
Abstract
Ventricular septal rupture (VSR) is a rare life-threatening mechanical complication secondary to acute myocardial infarction that usually occurs 2 to 8 days after infarction and frequently precipitates cardiogenic shock. The mortality rate for VSR has been reported to be between 41% and 80%; therefore, immediate surgical intervention should be considered. Furthermore, VSR is a complication of 0.17% to 0.31% of patients who present with an anterior myocardial infarction. Because of the rarity of this pathology, the role of transthoracic echocardiographic investigation will help to improve what is already considered a poor prognosis for these types of patients. This case study illustrates how transthoracic echocardiography plays an essential role in the rapid assessment and diagnosis of VSR in clinical practice.
Ventricular septal rupture (VSR) is a rare life-threatening mechanical complication secondary to acute myocardial infarction (MI) that usually occurs 2 to 8 days after infarction and frequently precipitates cardiogenic shock.1,2 The mortality rate for VSR has been reported to be between 41% and 80% 3 ; therefore, immediate surgical intervention should be considered. Furthermore, VSR is a complication of 0.17% to 0.31% of patients who present with an anterior myocardial infarction. 3 Because of the rarity of this pathology, the role of transthoracic echocardiographic investigation will help to improve what is already considered a poor prognosis for these types of patients. This case study illustrates how transthoracic echocardiography plays an essential role in the rapid assessment and diagnosis of VSR in clinical practice.
Case Study
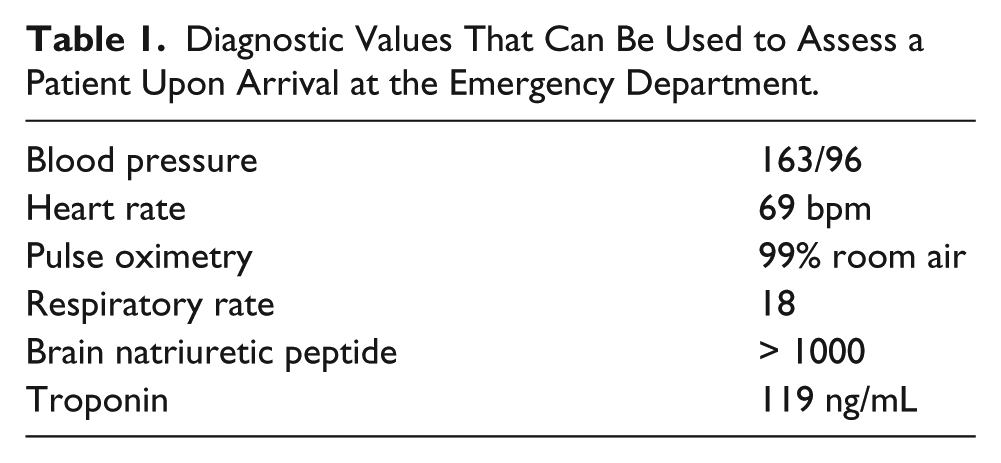
A 67-year-old female patient presented to the emergency department (ED) with progressive burning chest pain radiating to the right arm and jaw. She denied previous cardiac symptoms prior to this event. Physical examination revealed elevated blood pressure, troponin, and brain natriuretic peptide (BNP) levels (Table 1). Of note, normal levels of troponin are not measurable in healthy patients and normal BNP levels are less than 100 pg/mL for both men and women.4,5 However, both of these cardiac marker values were significantly elevated in this patient. Along with an abnormal physical examination and lab results, the initial 12-lead electrocardiogram (EKG) showed a right bundle branch block and septal infarct and lateral injury pattern with an anterolateral myocardial infarction (Figure 1). ST segment elevation in leads I, aVL, and V2 is represented by the black circles and ST depression in leads II, III, and aVF is represented by the black arrows. There was also associated T-wave inversion in leads V1 to V3, represented by the large blue circle (Figure 1). Patient symptoms, serology, and EKG findings are consistent with an ST elevation myocardial infarction. The patient was immediately taken to the cardiac catheterization laboratory for intervention. Cardiac catheterization demonstrated a 100% stenosis with thrombus in the proximal left anterior descending artery and a left ventricular ejection fraction of approximately 25% by ventriculography. Intervention was performed and a drug-eluding stent was successfully placed across the lesion with 0% residual stenosis.
Diagnostic Values That Can Be Used to Assess a Patient Upon Arrival at the Emergency Department.
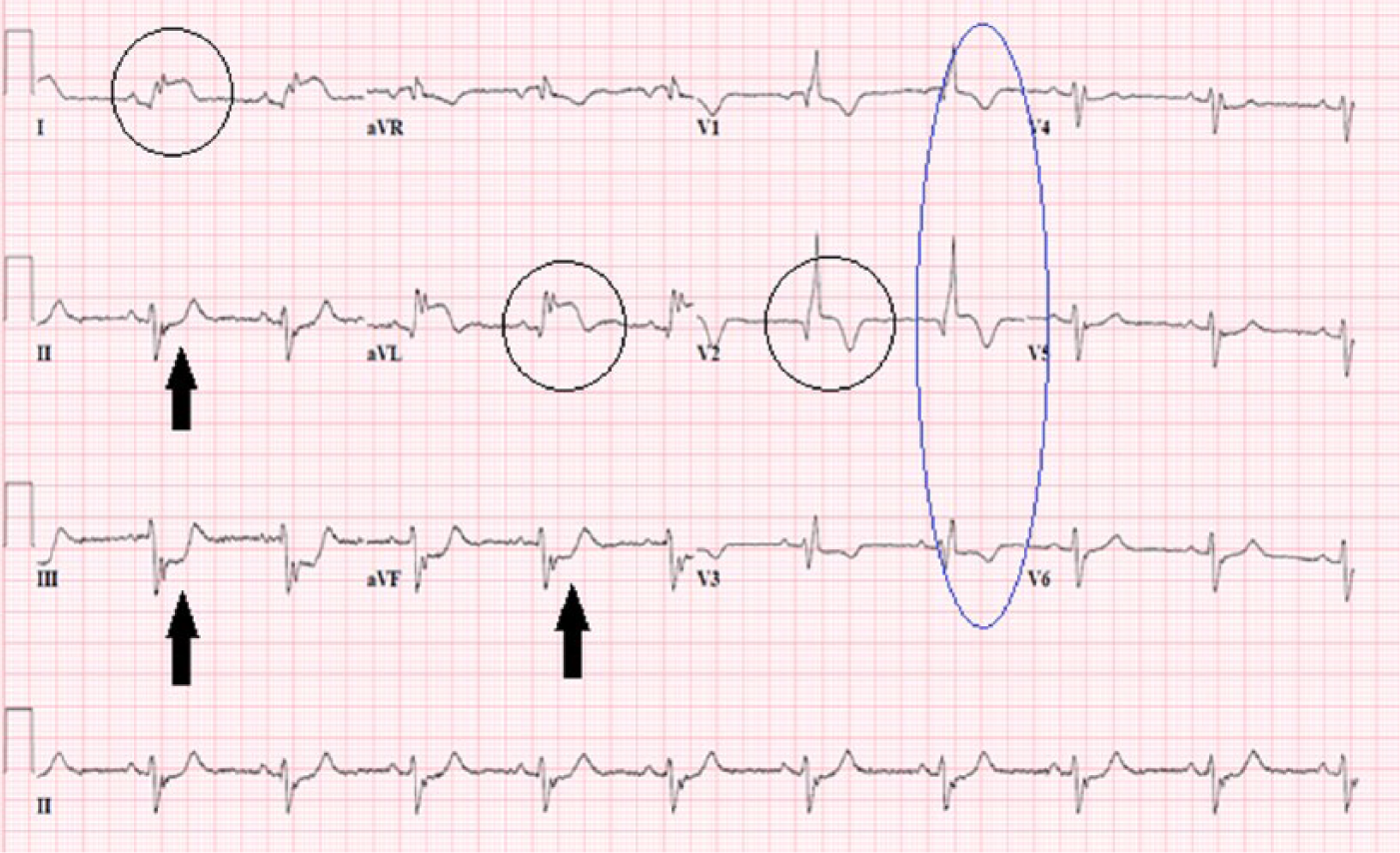
Patient’s electrocardiogram demonstrating ST elevation and depression throughout the precordial and limb leads.
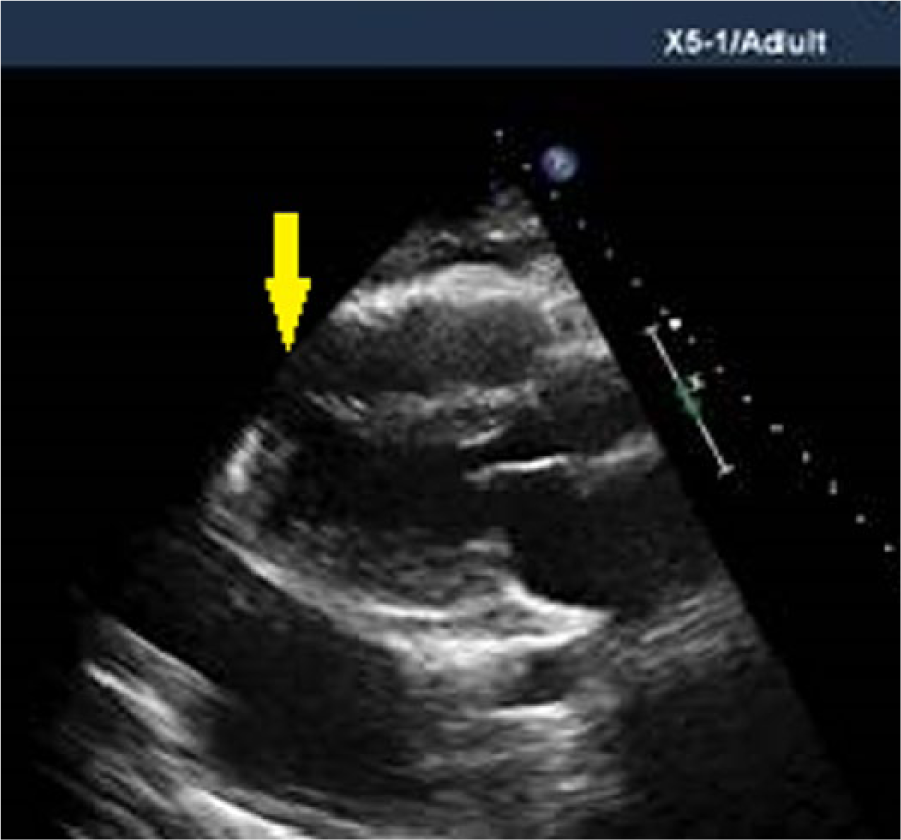
Transthoracic echocardiogram was performed the next day and demonstrated a left ventricular ejection fraction of 30% to 35%, respectively. There was severe hypokinesis of all apical and distal segments and hypokinesis of the mid anterior and anteroseptal walls. A trivial pericardial effusion (seen only in systole) was noted circumferentially. Contrast was used to delineate endocardial borders and evaluate the apex due to poor technical image quality. The perflutren contrast agent Definity (Lantheus Medical Imaging, North Billerica, MA) was administered intravenously according to the product package insert. Images were acquired with a broadband transducer using power modulation–contrast-specific settings at a very low mechanical index of 0.25 (iE33; Philips Healthcare, Andover, MA) and a frame rate of 43 Hz. There appeared to be a small aneurysmal segment in the apical septal wall with slight bulging in systole (Figure 2). The patient was eventually stabilized, discharged, and instructed to follow up with her cardiologist in 2 weeks.
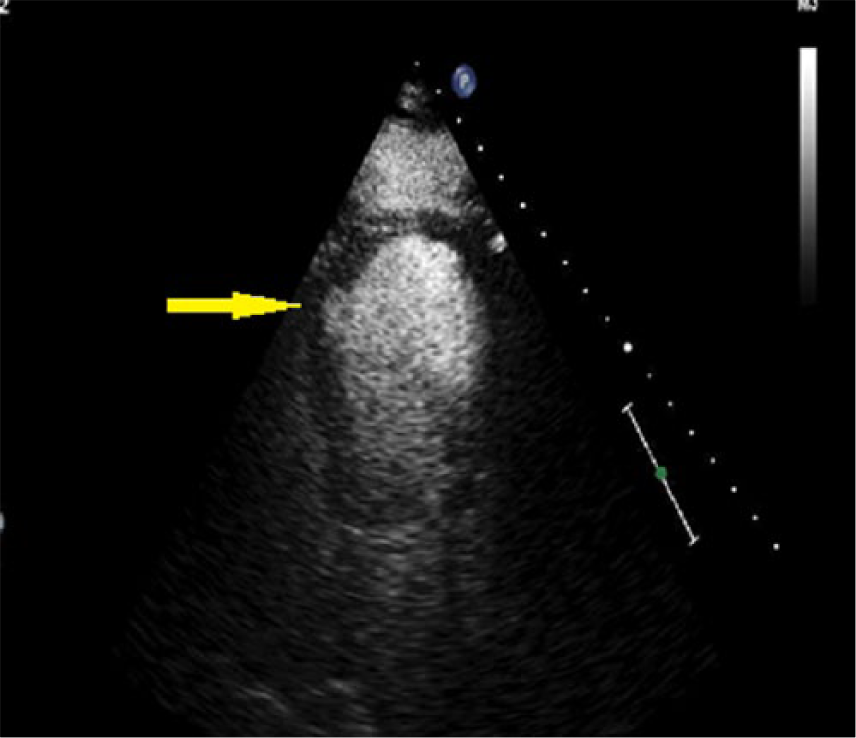
An apical four-chamber view showing an apical septal aneurysm seen with contrast (yellow arrow).
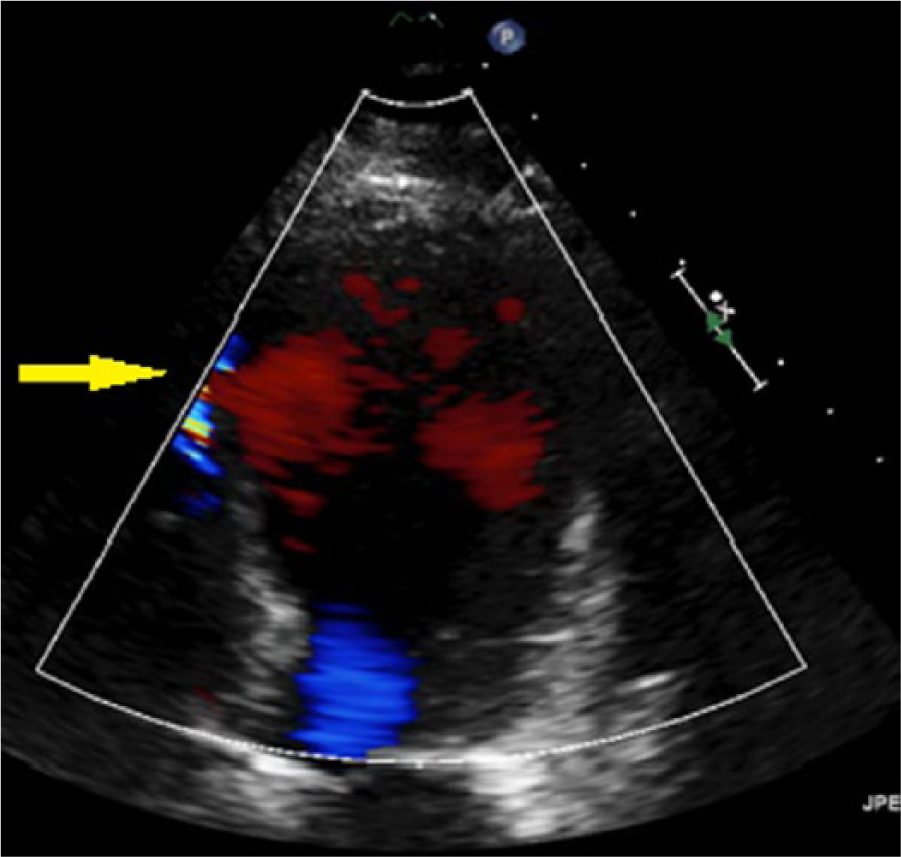
The patient returned to the emergency department 8 days later with severe nausea, vomiting, and weakness. In addition, clinical examination revealed acute, decompensated heart failure and a new heart murmur. The patient was admitted to the hospital’s critical care unit. A transthoracic echocardiogram was ordered to evaluate the murmur, which demonstrated a possible shunt in the apical septal wall (Figure 3). Subsequently, a repeat echocardiogram was performed to interrogate the questionable findings in more detail, which led to confirmation of a VSR of the apical septal wall with left-to-right shunting demonstrated by color Doppler imaging (Figure 4). (Figure 5 demonstrates the shunt without color Doppler.)
Apical four-chamber view showing a small retrograde jet with turbulent color Doppler flow (yellow arrow).
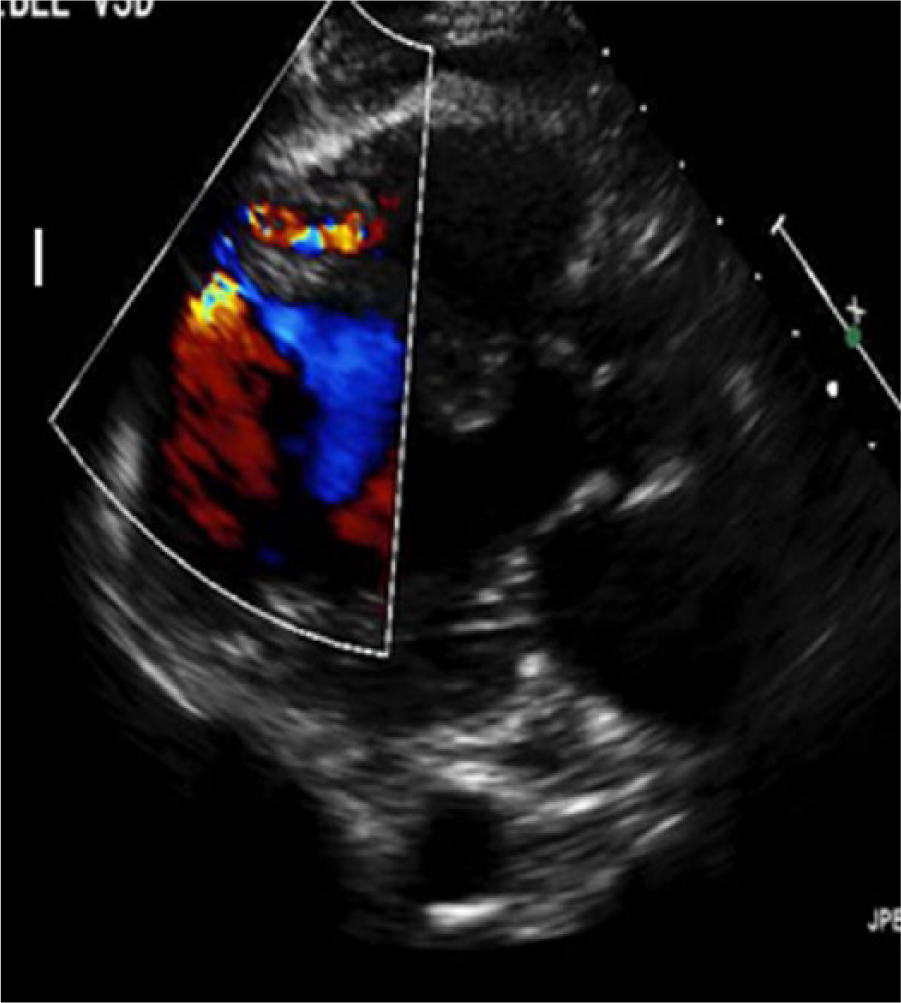
Slightly off-axis parasternal long-axis view showing an apical septal left-to-right shunt due to acute ventricular septal rupture with color Doppler, proving the value of nontraditional echo windows.
Parasternal long-axis view without color Doppler illustrating the ventricular septal rupture toward the distal part of the septum (yellow arrow) and an associated pleural effusion.
Discussion
Since VSR is such a rare occurrence, no separate classification method has been developed, resulting in the utilization of the currently accepted method proposed by Becker and van Mantgem. 6 Three types of VSR have been described by the original classification of type I, II, and III. A type I lesion is defined by an abrupt tear in the ventricular wall without thinning, a type II VSR is defined as infarcted myocardium that erodes before rupture and is covered by thrombus, and type III describes the perforation of a previously formed aneurysm. 1
The cardiac sonographer may be the first in line to evaluate a VSR, rapidly identifying left ventricular wall borders from multiple imaging windows. Because a VSR may not be present in the standard imaging planes, it is the responsibility of the cardiac sonographer to angle (sweep) through regions of the myocardium to determine what structural damage has occurred, if any. This is especially important in a patient with a recent MI and new heart murmur, as VSR should be suspected. In this case, it appears that there was an apical aneurysm present during the first transthoracic echocardiogram performed, as seen in Figure 2, which would classify this particular case as a type III rupture.
Upon confirmation of a VSR, given the mortality rate, it is imperative that the cardiac sonographer relay the findings immediately to the interpreting physician. A comprehensive evaluation of intracardiac shunting includes 2D, color, and continuous wave Doppler. Although pulmonary-to-systemic blood flow ratio (Qp/Qs) would be performed on traditional septal defects to determine timing of surgery, this is not necessary, as a VSR would be closed acutely.
However, it is worthy of discussion for properly obtaining the Qp/Qs for the cardiac sonographer in clinical practice. When there is suspicion of shunting between chambers, whether it is congenital or acquired, calculations of right- and left-side stroke volumes and cross-sectional areas of outflow tracts are applied to the Qp/Qs equation. This equation determines the magnitude of the shunt, giving a shunt ratio that assists in determining the presence and magnitude of the shunt. To calculate Qp/Qs, the right ventricular stroke volume and left ventricular stroke volume are derived from four measurements: Right ventricular outflow track (RVOT) diameter, left ventricular outflow track (LVOT) diameter, a pulsed wave Doppler velocity-time integral (VTI) of the RVOT, and a pulsed wave Doppler VTI of the LVOT, which are taken from both the parasternal and apical imaging windows. 7 The equation is SVRVOT / SVLVOT. A normal shunt ratio is 1:1 because both the systemic and pulmonary systems recognize equal blood flow volumes. 4 In this instance, right-side pressures estimated for this patient were moderately elevated and a Qp/Qs was calculated as 1.5 (32 mLRVOT / 22 mLLVOT), which is classified as a significant shunt by hemodynamic quantification. 7 Surgical intervention was considered and preparation was attempted; however, the patient continued to decline.
Some difficulties encountered in obtaining accurate Qp/Qs are poorly visualized cardiac anatomy, additional cardiac pathology that would interrupt an accurate LVOT velocity (i.e., hypertrophic obstructive cardiomyopathy), and irregular heart rhythms. It is fundamental that sonographers accurately measure the left and right outflow track diameters because these values are squared in the equation. If the measurement is incorrect, the ratio may be underestimated or overestimated significantly, possibly changing the route of care for that patient. According to the Qp/Qs equation, a shunt ratio of > 1:1 indicates that pulmonary flow is greater than systemic flow.
Most VSRs present themselves within 3 to 5 days post-anterior myocardial infarction.8–11 According to Arnaoutakis et al., 12 if surgical repair is considered, surgical mortality rates are 54.1% if performed within 7 days of an MI. Factors contributing to a worsening prognosis include right ventricular dysfunction, cardiogenic shock, multiple organ failure, and severity of the VSR. 13 If surgery is delayed or the patient presents to the hospital for emergency after 7 days post-MI, surgical mortality rates are 18.4%. 12
Conclusion
In patients with recent MI presenting with a new murmur and worsening heart failure, the presence of a VSR should be considered. The cardiac sonographers’ role in evaluation of intracardiac shunting is critical in patients with a suspected VSR, as the mortality rate is high.
In this case study, the VSR was able to be assessed by the cardiac sonographer using off-axis and nontraditional windows. Expecting the unexpected in sonography is the best mindset to approach a difficult patient examination and to use problem-solving skills, which may result in high-quality outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.