
Abstract

Introduction
Pelvic venous reflux (PeVR) is a condition that can cause chronic pelvic pain (CPP). It is surprisingly common, but the condition often goes unrecognized during evaluation of women for CPP. The diagnosis can be made by a specialist familiar with PeVR, who can then educate the patient about the condition and about the various treatment options.
What is chronic pelvic pain?
CPP is defined as constant or intermittent pelvic pain persisting over at least 6 months. CPP is common worldwide, accounting for up to 10% of visits to a gynecologist. 1 While it can occur in women at any time of life, it impacts up to one in six women of child-bearing age. 2 The impact of CPP on quality of life including work, leisure activities, and relationships may be substantial. Costs in lost productivity and medical care are estimated to be over US$3 billion per year in the United States. 2 There are many causes of CPP, including endometriosis, fibroids, urinary or bowel conditions, and disorders of the pelvic veins.
What is pelvic venous reflux (PeVR)?
Veins are the blood vessels that carry blood from the body back to the heart. When the valves in veins of the pelvis and the ovaries are not functioning, or the veins have a blockage (obstruction), the blood can flow away from the heart and pool in the pelvic veins. This flow in the wrong direction is known as reflux. As pressure builds up in the pelvic veins, they become dilated. Although in many women this causes no symptoms, in other women PeVR can cause CPP. PeVR is the second most common cause of CPP, following only endometriosis. 3
What is pelvic congestion syndrome?
The term pelvic congestion syndrome was coined in the 1940s by Dr HC Taylor. 4 Historically, the proposed causes included wearing tight corsets and other garments, as well as emotional instability. Our understanding of the causes of pelvic venous disorders has come a long way since that time, and we know now that pelvic veins may become dilated and cause symptoms because of obstruction, reflux, or a combination of both. Two types of venous obstruction include compression of the vein draining the left kidney (called the ‘nutcracker syndrome’) and the vein(s) draining the legs (called iliac vein compression or May–Thurner syndrome). The term pelvic congestion syndrome, although commonly used, is overly simplistic, and many experts in the field believe it should be abandoned in favor of using the term pelvic venous disorders. 5
What are the symptoms of PeVR?
Many women with PeVR have no symptoms. It is estimated that on imaging tests (such as computed tomography [CT] scans of the abdomen/pelvis) done for other reasons, up to 47% of women have pelvic varicosities. 6 It is not clear why some women with PeVR have pain, while others do not. A similar scenario exists with varicose veins in the leg—some men and women with varicose veins have pain, swelling, and other symptoms, while others have no symptoms. PeVR can cause dilated veins with symptoms in the pelvis, vulva (area around the vagina), leg, or all three locations.
Pelvic symptoms
Pelvic symptoms may include CPP with heaviness, aching, or fullness. Women may have pain with intercourse, which often occurs after intercourse and may take hours to resolve. Women may urinate frequently or have increased pain with prolonged standing or after exercise. The symptoms are almost always worse during the menstrual period (menses). 7
Vulvar symptoms
Some women with PeVR have bulging veins in the vulva and labial area. Hemorrhoids are often present as well. Women with vulvar varicose veins may or may not have pelvic symptoms. Typical vulvar symptoms include heaviness, aching, throbbing, and itching. Vulvar varicose veins often occur during a woman’s second or third pregnancy and often improve after delivery. As with the pelvis, symptoms are often worse during menses.
Leg symptoms
PeVR can extend from the vulvar area into the legs. Symptoms are similar to varicose veins in the leg that are not coming from the pelvis (heaviness, aching, swelling, throbbing, and itching). The pattern of varicose veins is usually different from non-pelvic varicose veins, and the symptoms tend to be cyclical and worse during menses or after exercise. Figure 1 shows three common patterns for varicose veins of the leg that are due to PeVR.
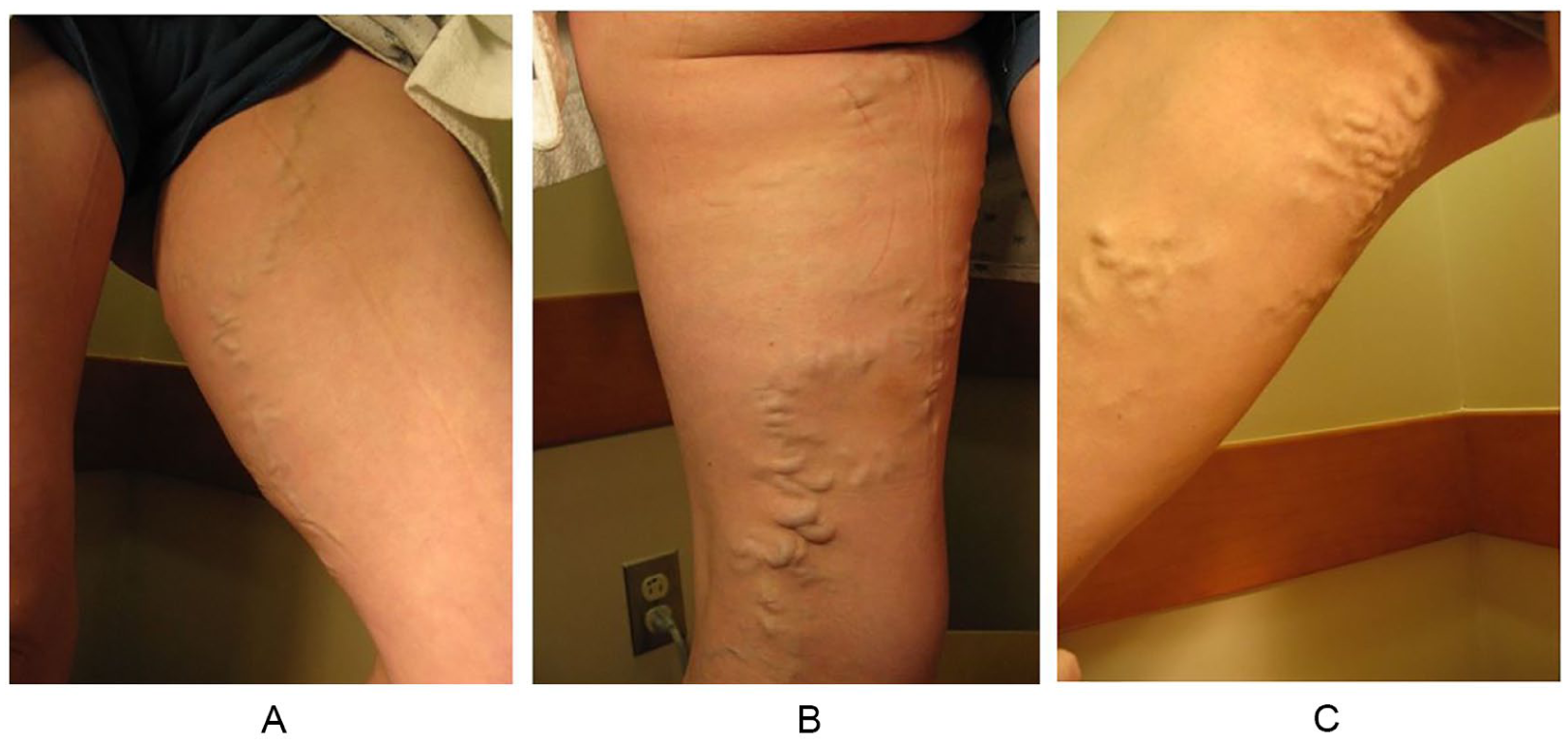
Three common patterns of pelvic-derived varicose veins of the leg: (A) anterior (front) pattern; (B) posterior (back of leg) pattern; and (C) medial (side of leg) pattern.
What are the risk factors for PeVR?
Symptoms of PeVR usually occur in women of childbearing age. Symptoms often improve after menopause. The symptoms typically appear after at least two pregnancies, and if dilated pelvic veins are found in a woman with no history of pregnancy, other causes should be considered (such as venous obstruction/blockage). During pregnancy, the weight of the uterus puts pressure on the pelvic veins, which also dilate due to hormonal factors. Blood flow to the pelvis during pregnancy increases up to 60-fold. 3 These changes often reverse after pregnancy, but in some women dilated veins remain and can cause symptoms. One study showed that compared to women of the same age, women with PeVR tended to be thinner and to have had infants with heavier birthweights. 8
How is PeVR diagnosed?
The first step in the diagnosis of PeVR is a clinical history taken by a health care provider familiar with the disorder. The next step is an imaging study to look at the veins in the abdomen, pelvis, and sometimes the legs. The type of study ordered depends on local and regional expertise. Imaging studies for PeVR include ultrasound, either with a probe placed on the abdomen (transabdominal) or inside the vagina (transvaginal), CT scans, magnetic resonance imaging (MRI) scans, or a study called venography in which contrast dye is directly injected into veins. All of these imaging studies can show abnormal dilated veins. The left ovarian vein is the most common vein to become dilated. The right ovarian vein can also be abnormal, as can veins draining from the pelvis known as the internal iliac veins. Venous compression or obstruction can also be present and can mimic symptoms of PeVR, which should be assessed by the imaging study. Figure 2 shows examples of a transabdominal ultrasound, a CT scan, and a venogram showing PeVR.
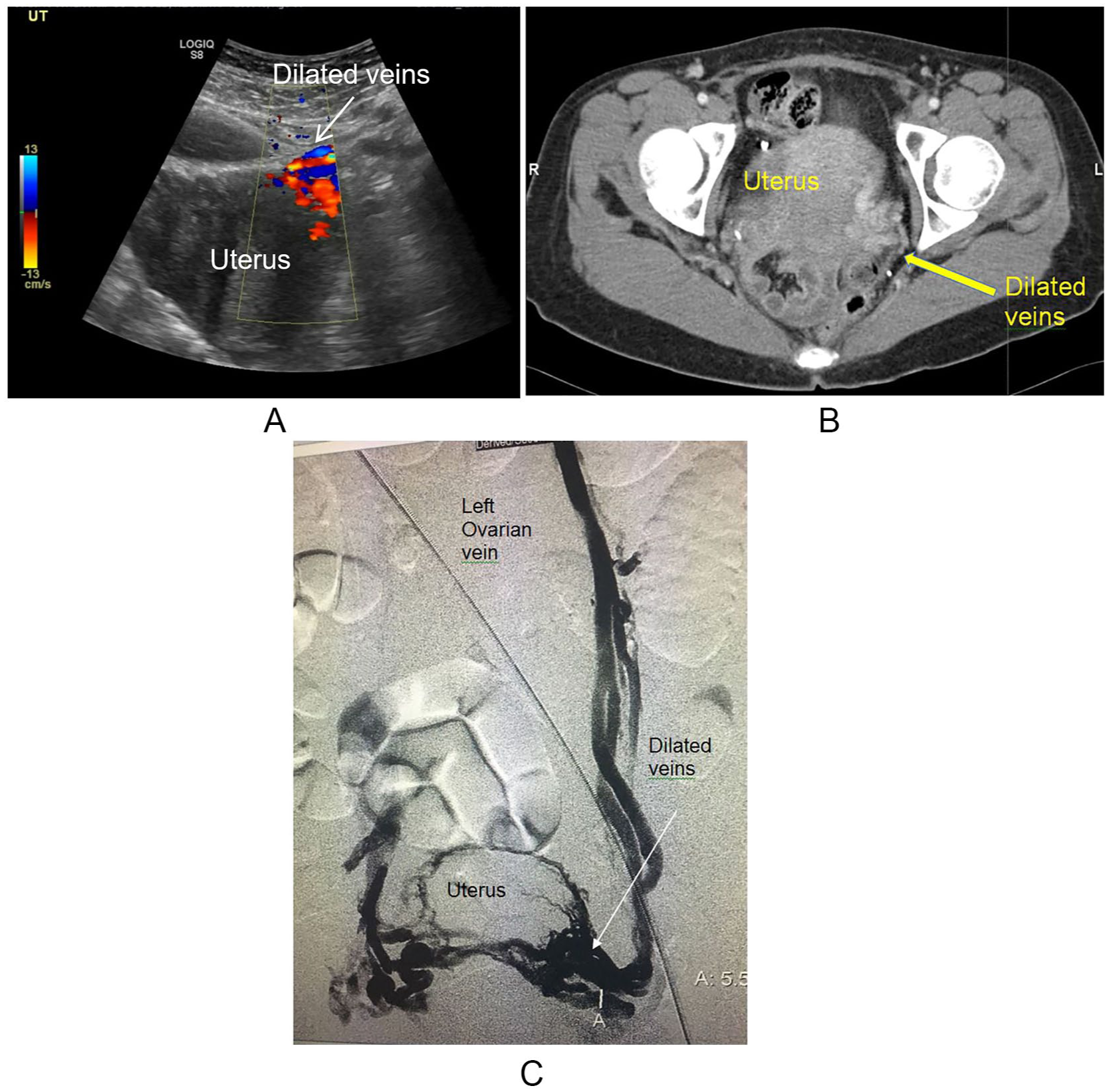
(A) Transabdominal ultrasound, (B) CT, and (C) venography images of PeVR with dilated veins (arrows).
What type of specialist treats pelvic vein disorders?
Specialists most familiar with pelvic venous disorders include some obstetricians/gynecologists, vascular medicine doctors, vascular surgeons, and interventional radiologists. Typically, treatment involving a procedure will be performed by a vascular surgeon or interventional radiologist.
How is PeVR treated?
Treatment options for PeVR range from no treatment or medical management to interventions to close the abnormal veins. Some providers have even advocated for hysterectomy, although many physicians treating this disorder feel that option is not warranted as it removes organs (the uterus and sometimes the ovaries) that are not causing symptoms and it does not always remove the painful veins. If the symptoms of PeVR are mild and not affecting quality of life, reassurance and no treatment may be the best plan. Although PeVR can have negative effects on many patients, it is not life-threatening, and the symptoms often improve or resolve after menopause. 8 Any potential benefit of treatment therefore must be balanced against the success rates and risks of treatment. Medical management of PeVR includes over-the-counter pain medication such as acetaminophen or non-steroidal anti-inflammatory agents (NSAIDs) like ibuprofen. As the symptoms are affected by hormones such as estrogen, treatment with hormone-suppressing agents (e.g. medroxyprogesterone acetate (MPA), or goserelin) may offer some relief, but it is often not sustained and can have unwanted side effects.3,9
How is PeVR treated in patients with chronic pelvic pain?
In the past, open surgery was sometimes used to treat PeVR, but now treatment is usually a minimally invasive outpatient procedure that closes the abnormal veins. The most common procedure to treat PeVR is called embolization. It is performed by reaching the pelvic veins through a catheter (tube) placed in the vein of the neck or in the groin under local anesthetic and then injecting a medication to close the veins (sclerotherapy), or placing soft metal coils or plugs in the veins (coil embolization), or both. The treating physician will first verify the diagnosis with venography and rule out venous compression as a cause of symptoms. Both ovarian veins and internal iliac veins and their branches will be examined (Figure 3). The procedure is typically performed as a same-day or outpatient procedure and may be done with just a local anesthetic, a local anesthetic with sedation, or a general anesthetic. After the procedure, patients may feel heaviness or cramping in the pelvic area for several days. It may take a number of months or several menstrual cycles for patients to feel a full benefit from the procedure. Complete or partial improvement of symptoms after coil embolization and sclerotherapy of pelvic veins ranges from 68% to 100% in various studies that have looked at patient outcomes. 10
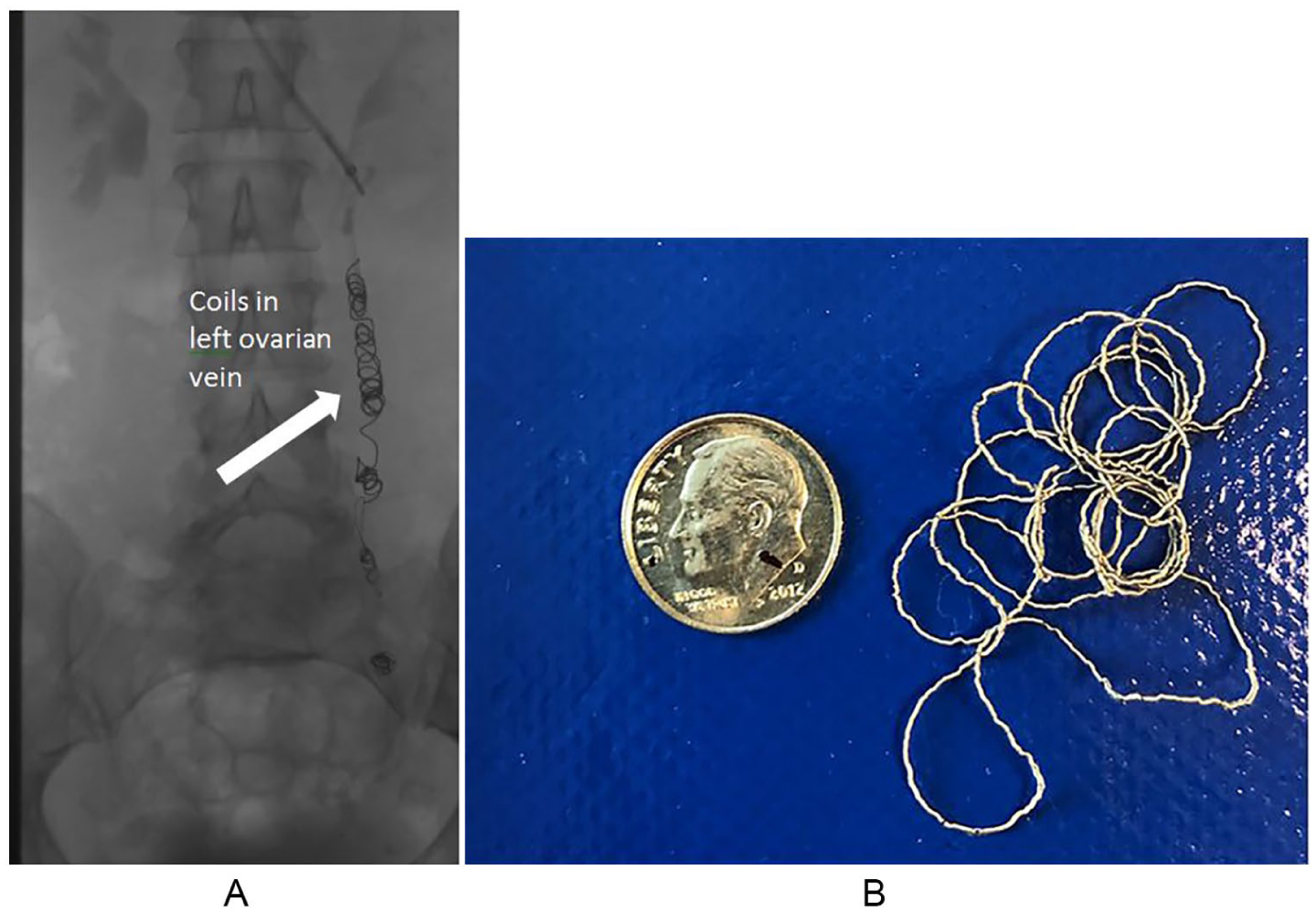
(A) An X-ray after coil embolization and (B) an embolization coil (to scale with a dime).
How is PeVR in the vulva and leg treated?
Many women with vulvar and leg varicose veins have no internal pelvic pain, and the symptoms are limited to the vulva and legs. In these cases, the symptomatic veins in the vulva and leg can usually be treated directly, leaving the veins inside the pelvis alone. Treatment of the veins inside the pelvis can be performed at a later date if the patient does not improve with direct treatment of the leg or vulva varicose veins, or if they develop pelvic pain. Vulvar and leg varicose veins can usually be treated with injection of a medication into the abnormal veins using ultrasound guidance and very small needles. This medication causes the veins to shrink in size and eventually close up and go away. This is a procedure known as sclerotherapy and can be performed in an office setting. On some occasions, if the veins are very large, they may need to be removed through small incisions in the skin, a procedure called microphlebectomy. Figure 4 shows images of a patient with vulvar and upper thigh varicose veins before and 3 months following treatment with ultrasound-guided sclerotherapy.
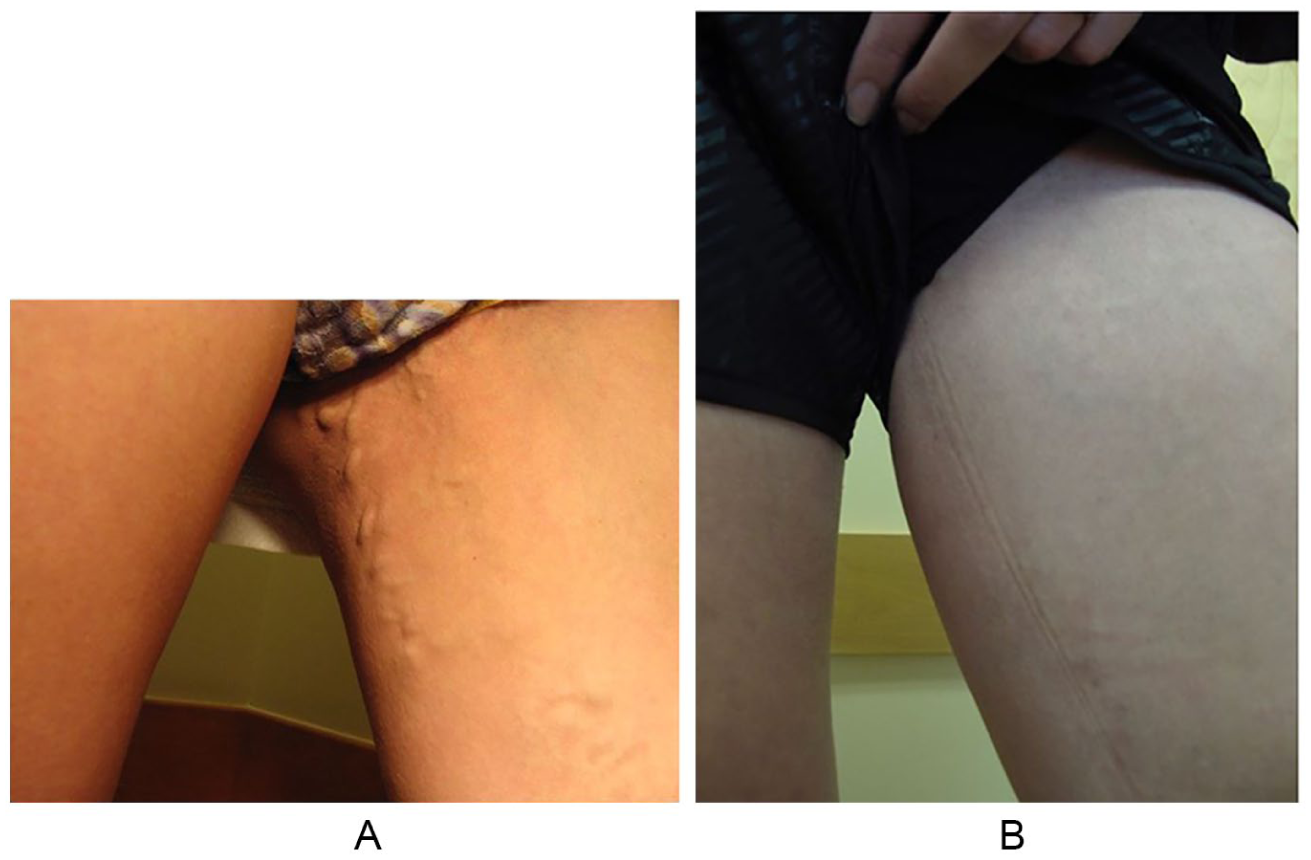
Pelvic-derived varicose veins of the vulva and upper thigh before (A) and 3 months after (B) ultrasound-guided foam sclerotherapy.
What are the potential complications of treatment?
Treatment of PeVR is generally very safe, but all invasive procedures have potential complications. Uncommon complications have included localized vein inflammation, bleeding, bruising, blood clots, movement of coils, or allergic reactions to the medications used to close the veins or to the contrast agents used to visualize them. It is important for patients to let their physician know of any allergies or sensitivities to medications or to metals. Patients who have been treated with metallic embolic coils or plugs can generally safely have magnetic resonance imaging (MRI) scans in the future, but the coils can cause ‘artifact’ on the images that may make them more difficult to interpret.
What can be expected in the long-term after treatment? Will the problem return?
Varicose veins in the pelvis, vulva, and legs can recur after treatment, especially after a subsequent pregnancy. Symptoms may reoccur due to progression of venous disease, or if the veins were not completely treated. Recurrence rates range from 5% to 25%. 10 If patients have recurrent symptoms, they can undergo retreatment if necessary. Fortunately, long-term outcomes for most women are favorable, and symptoms of PeVR usually improve or resolve with menopause.
Summary
PeVR (formerly pelvic congestion syndrome) is one of the most common causes of CPP in women of childbearing age. With proper clinical evaluation and treatment of PeVR, improvements in quality of life are typical. Recognition of this disorder by primary care physicians and obstetricians/gynecologists can help in the referral of these women in a timely manner to physicians with expertise in its diagnosis and treatment.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The ‘Vascular Disease Patient Information Page’ is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.