tomography (CT) scan of the chest was expedited to exclude underlying lymphadenopathy or other extracardiac masses.
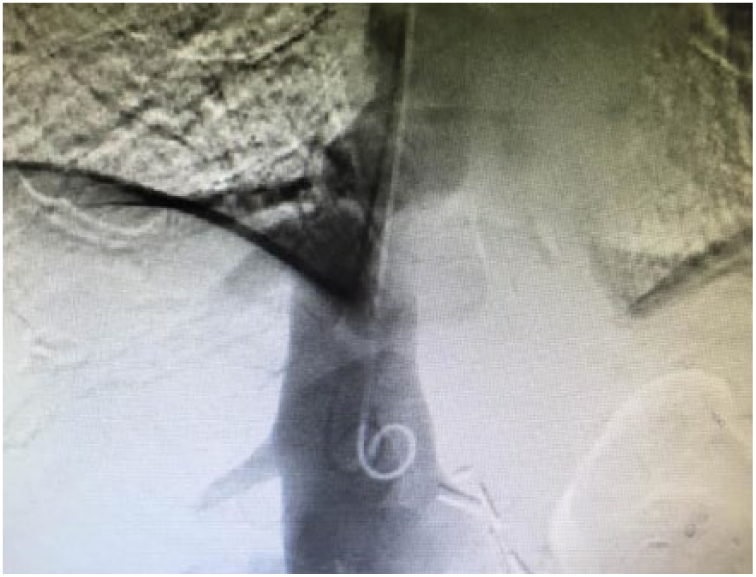
Venogram demonstrating a filling defect caused by an extrinsic, smooth process within the left lateral aspect of the inferior vena cava.
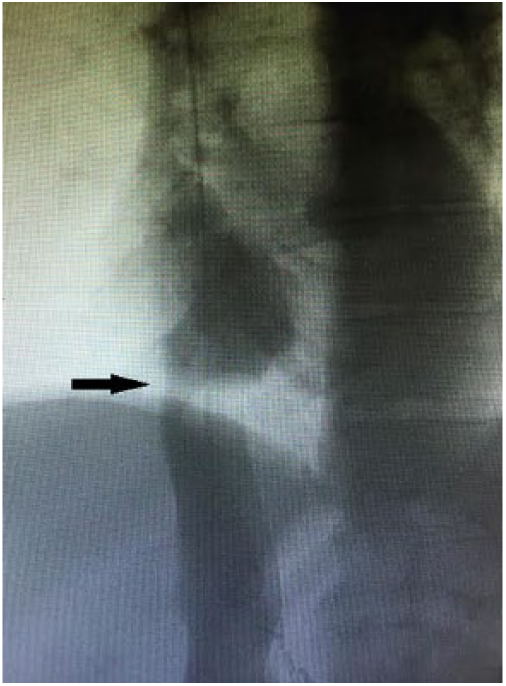
Venogram illustrating luminal narrowing (black arrow) of the inferior vena cava due to the extrinsic compression.
The chest CT scan demonstrated evidence of a complex appearing, nonenhancing cyst in the superior posterior aspect of the left lobe of the liver that measured 4.1 × 2.8 cm (Figure 9). The Hounsfield unit (HU) density of the cyst was 30 HUs. The HU is a CT unit of measure that quantifies the varying degrees of tissue and substance densities. 1 The higher the value of HUs, the denser the tissue in question. Less dense substances have a lower HU. As seen in Table 1, the varying degrees of HUs are compared with different types of substances. In this scenario, the mass in question has a similar density to soft tissue, according to Table 1. The cyst is also described as partially compressing the superior intrahepatic IVC, which is draped around the cyst, causing luminal narrowing. This narrowing poses further risk to the patient, which will be described later in the discussion. Furthermore, as initially discovered with the venogram, the CT scan also confirmed no definite thrombosis within the IVC.
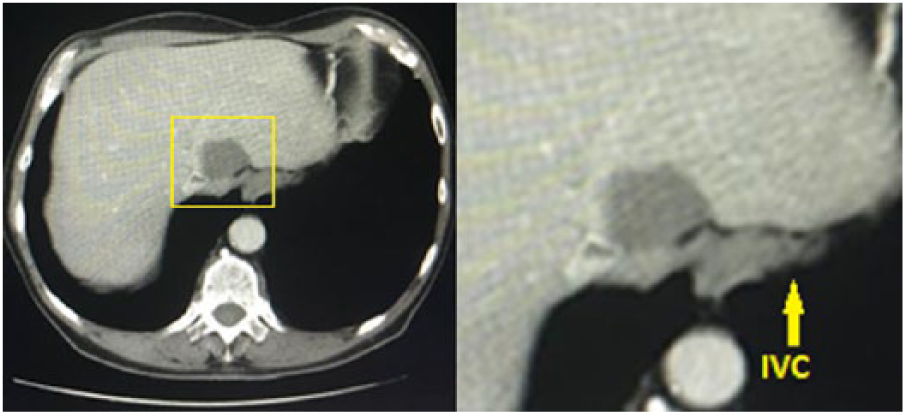
Chest computed tomography scan showing the hepatic cyst compressing the inferior vena cava (IVC), which is draped around the cyst (yellow outline). A magnified view showing the cyst in relation to the compressed IVC.
Hounsfield Units of Relative Densities of Various Substances a .
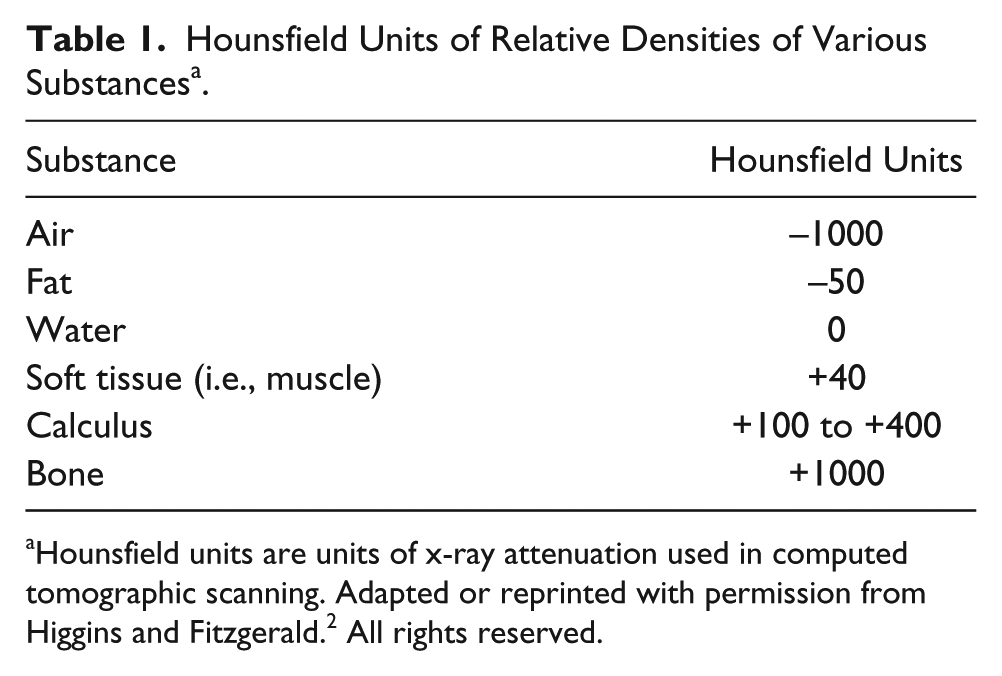
Hounsfield units are units of x-ray attenuation used in computed tomographic scanning. Adapted or reprinted with permission from Higgins and Fitzgerald. 2 All rights reserved.
Discussion
There are various types of cysts that can arise in the human body. Simple hepatic cysts are fluid-filled sacs that are seen in various sections of the liver. 3 Other types of cysts are those stemming from polycystic liver disease, cystic tumors, abscesses, and parasitic cysts, which come from ingesting food that is contaminated with parasitic eggs of tapeworms. 3 Complex hepatic cysts have the potential to congenitally develop or arise later in life, as seen in this case. 3 Most patients are asymptomatic from hepatic cysts, typically found in adults, incidentally with sonography or CT. 3 Although most liver cysts produce no symptoms and are not rare, if large enough, they can be palpable through the abdomen and corrected with surgery if severe pain develops. Conversely, there is no need to treat smaller cysts in the liver. 4
Although this patient had no visual signs of thrombosis, similar studies have shown that compression of the IVC due to extrinsic hepatic cysts has indeed led to secondary formation of thrombus burden, yet on an infrequent basis.5–9 In one study of 141 patients with IVC thrombosis, 16% of the cases were due to external compression of the IVC. 10 So, although in this case study, there was a lack of definite thrombosis in the IVC, this patient had already developed a risk of thrombus development from stasis and obstruction of laminar blood flow due to the compression of the liver cyst, thus increasing the risk of pulmonary embolism. Discovery of IVC clots rarely occurs during an echocardiogram; however, sonography can be a useful tool in documenting characteristics of the IVC and the right heart. Paying special attention to the right-side anatomy and cardiac hemodynamics is paramount when dealing with circumstances involving venous thrombosis and hepatic masses compressing the IVC.
Hepatic cysts are just one cause of IVC compression. Although it is uncommon to see a compressed IVC incidentally during an echocardiogram, IVC syndrome is not a rare condition. Other causes of IVC compression and obstruction include (but are not limited to) pregnancy, bowel obstruction, abdominal aortic aneurysm, Budd-Chiari syndrome, and mediastinal masses.11–14
The uniqueness of this study lies within the rarity of finding a compressed IVC during an echocardiogram due to external sources and what the cardiac sonographer can do to fully quantify and investigate the source of compression. Whereas abdominal sonographic imaging can be similar to the subcostal cardiac window, the cardiac sonographer’s familiarity with the heart anatomy adds value to supplementary noninvasive testing, with regard to right-side anatomy. From the cardiac sonographer’s perspective, this case study is one example of how it is possible to manipulate the ultrasound transducer to visualize the IVC, hepatic vein, liver, and the right heart. This study also provides an example of which image optimizations cardiac sonographers should make, from a technical standpoint, to adjust a subcostal image to its fullest potential for diagnosis of an IVC thrombosis or hepatic mass.
To obtain images of the IVC, hepatic vein, and liver from the subcostal window during an echocardiogram, patients should lie in the supine position with their knees bent to relax the abdominal muscles (if possible). The probe is placed under the patient’s ribs in the epigastric region with the indicator aimed at the patient’s left shoulder. The IVC and hepatic veins can be visualized by turning the indicator toward the patient’s right shoulder with an inferior angulation of the probe. 15 From there, respiratory changes and IVC size can be documented, and from this quantitative and qualitative information, right atrial pressures can be estimated. In this case study, flow hemodynamics around the cyst compressing the IVC are recognized with color Doppler and spectral Doppler. As seen in Figure 5, color Doppler proves that there is a break in laminar blood flow within the vessel. The mosaic pattern of blood flow within and distal to the lesion tells us that there is a higher than normal velocity stemming from the obstruction. Sonographers should implement pulsed wave Doppler, as seen in Figure 6, to assess the peak velocity of blood traveling around the compressed IVC.
Imaging depth within the subcostal window varies. Depending on the patient’s adipose tissue, varying imaging depths may be necessary for different patients. Due to the distance between the transducer and the heart in more obese patients, maximal depth in the far field zone may be essential. Once the appropriate depth is determined, sonographers should measure the IVC/hepatic vein lesion with calipers (Figure 4). When measured, this can help correlate with the measurements of other modalities. As seen in the sonograms, zoom magnification and unmagnified images are necessary to visualize the lesion more closely and its adjacent anatomy, respectively. Also, as seen in Figure 2, the focus is positioned in the middle where the hepatic cyst is located. For optimal image quality, align the focus along the sector at the region of interest and minimize the sector width to increase frame rate.
Furthermore, the color scale in the abdominal sonogram and echocardiographic images are set at different values. One method to detect flow in traditionally lower velocity areas is to lower the color scale. This was performed in the abdominal sonogram. In echocardiography, the typical color Doppler scale is 50 to 60 cm/s. 16 Instead of lowering the scale below 50 cm/s to bring outflow in the IVC, the sonographer adjusted the flow optimization setting to “low.” One additional testing consideration that would have helped to improve the study, if available, would be the use of 3D echocardiography. 3D echocardiography would provide a more detailed internal perspective of the IVC, mass, and any clot formation around the compression. 17 The combination of these tactics will help sonographers in fully scrutinizing hepatic lesions/IVC thrombosis in similar circumstances.
Conclusion
This case is a rare scenario that should be emphasized for both cardiac sonographers and cardiologists as to the importance of using the subcostal window on patients to specifically visualize the IVC. Strictly adhering to an echocardiography lab’s protocol and how adjustments are made to the sonographic settings and “knobology” can be critical. On a physician level, the strides taken to properly structure this patient’s healthcare were achieved through the appropriate diagnostic tests and procedures used to identify and diagnose this lesion in a timely sequence from the initial abdominal sonogram to the chest CT scan.
Although this was determined to be outside of the cardiovascular system and not indeed an IVC thrombosis, the patient is still ironically at risk for clot development around the mass. This scenario should underscore the possibility of discovering difficult incidental findings during any sonogram and to consider varied differential diagnoses as patients are imaged.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.