
Abstract
A particular pelvic pathology that may not be recognized, and is easily missed, is pelvic congestion syndrome. There is limited understanding about this condition, and many sonographers may have limited to no knowledge of this disorder. This article is to bring an awareness of this condition and the sonographic images necessary to obtain, so that further testing and possible treatment could relieve the patient of symptoms. Since a pelvic sonogram is generally the first modality of choice when an assessment of the pelvic organs is ordered, detailed imaging of all the pelvic region should be evaluated, including the vessels within this area. When evaluating a patient with chronic pelvic pain and visualizing any dilated vessels during a transabdominal or transvaginal sonogram, further imaging and documentation are essential. With this additional information, further testing with computed tomography or magnetic resonance imaging, along with a venogram, may result in a definitive diagnosis of pelvic congestion syndrome to facilitate treatment.
Keywords
Introduction
Pelvic pain is a common occurrence among female patients and can be assessed with a physician’s order for a pelvic sonogram. In evaluating a patient who is experiencing chronic pelvic pain, especially if other pathologies have been ascertained, further detailed investigation and images should be acquired. Although these symptoms can be associated with many other pelvic disorders, pelvic congestion syndrome (PCS) needs to be considered as a possible diagnosis. This also needs to be a consideration no matter the age group, since this has also been noted in adolescents. 1 When dilated vessels are visualized during a transabdominal or transvaginal pelvic sonogram, specific and detailed images should be obtained during the sonographic examination. With the knowledge that these dilated vessels could indeed be the source of a patient’s pain, having an understanding of the specific images to obtain could contribute to an earlier diagnosis for the patient. This particular finding with sonography can also lead to additional diagnostics to further evaluate the source and treatment, such as embolization therapy.
There are many choices for obtaining the proper diagnostics; therefore, complex problem solving may be required when faced with an unusual pathology and the appropriate treatment choice. When investigating the imaging modalities used within the diagnostic process, there are specific advantages and disadvantages to each type of testing. A significant difference between sonography and other imaging modalities is that the quality and diagnostic yield are heavily based on the experience and knowledge of the sonographer. In the field of women’s health, there are so many types of syndromes, conditions, and disease processes that it is difficult to have knowledge of them all. A specific female pelvic syndrome that some sonographers may be unfamiliar with is PCS.
Pelvic congestion syndrome is a condition that is not well understood, and therefore, knowledge of this pathology is very limited and it is unknown to many sonographers. This disorder can be defined as the presence of ovarian and pelvic varicose veins and is associated with chronic, persistent pelvic pain for more than 6 months, even in the adolescent population.1–3 Veins are considered varicose when they are dilated beyond their normal measurement and generally form due to incompetence of the valves within the veins. These dilated pelvic vessels in a female patient can be compared with the varicoceles that can be visualized during a testicular sonogram. There are a number of factors that may play a role in the formation of the dilated veins found in PCS.
Dilated veins are an abnormal finding in any part of the body and are also referred to as venous insufficiency, venous incompetence, or venous reflux. This disease process occurs when the valves within the veins fail to work properly. Since the veins bring blood back to the heart, with proper valve function throughout the venous system, blood should travel in one direction. When these valves no longer work properly, for whatever reason, the blood will reflux backward and cause veins to become dilated and engorged. A number of factors can contribute to the dysfunction of valves within the venous system.
There are many contributing factors that can lead to incompetent veins in the pelvis including congenital factors, hereditary factors, pregnancy, pelvic pathology, or certain syndromes causing obstruction. Generally, PCS occurs in female patients of child-bearing age. When considering a congenital malformation, documented cases in adolescents as young as 13 years have occurred; therefore, PCS should be considered regardless of the patient’s age. One congenital anomaly to consider is the absence of the valves within the veins in the pelvis, which results in retrograde blood flow. 3 Heredity plays a major role in many conditions, including venous insufficiency within the pelvic vessels. Generally, when venous pressure is increased, due to pregnancy or an obstruction from pelvic pathology, valvular function can become dysfunctional, resulting in venous insufficiency. Two syndromes that also can be a contributor to PCS are nutcracker syndrome and May-Thurner syndrome.
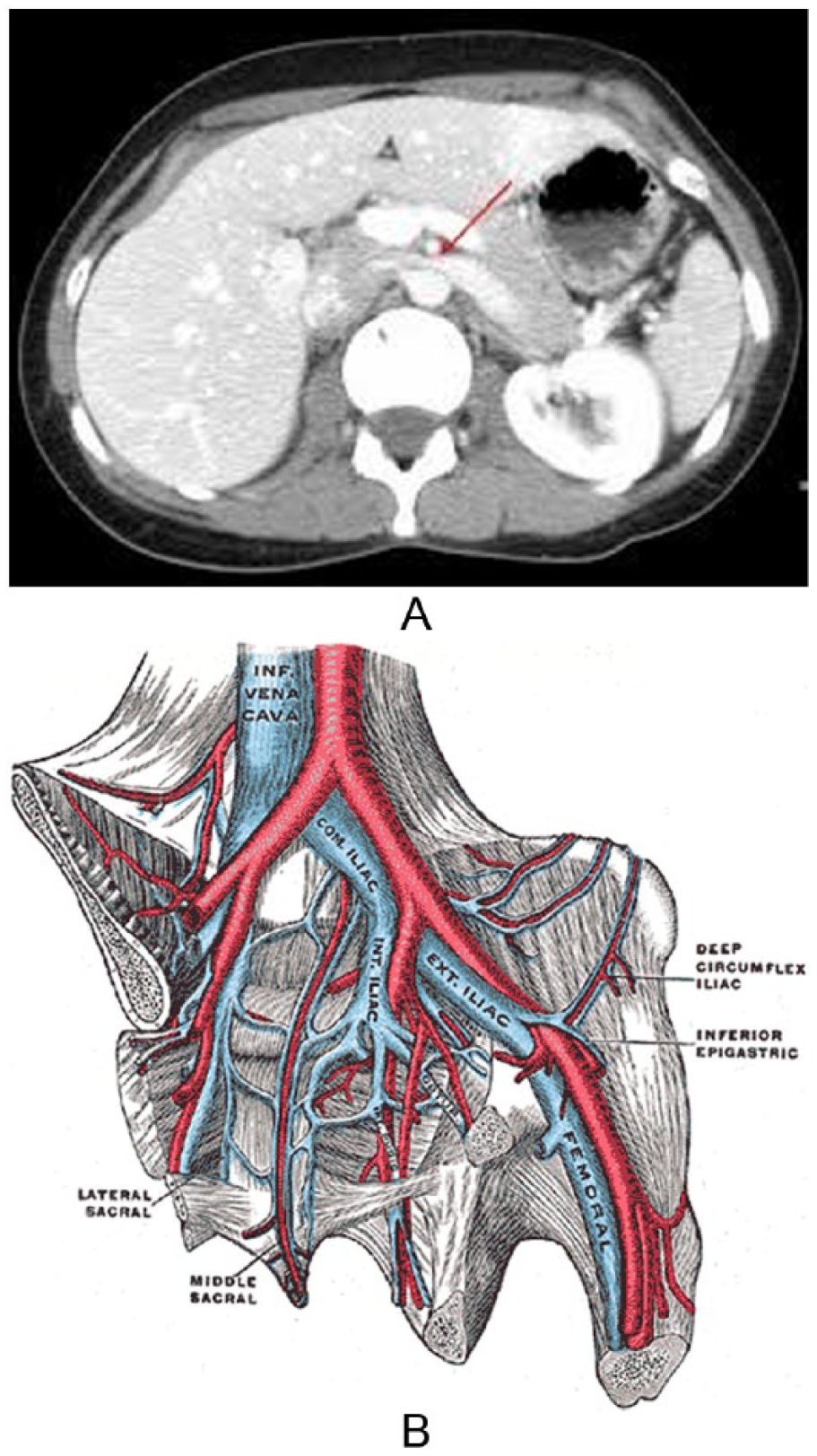
Nutcracker syndrome (Figure 1A) 4 is a condition in which the left renal vein is compressed by the abdominal aorta and the superior mesenteric artery, resulting in a variable degree of left renal vein obstruction. 5 Another condition that compromises the correct venous flow pattern is May-Thurner syndrome (Figure 1B). 6 In this anomaly, the left iliac vein is compressed by the right iliac artery and therefore causes venous obstruction. 7 Due to these types of obstructions, blood will reflux and eventually dilate the left venous system. This in turn will create the pelvic dilated vessels found in PCS. With the onset of these dilated, engorged vessels, certain clinical symptoms will gradually present themselves.
Patients will present with certain clinical findings and a number of possible symptoms may be present with PCS. Clinical findings can demonstrate gluteal, vulvar, and perineal varicosities, along with varicosities in the upper inner thigh of the lower extremity and ovarian tenderness on examination.7,8 Also, according to Koo and Fan, 8 when evaluating patient presentation of postcoital pain that is also combined with ovarian point tenderness, it has been reported to be 94% sensitive and 77% specific for the diagnosis of pelvic venous congestion. 8 In a recent study, there was a significant association between lower extremity varicose veins and patients with pelvic congestion. 9 The self-reported symptoms from the patient along with the clinical findings can aid in the correct diagnosis.
Patients with PCS may present with symptoms that include chronic pelvic pain, dull pelvic achiness, dysmenorrhea, dyspareunia, and menorrhagia. As noted, many of these symptoms also correspond to a number of other possible pelvic pathologies. With any type of imaging, it is vital to obtain a thorough and complete patient history, which can give critical additional information and expedite the problem-solving process. As with varicose veins in the legs, pelvic varicosity symptoms can worsen throughout the day, especially with prolonged standing, causing progressively worsening pelvic pain later in the day. Some temporary relief may be experienced with rest and leg elevation, making symptoms inconsistent.
Pelvic pain is one of the most common indications for a physician to order a transabdominal and/or transvaginal pelvic sonogram. Generally, when an indication for the evaluation of the pelvic organs is determined, the first imaging choice is a sonogram. There are a number of benefits, as well as limitations, in using sonography as the initial imaging modality. Besides being a noninvasive procedure, having no radiation exposure, and being widely available and accessible, sonography is also a less costly way for a possible definitive diagnosis. Some limitations in imaging for PCS can include patient size and body habitus, compression of dilated veins due to bladder filling during transabdominal sonography, and the supine position of the patient. This can be slightly adjusted with a reversed Trendelenburg positioning technique with a transvaginal sonogram, causing the incompetent vessels to engorge and dilate.
When performing any pelvic sonogram with an indication of pelvic pain, especially chronic pelvic pain, all pelvic structures need to be thoroughly evaluated, including the pelvic vessels. Generally, after other pelvic pathologies have been ruled out, PCS should be a consideration. 10 With the visualization of any dilated vessel, either in the adnexa, near the ovary, or near the uterus, continued investigative evaluation is warranted. This additional information, based on the classic sonographic findings of pelvic venous insufficiency, can indicate further evaluation and a definitive diagnosis of PCS.
If indications suggest PCS, further evaluation should be performed when pelvic varicosities are apparent. Classic sonographic findings can include dilated varicosities found within the pelvis, demonstrating reversal of blood flow and an increase in diameter during a Valsalva maneuver. 11 These dilated varicosities are generally an indication of this disorder, with a vessel diameter of greater than 4 mm. 11 Similar to imaging varicosities within a testicular sonogram, the Valsalva maneuver can also give additional information by demonstrating dilated veins enlarging and displaying reversed blood flow with color Doppler within the dilated pelvic veins (Figure 2). This can also be documented by obtaining spectral waveforms. Along with the standard pelvic sonographic images, additional clinical information can be added by including measurements, color Doppler, and spectral Doppler of the dilated vessels, pre- and post-Valsalva maneuver. Placing the patient in a reverse Trendelenburg position, if possible, can be helpful in demonstrating the engorged pelvic varicosities. As more awareness is brought to this disorder, further images could be added to the protocol. Although sonographic findings may indicate PCS, additional testing will reach a definitive diagnosis. These sonographic criteria, along with the patient’s clinical findings and symptoms, can lead to further testing to positively diagnose a patient with PCS. There are a number of other imaging modalities used to further evaluate for PCS.
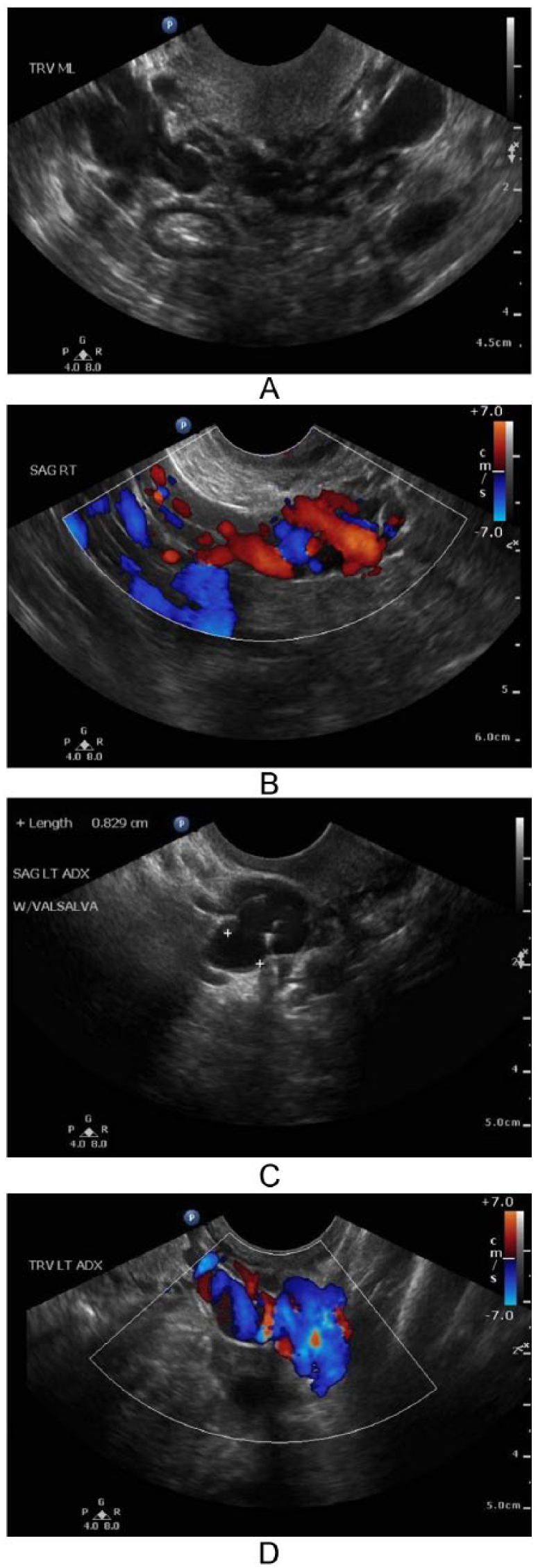
(A) Dilated pelvic veins found within the pelvis region are an indication of pelvic congestion syndrome. (B) Enlarged pelvic veins and significant reversed color Doppler flow with Valsalva maneuver noted. (C) Measurement of the enlarged vessel, demonstrated with Valsalva maneuver. (D) Demonstration of varicose pelvic vessels with color.
Since sonography can be limited due to patient body habitus as well as particular body regions that provide limited visualization, other imaging modalities may be helpful in providing a definitive diagnosis for the patient. These include computed tomography (CT), magnetic resonance imaging (MRI), and venography. Images from CT or MRI would also demonstrate an extensive overall view of possible sources for dilated vessels contributing to pelvic venous insufficiency. Additional findings, such as nutcracker syndrome or May-Thurner syndrome, as described earlier, may also be discovered, leading to potential variation in treatment. These are all very important factors when reviewing treatment options. As with any modality, there are advantages and disadvantages to consider when a physician is faced with choosing a particular imaging modality.
One significant advantage of using MRI over CT or a venogram is the use of non-ionizing versus ionizing radiation exposure. This is essential to keep in mind, since the majority of these patients are within child-bearing age. This is also a key factor when determining the best diagnostic options for any patient. Unnecessary exposure to radiation, which is cumulative in nature, should be avoided whenever possible. Availability and accessibility are a couple of disadvantages in using MRI when compared with the usage of CT. Cost is another important factor, since MRI is significantly more costly when compared with other imaging modalities.
Although MRI is an excellent diagnostic tool for pelvic venous insufficiency and allows a 3D evaluation of venous varicosities with reflux assessment, 12 a venogram is currently considered the gold standard for cases involving pelvic congestion. 4 This type of imaging is also used during the treatment process and can be accomplished at the time of the diagnostic imaging performed with venography. A venogram does rely on the use of ionizing radiation exposure to the patient being imaged. The pelvic images in Figure 3 demonstrate the contrast agent dispersing through the pelvic venous system. This also evaluates the dilated vessels to be considered for treatment and displays the incompetency of the vessels (Figure 3). 13
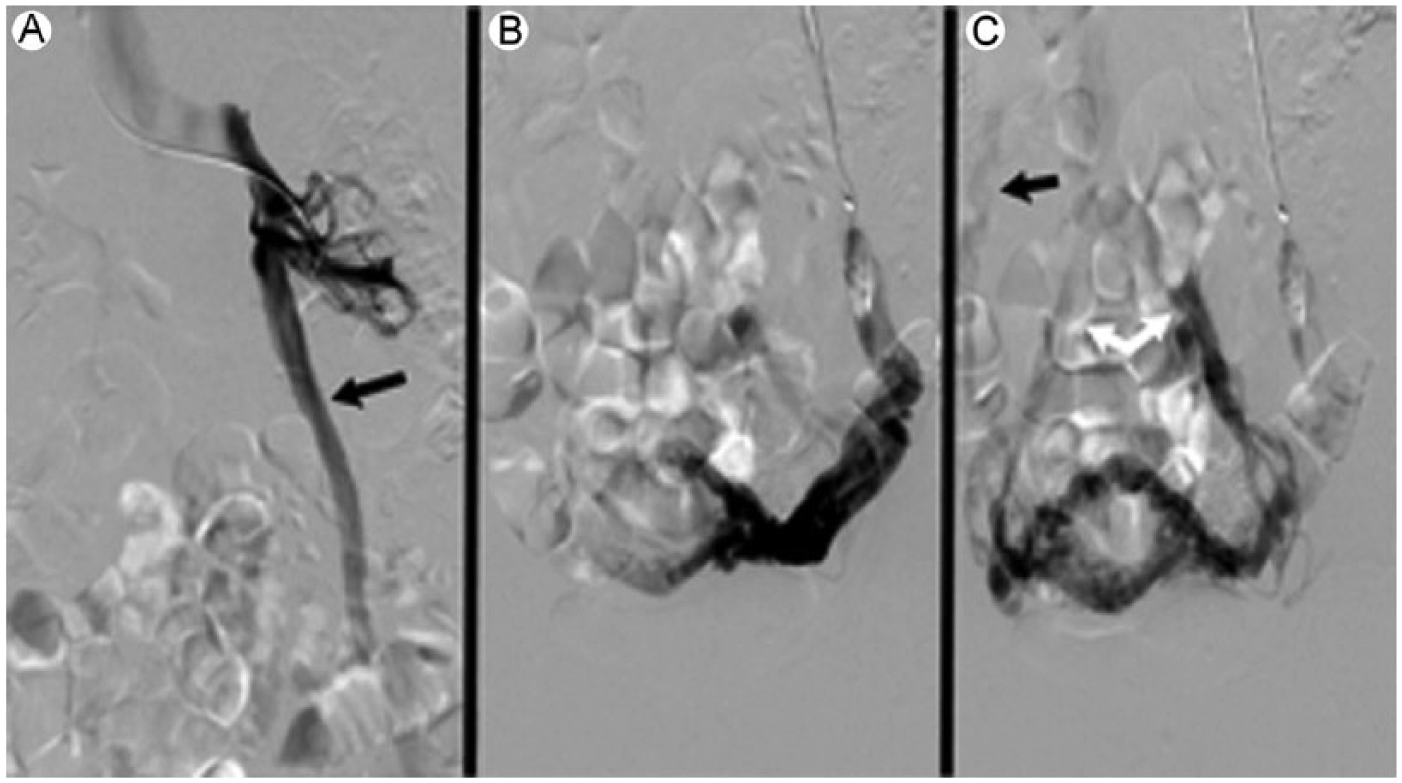
Venogram demonstrating the reflux in pelvic venous insufficiency. (A) Injection of the left renal vein demonstrating retrograde flow (black arrow). (B) Demonstrating uterine varicosities. (C) Varicosities into the right ovarian vein (black arrow).
Once the diagnosis has been determined, in a symptomatic patient, treatment options can be discussed and considered.
An invasive transcatheter embolization (Figure 4), 14 performed by an interventional radiologist, is the current standard used for treatment of PCS. This type of procedure has several options for successful occlusion of the vessel. These include coils, glue, or a foam or liquid consisting of a sclerosing agent. 2 Embolization has been used as a very successful form of treatment for patients with PCS. According to a study performed by van der Vleuten, van Kempen, and Schultze-Kool, 2 96% to 100% of the embolization cases were successful, with improvement of symptoms in 67% to 89% of the patients after their procedure.
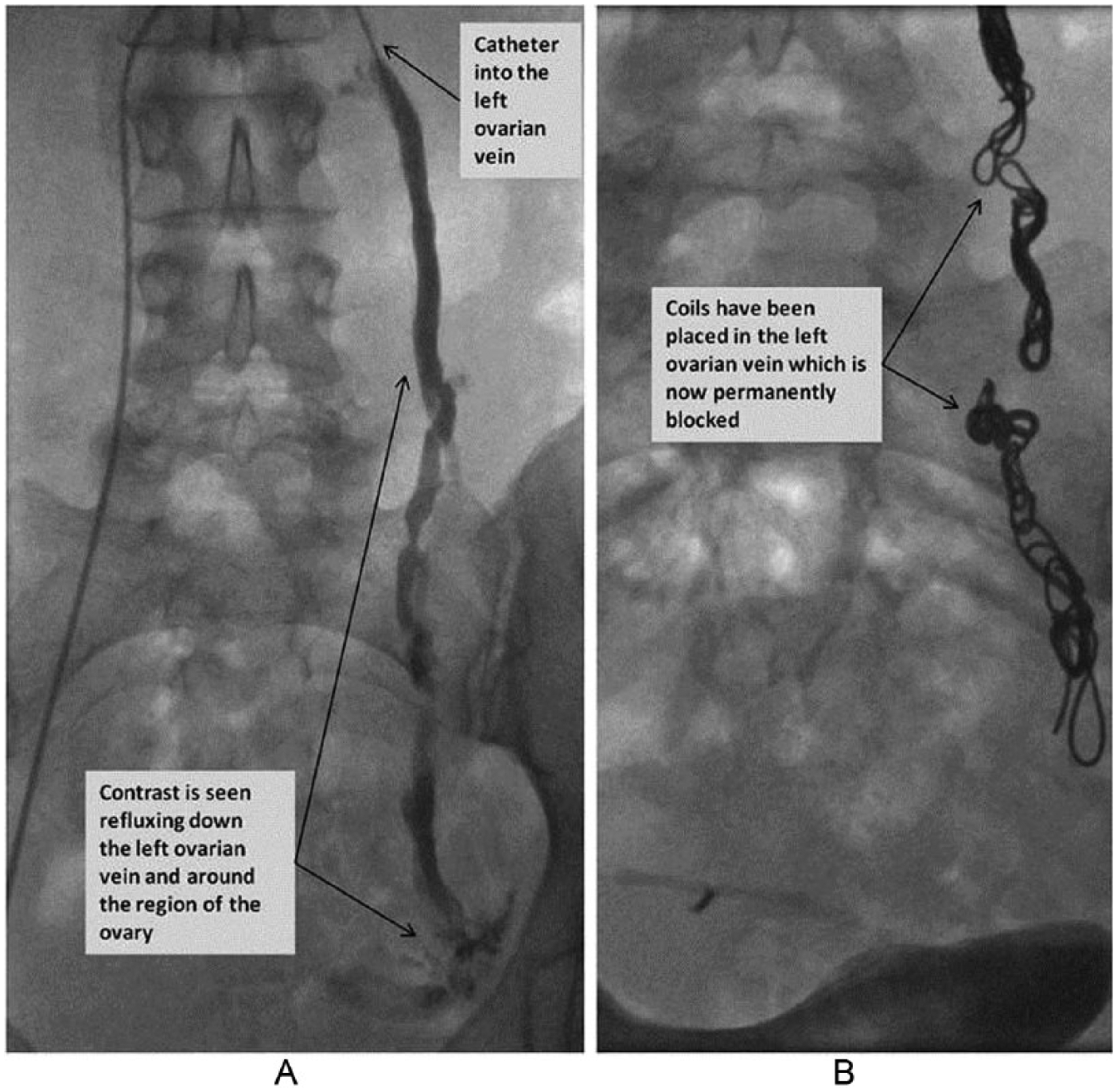
(A) The catheter is seen within the left ovarian vein (top thin black arrow). The contrast agent is seen refluxing down the left ovarian vein (thin black arrows). (B) This has been successfully embolized (permanently blocked) with coils (thin black arrows). See http://www.bsir.org/patients/pelvic-venous-congestion-syndrome/#pelvic-venous-congestion-syndrome.
Conclusion
Pelvic congestion syndrome is a disorder that is not well known and therefore can be diagnostically missed. With a better understanding of this condition, a properly recorded set of patient symptoms, and high-quality sonographic images, sonographers can greatly assist a symptomatic patient with chronic pelvic pain to an earlier diagnosis. Additional imaging with CT or MRI can confirm pelvic venous insufficiency, along with the source of the disorder, so treatment options can be reviewed and discussed. Earlier detection of PCS, along with successful treatment, can lead to a patient’s relief of these chronic symptoms.
Footnotes
Acknowledgements
The author would like to thank Professor Tammy Stearns at Adventist University of Health Sciences for her invaluable knowledge of the varying modalities used throughout the diagnostic process. The author would also like to give a special thank you to Neal Smith, Jr., MS, JD, at Adventist University of Health Sciences, for all of his assistance with acquiring the necessary permissions.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
{kind=link}