
Abstract
Cardiac rupture, such as ventricular free-wall rupture, ventricular septal perforation, and papillary muscle rupture, is a life-threatening complication of acute myocardial infarction. Herein, we report a very rare case of combining these three types of ventricular rupture. A 71-year-old woman underwent mitral valve replacement and left ventricular free-wall rupture repair after an acute myocardial infarction. She was transferred to our hospital under mechanical support by venoarterial extracorporeal membrane oxygenation and intra-aortic balloon pump due to circulatory collapse. Transthoracic echocardiography revealed a left-to-right shunt caused by ventricular septal perforation. The patient underwent endoventricular patch plasty for septal defect closure. Unfortunately, a prolonged postoperative course led to the development of multi-organ failure followed by fatal outcome on day 32 postoperatively. To our best knowledge, this is the first reported case of ventricular triple rupture associated with acute myocardial infarction.
Keywords
Introduction
Cardiac rupture is relatively infrequent but life-threatening complication of acute myocardial infarction (AMI). It is classified as ventricular free-wall rupture (FWR), ventricular septal perforation (VSP), or papillary muscle rupture (PMR). According to Shimizu et al., 1 mortality was found to be 23.9%, 31.7%, and 37.9% in patients with FWR, VSP, and PMR, respectively. A combination of any two types of rupture, called ventricular double rupture (VDR), has been reported. 2 However, a case of simultaneous occurrence of all three mechanical complications has not been reported. Herein, we report the case of ventricular triple rupture (VTR) in a 71-year-old woman due to AMI.
Case report
A 71-year-old woman with chest pain for 2 days was admitted to a previous hospital. Electrocardiography showed ST-segment elevation in leads II, III, and aVF, andST-segment depression in leads V1-2 (Figure 1). Serum creatine kinase (CK) and creatine kinase-MB (CK-MB) levels were increased to 1596 and 139 IU/L, respectively. Emergency coronary angiography revealed occlusion of the distal site of the right coronary artery (RCA) (Figure 2(a)). Percutaneous coronary intervention in the RCA (Xience Xpedition®, Abbott laboratories, Abbott Park, IL, USA) was performed in the previous hospital. On day 1, severe mitral regurgitation developed, which required an emergency operation. Since the posterior papillary muscle ruptured in the operation field, consistent with PMR, it was resected. Moreover, mitral valve replacement (Mosaic® 27 mm, Medtronic plc, Minneapolis, MN, USA) and coronary artery bypass grafting with saphenous vein to the left anterior descending artery were performed. Intraoperatively, hemopericardium with an oozing type of FWR was found. Therefore, FWR was repaired using a sutureless technique using a fibrinogen-combined sheet (TachoSil®, Takeda, Osaka, Japan). On day 2, the patient experienced cardiogenic shock with electrocardiographic changes: stent thrombosis due to discontinuing prasugrel was considered. However, coronary angiography showed no significant coronary stenosis. Causes of these sudden changes were unclear at that time due to persistent hemodynamic instability. Therefore, peripheral venoarterial extracorporeal membrane oxygenation (ECMO) combined with intra-aortic balloon pump (IABP) was applied for hemodynamic support, and the patient was transferred to our hospital on day 5.
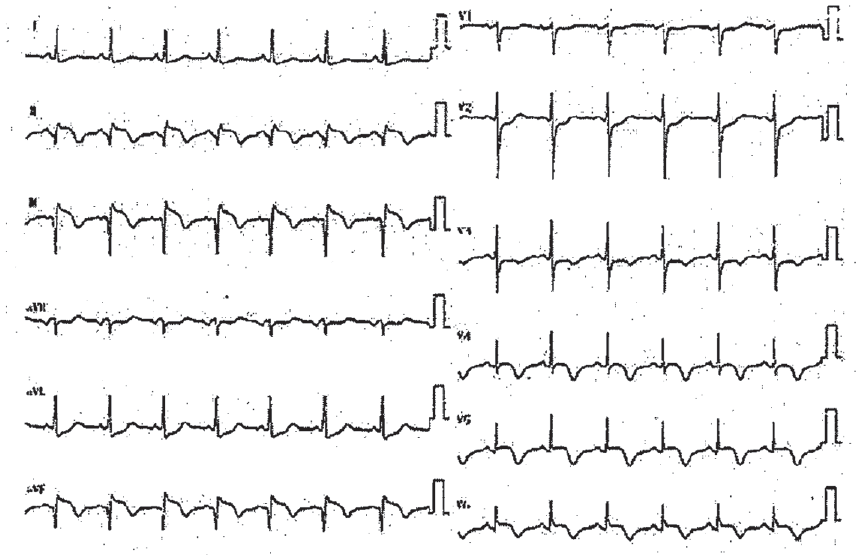
Preoperative electrocardiography showed ST-segment elevation in leads II, III, and aVF, and ST-segment depression in leads V1–2.

(a) Preoperative coronary angiography demonstrating occlusion (indicated by the yellow arrow) of the distal site of the RCA. (b) Transthoracic echocardiography revealed a left-to-right shunt caused by the postinfarction ventricular septal defect.
On admission, a chest radiograph revealed lung congestion. Furthermore, transthoracic echocardiography revealed a left-to-right shunt caused by VSP, which might have caused hemodynamic instability on day 2 in the previous hospital (Figure 2(b)). Peripheral ECMO was switched to central ECMO with left atrial venting, withdrawing IABP, on day 5. Cerebral computed tomography (CT) was performed owing to the patient’s depressed mental status. It revealed hemorrhagic infarction within the left cerebellar hemisphere and occipital and parietal lobes (Figure 3(a) and (b)). Cardiac magnetic resonance imaging was performed during the waiting period, revealing an apical aneurysm of the left ventricle. Due to development of cerebral hemorrhagic infarction, surgical repair was delayed and performed 30 days after circulatory support initiation.

Cerebral CT revealed hemorrhagic infarction within the left cerebellar hemisphere (a) and the occipital and parietal lobes (b).
Endoventricular patch plasty combined with VSP closure was performed. Small defects were observed through incision of the thin inferior wall of the aneurysm at the interventricular septum (Figure 4(a)). All defects were excluded using a bovine pericardium patch (Figure 4(b)). Then, endoventricular patch plasty for left ventricular aneurysm was performed: a double patch with bovine pericardium and a Dacron patch (J Graft®, Japan Lifeline Co., Ltd., Tokyo, Japan), and the incision was closed with Teflon felt strip reinforcement. The patient could wean from extracorporeal circulation with the assistance of IABP.
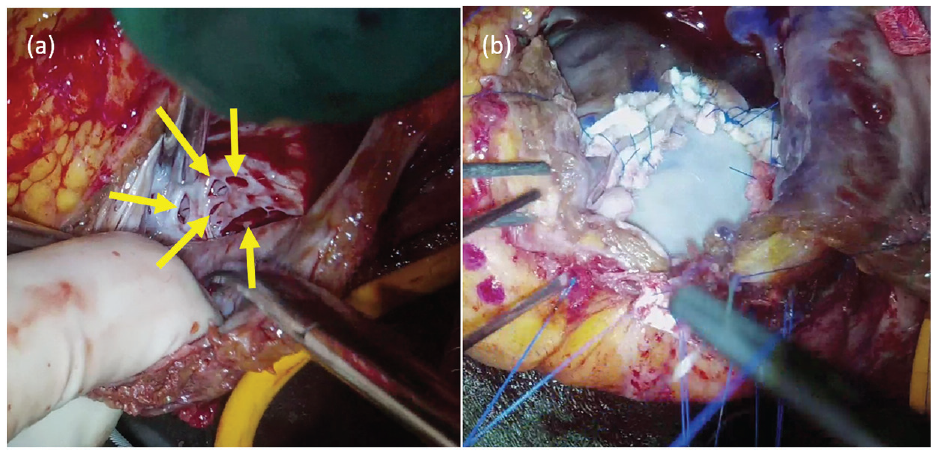
Operative views. (a) Small defects at the apical side of the aneurysm. (b) We excluded all the defects with a patch of bovine pericardium.
Regarding complications of right thoracic suction, the right inferior pulmonary vein was injured and the packing gauze into her right thorax could not control this injury.
A prolonged postoperative course led to the development of multi-organ failure followed by fatal outcome on day 32 postoperatively.
Discussion
Left ventricular FWR, VSP, and PMR are rare but fatal complications of AMI. In the era of reperfusion therapy, these complications have dramatically reduced. 3 However, these events often lead to rapid deterioration in the patient’s clinical condition. 4 On the contrary, it is also said that surgical mortality has increased because of the change in the nature of the patients coming to surgery. 5 If this clinical condition is not treated surgically, the mortality rate is reported to be nearly 80% within a week, 6 to save patients’ lives, early diagnosis and surgical repair are needed. To our best knowledge, simultaneous emergence of all three complications has not previously been reported in the literature.
VDR, defined as a combination of any two of the three forms of cardiac rupture, has been reported, and they commonly present as a combination of FWR and VSP. 6 Mann et al. 7 classified VDR into two types: true and junctional. In the true type, distinct tears can be observed in the ventricular septum and free wall. In the junctional type, rupture is located where the left ventricular septum and free wall meet; this was observed in the present case. Several reports have shown that female sex, advanced age, hypertension, and first MI were risk factors of cardiac rupture.
In this case, FWR and VSP were true types: the patient was female, an older adult, diagnosed with hypertension, and had recently sustained her first MI. VSP occurred after time passed after initial VDR, despite reperfusion of the coronary artery, which is extremely rare. However, we suggested that this occurred accidentally. Abandonment of after load reduction using IABP after the initial repair might have resulted in left ventricular aneurysm formation followed by VSP. Mechanical circulatory support after VDR has to be considered for preventing VTR.
Conclusion
We report the first case of VTR associated with AMI. It is necessary to always observe subsequent cardiac rupture when one of the mechanical complications occur.
Footnotes
Acknowledgements
The authors are grateful to Editage for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from legally authorized representatives for the anonymized patient information to be published in this article.