
Abstract
Aim: To determine the prevalence of cholelithiasis in a Nigerian population. Subjects and Methods: A cross-sectional study of Igbo adult subjects in Nnewi, Nigeria, was conducted from June 2011 to April 2014. A sample of 3501 adult subjects’ gallbladders and associated biliary systems was evaluated by sonography, and the presence or absence of cholelithiasis was documented. The age and anthropometric variables of the subjects were recorded. Results: The subjects (18-92 years) comprised 1731 men (49.4%) and 1770 women (50.6%). Only 4.4% (n = 154) had cholelithiasis. It is more common in women than men, at a ratio of 2.8:1. It is also more common in subjects with a high body mass index. Conclusion: The prevalence of cholelithiasis among the Igbo people in Nnewi is 4.40%, and it is about three times more common in women than men.
Biliary diseases, especially cholelithiasis, are a major cause of right-upper-quadrant (RUQ) abdominal discomfort or pain. The gallbladder is quite amenable to sonographic evaluation, because the large accumulation of bile after a fasting period makes it easy to locate and identify any pathology. RUQ abdominal pain, a common symptom of cholelithiasis, is the most common indication for an RUQ abdominal sonogram. 1 Cholelithiasis always begins insidiously, remaining asymptomatic for long periods and possibly causing life-threatening complications if not detected and treated appropriately. 2
The unmodifiable risk factors for cholelithiasis include ethnic background, increasing age, female sex, and familial history or genetics. 3 The modifiable risk factors include a “Western type” diet (characterized by overnutrition with refined carbohydrates and reduced intake of dietary fiber), obesity, decreased physical activity, rapid weight loss, and use of oral contraceptives.3,4 Other risk factors include pregnancy and parity, drugs (e.g., ceftriaxone, octreotide, thiazide diuretics), total parenteral nutrition or fasting, and bariatric surgery. 4 Diseases are also risk factors, such as liver cirrhosis, type 2 diabetes, metabolic syndrome, dyslipidemia, nonalcoholic fatty liver disease, chronic hemolysis, ileal Crohn’s disease, cystic fibrosis, biliary infection, infestations, and chronic hepatitis C. 4 Childhood cholelithiasis, once considered rare, is becoming increasingly common due to the same risk factors as in adults, particularly obesity. 3 Additional risk factors include reduced antinucleating factors and gallbladder hypomotility, which, along with mucin, may contribute to aggregation of crystals and hence to the formation of gallstones. 5 Epidemiologic studies have reported that the incidence of cholelithiasis varies among populations.3,6,7 Other reports suggest that genetic and dietary factors may be responsible for population-specific differences in incidence of cholelithiasis.8–10 It is therefore imperative that prevalence rates are established for different populations, since the incidences of cholelithiasis vary from population to population, being influenced by genetic characteristics and the prevailing environmental factors. The availability of reliable epidemiologic statistics on cholelithiasis for a population can assist clinicians and sonographers to determine whether cholelithiasis is present with RUQ abdominal pain. Clinicians and sonographers in Nnewi and surrounding communities rely on data obtained from Caucasian as well as other African populations, owing to the lack of epidemiologic data on cholelithiasis in adult Nigerians in Nnewi. The locality appears to have been neglected in epidemiologic studies of cholelithiasis presumably because of the nonavailability of tertiary health care institutions until the 1990s.
This study therefore investigated the prevalence of cholelithiasis among adult subjects in Nnewi, Nigeria. It also investigated the influence of anthropometric characteristics on the prevalence of cholelithiasis in the locality.
Subjects and Methods
This was a prospective cross-sectional study that targeted the adult population of Igbo ethnic extraction in Nnewi, Nigeria. The population of Nnewi is predominantly made up of the Igbo people, who are much easier to access than the other ethnic groups. The research design and protocol were approved by the Human Research and Ethical Committee, Nnamdi Azikiwe University Teaching Hospital, Nnewi. The participants consisted of volunteers who expressed willingness to take part in the study at the time that they were approached for enlistment. The study was conducted between June 2011 and April 2014.
The minimum sample size of participants in the study was determined with the following statistical formula 11 :

where n = the desired minimum sample size, Z = 1.96 at the 95% confidence interval, and p = estimated population proportion. Since this proportion was not known for the target population, a value of 50% (i.e., 0.5) was assigned to obtain the maximum value for p. In addition, d = the absolute precision required on either side of the proportion = 5% (0.05); therefore,

A minimum sample size of 384 participants was calculated, but 3501 subjects were included to increase the validity of the study.
The selection of prospective participants was done by the cluster sampling technique. The clusters (i.e., where the participants were selected) include the Uruagu, Umudim, Otolo, and Nnewichi communities, which make up Nnewi. The participants were approached to enroll in the study in various public places, such as churches, neighborhood markets, and schools. The selection criteria were as follows:
a subject must be of Igbo ethnic origin and residing in Nnewi at the time of the study;
a subject must be ≥18 years old; and
a subject must willingly consent to participate in the study.
Sonography of the Gallbladder and Data Collection
Informed consent was sought and obtained from each participant prior to enrollment in the study. Each selected subject, after an overnight fast, underwent RUQ abdominal sonography to determine the presence or absence of gallstones. Sonography was conducted in a makeshift cubicle, with a portable Kaixin KX 2000G ultrasound scanner equipped with a 3.5-MHz curvilinear transducer. The scanner was manufactured by Xuzhou Kaixin Electronic Instrument Company Limited, Jiangsu, China. A basic scanning protocol described by Sanders 1 was adopted and used for each subject. Each subject was laid supine on a mobile examination couch and coupling gel applied to the RUQ. The depth of the scanner was set such that the posterior wall of each gallbladder examined was satisfactorily demonstrated. The gallbladder was first examined with each subject in the supine position. Then, the long axis view was obtained by varying the obliquity of the transducer until the maximum length of the gallbladder was in view. This was followed by scanning the short axis of the bladder starting from the neck and sweeping through the fundus. More caudal angulations through the body demonstrated the entire fundus. The procedure was repeated with the subject in the decubitus, prone, and upright positions to ensure a holistic evaluation of the gallbladder.
A normal gallbladder was identified as one with its lumen distended with echo-free bile, as shown in Figure 1. The presence of cholelithiasis was identified as echogenic debris in the gallbladder lumen, with or without posterior acoustic shadowing (see Figure 2). Precaution was taken not to interpret a shadow cast by a rib segment over the gallbladder as emanating from a stone in the gallbladder. Shadowing attributed to a rib usually originates from outside the gallbladder lumen, as shown in Figure 3. Evidence of comorbidity with cholecystitis was identified as thickening of anterior gallbladder wall, usually >3.0 mm, with or without a halo of edema. Symptomatic presentation of cholelithiasis was classified as the presence of a gallstone in subjects with concurrent pain in the RUQ of the abdomen.

Sonogram of a normal gallbladder.
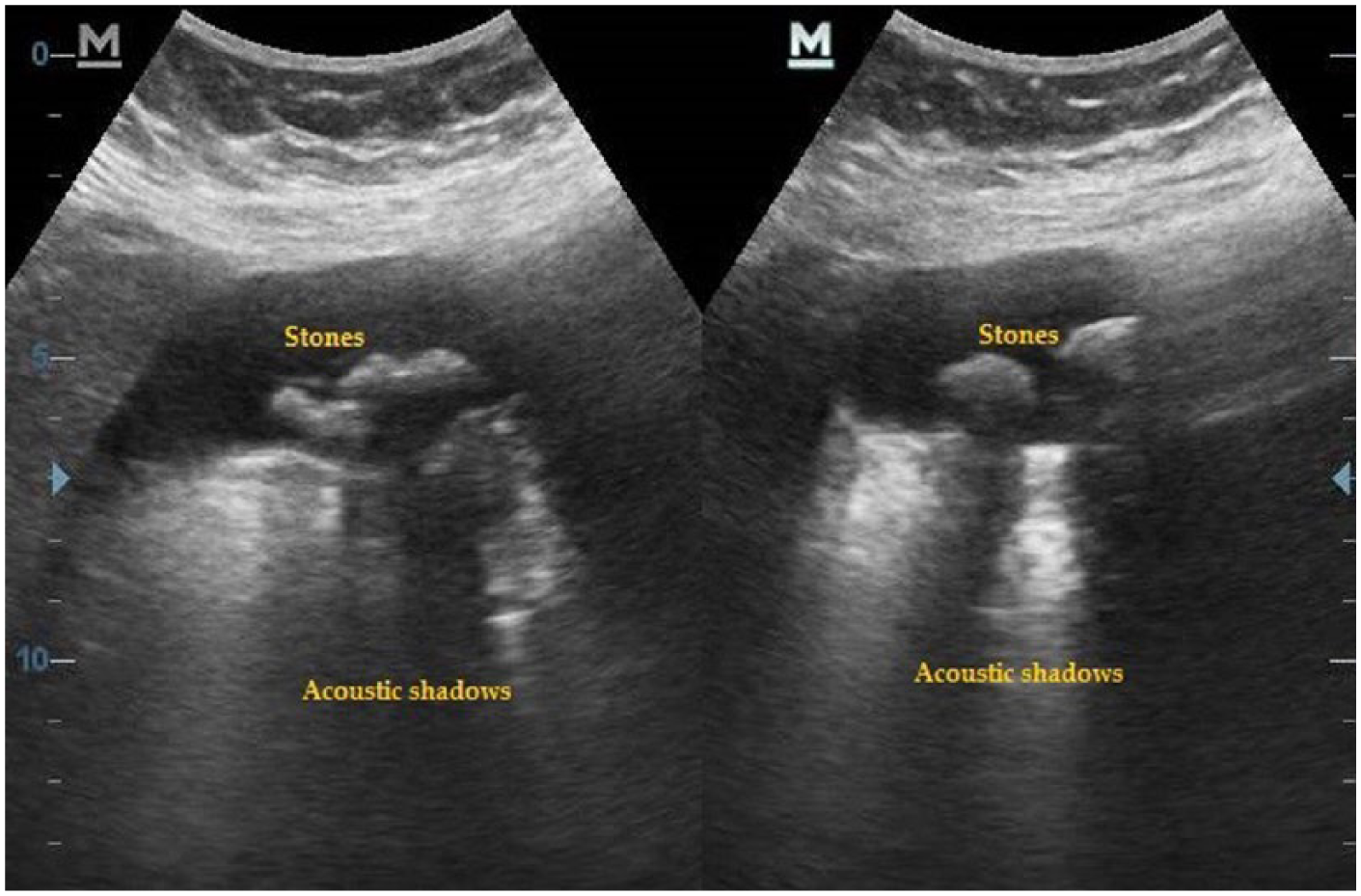
Sonogram of a gallbladder with multiple shadowing echogenic stones.
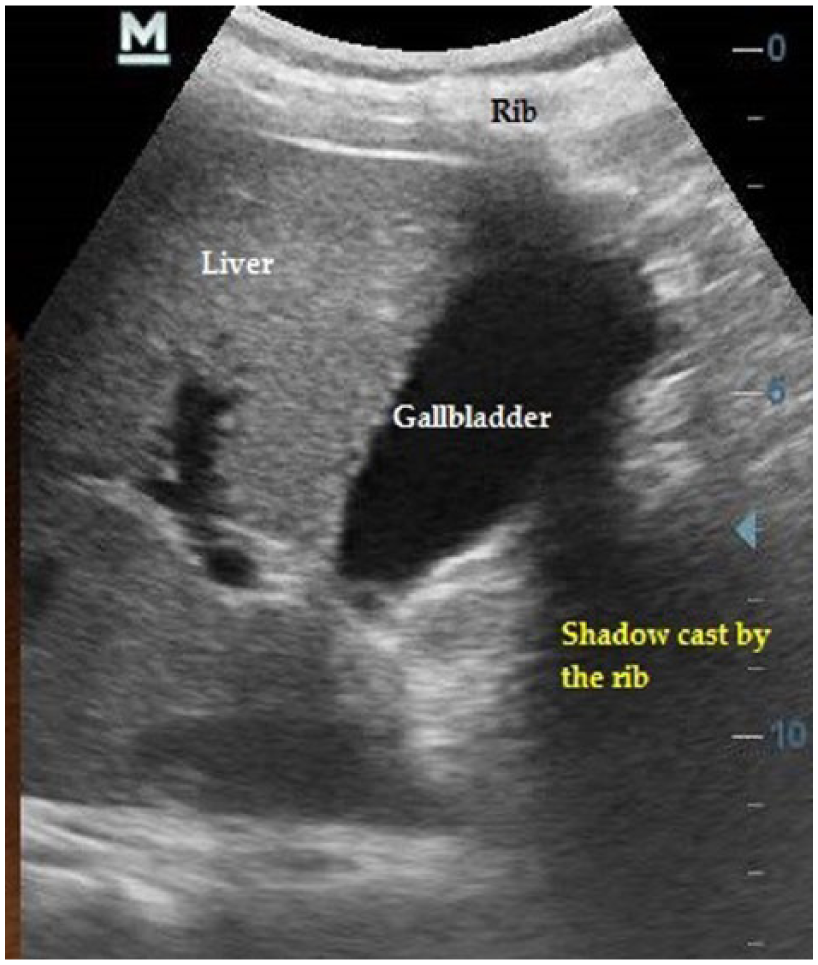
Sonogram of a normal gallbladder with a rib casting shadow over it.
Each subject was weighed with a well-calibrated weighing balance (Herson Emperos, China). It is graduated in a 0.1-kg (0.22 lb) interval and capable of weighing up to 120 kg (265 lb). The weight was measured with the weighing balance placed on a level ground and the patient standing barefooted and wearing light clothes. The height was measured with a well-calibrated meter rule, with the patient standing in the Frankfurt position and with head apparel removed. The age of each subject was obtained from his or her birth certificate and recorded in the data capture sheet.
Data Analysis
The body mass index (BMI) of each subject was calculated with the following formula: weight (kg) / height2 (m). Statistical analysis was done with SPSS 20.0 (SPSS Inc., Chicago, Illinois). Descriptive and inferential statistics were calculated. Gallstone incidence according to sex, age, and BMI was analyzed with descriptive statistical tools and presented in frequency distribution tables. Statistical significance was considered at P < .05 for inferences.
Results
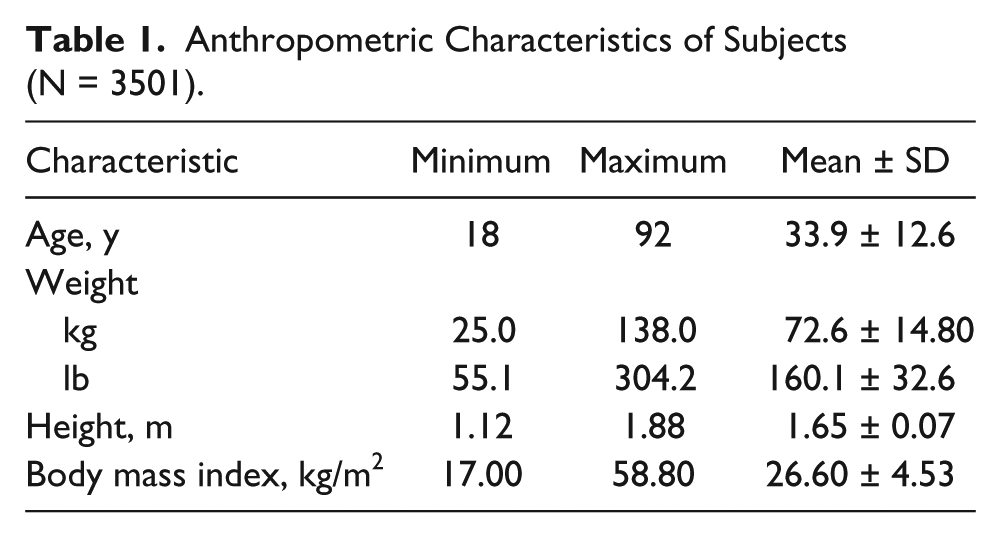
A total of 3501 subjects were evaluated in this study (n = 1770 women, 50.6%; n = 1731 men, 49.4%). The minimum age was 18 years, and the maximum was 92 years, with a mean of 33.88 ± 12.60 years (Table 1). The minimum and maximum weights were 25.0 kg (55.1 lb) and 138.0 kg (304.2 lb), respectively, with a mean value of 72.6 ± 14.80 kg (160.1 ± 32.6 lb); height ranged from 1.12 to 1.88 m, with a mean of 1.65 ± 0.07 m; and BMI was 17.0 to 58.80 kg/m2, with a mean of 26.60 ± 4.53 kg/m2. The female subjects were made up of women with widely differing characteristics, as shown in Table 2. Only 13.7% (n = 242) of the women were still nulliparous at the time of the study.
Anthropometric Characteristics of Subjects (N = 3501).
Anthropometric and Obstetric Characteristics of the Women (n = 1770).
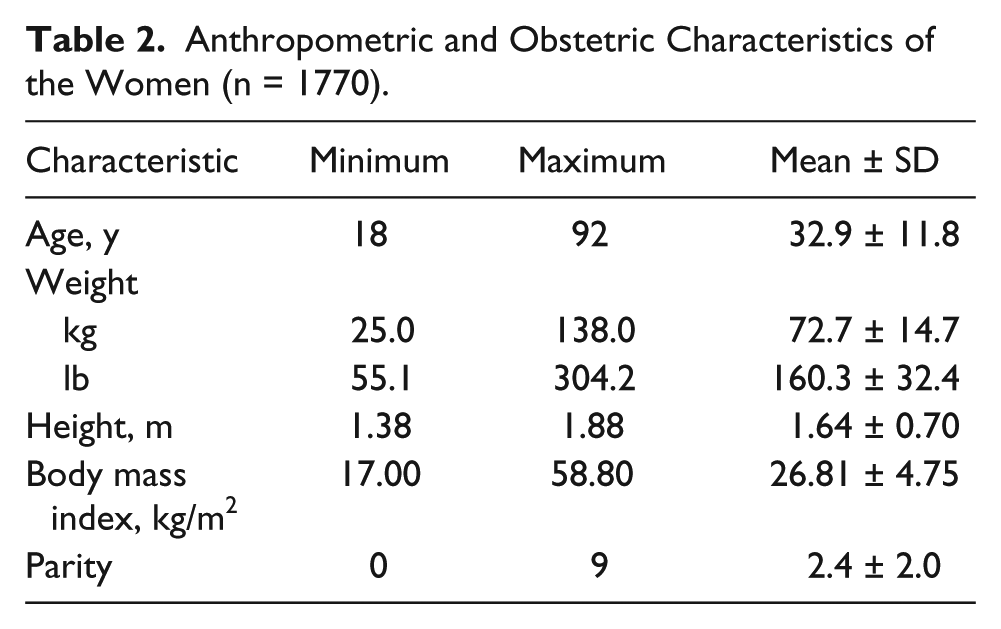
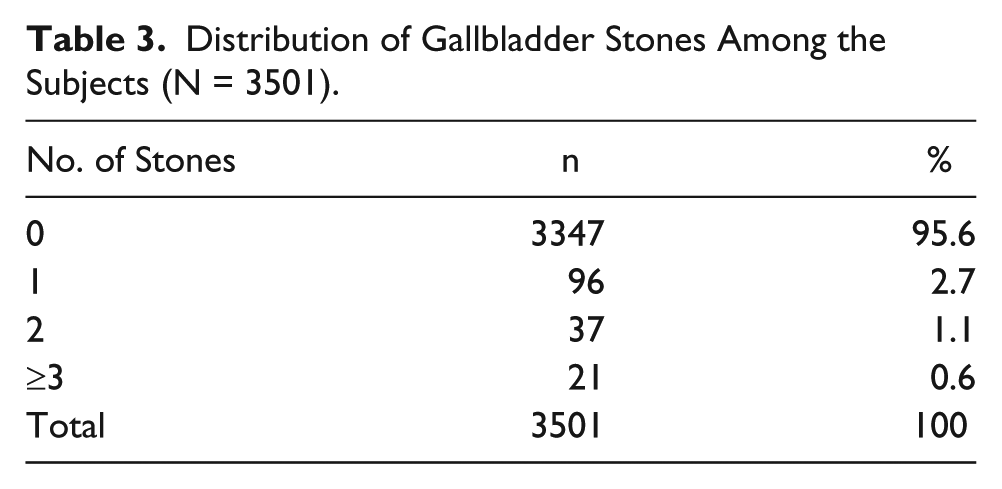
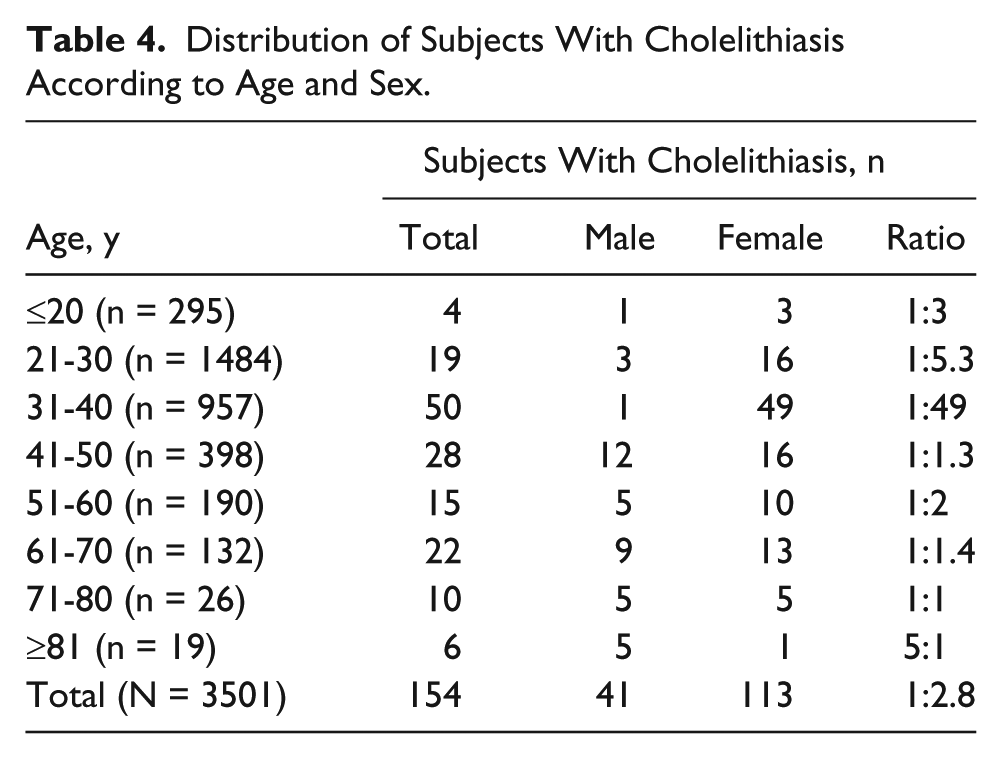
Table 3 shows that 95.6% (n = 3347) of the patients had no stones; 2.7% (n = 96), solitary stones; 1.1% (n = 37), two stones; and 0.6% (n = 21), three stones or more. Gallstone occurrence was least common among the subjects who were ≤20 years old and those >80 years old and most common in the 31- to 40-year age group (see Table 4). The study indicated that among the female participants, there was a significant (P < .05) link between parity and having cholelithiasis, as shown in Table 5.
Distribution of Gallbladder Stones Among the Subjects (N = 3501).
Distribution of Subjects With Cholelithiasis According to Age and Sex.
Frequency of Cholelithiasis According to the Parity of Female Subjects.
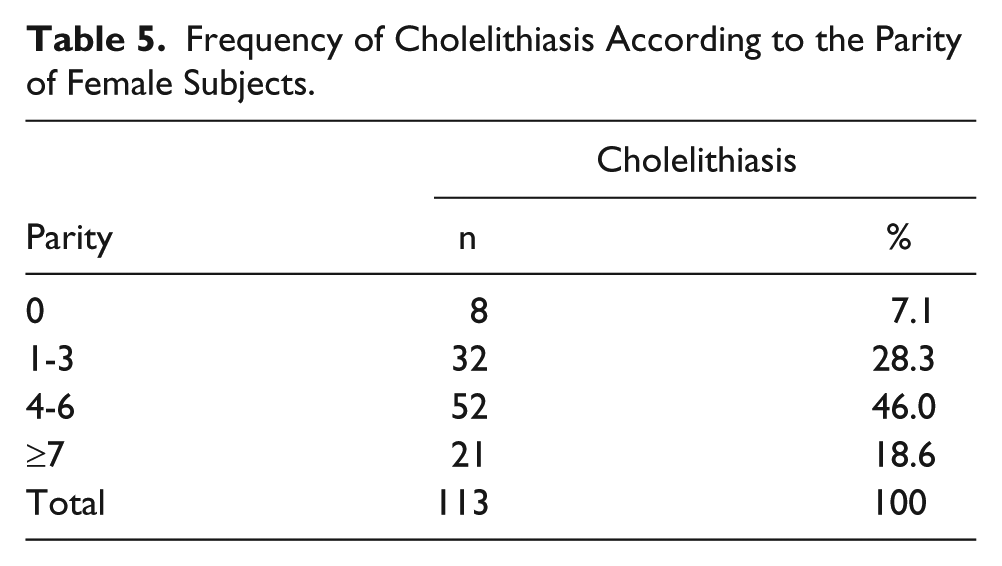
Table 6 shows the distribution of gallstones according to the sex and BMI of the subjects. In the 18.5- to 24.9-kg/m2 category, gallstones were found in 3.9% (n = 6) of men, compared with 20.1% (n = 31) of women (P < .05). In the 25.0- to 29.9-kg/m2 category, the sex distribution was 12.3% (n = 19) for men, compared with 21.4% (n = 33) for women (P < .05), and in the ≥30.0 kg/m2 category, it was 13.6% (n = 21) for men, compared with 31.8% (n = 49) for women (P < .05). Table 6 also shows that the proportion of subjects with gallstones increased with higher BMI.
Distribution of Gallstones According to Body Mass Index and Sex.
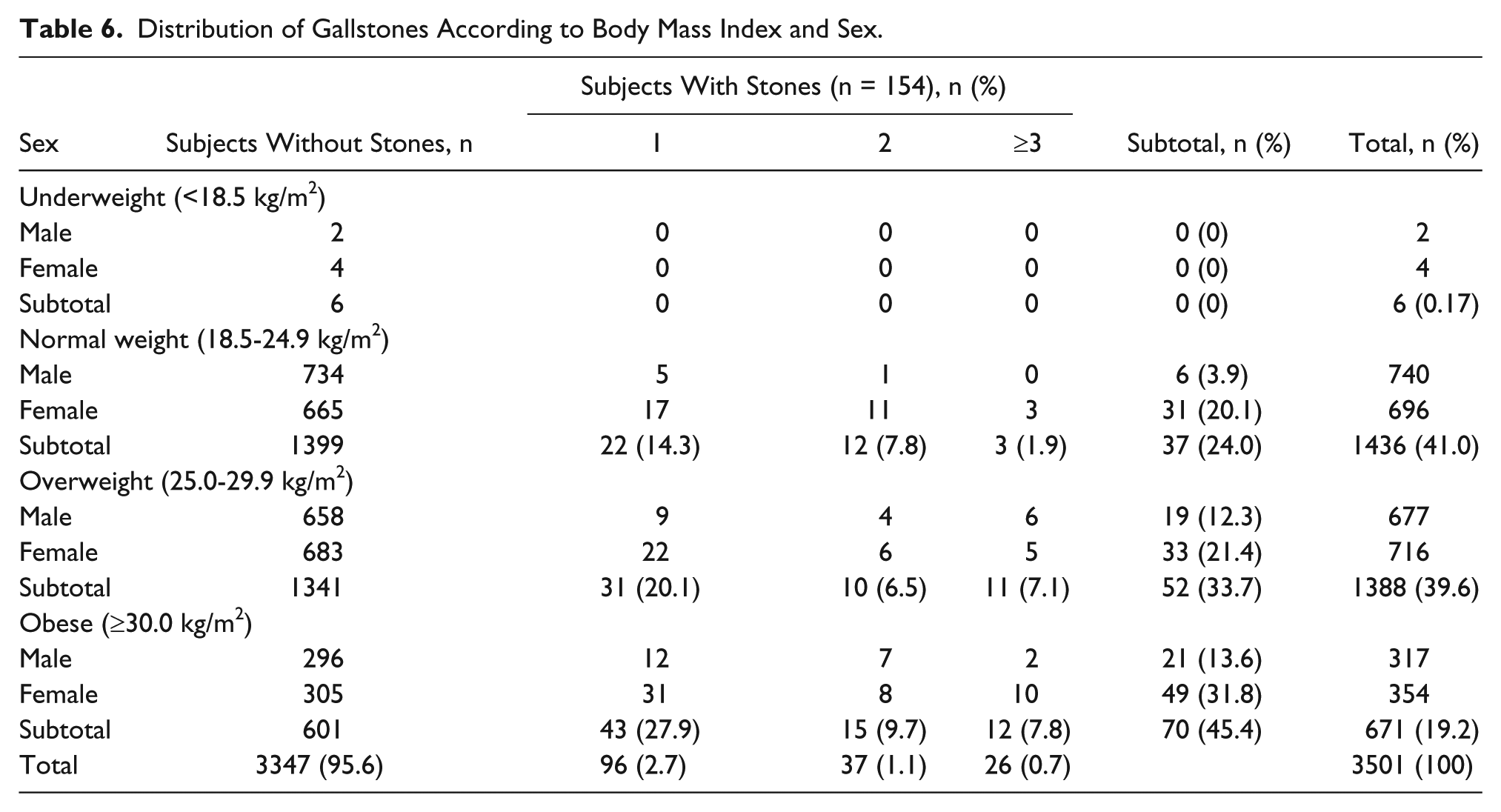
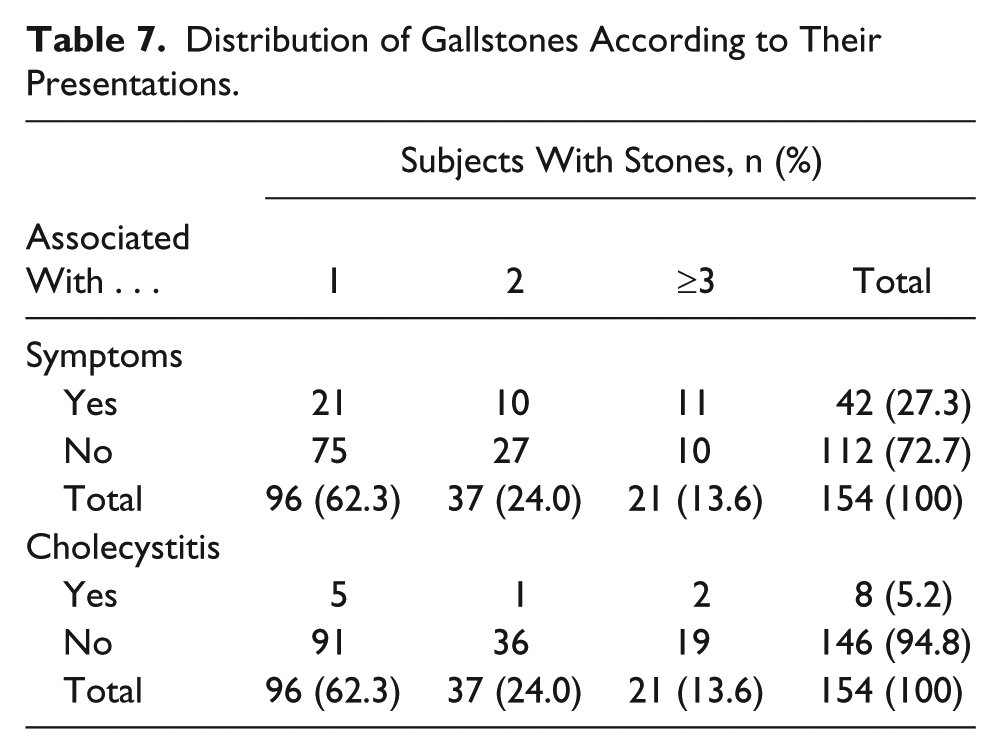
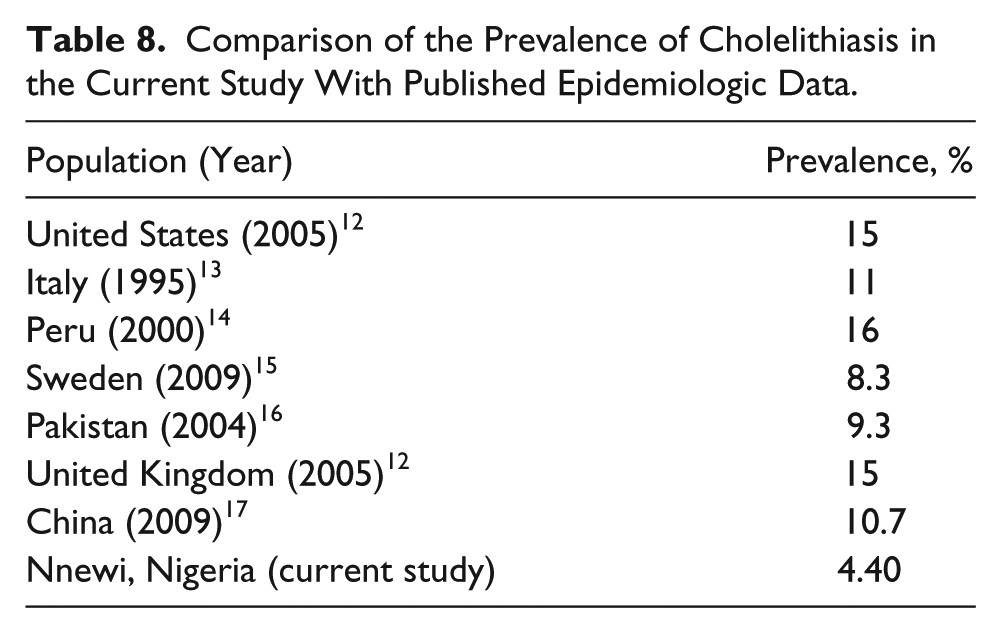
Table 7 shows the distribution of gallstones according to the presence or absence of symptoms and cholecystitis. Table 8 compares the prevalence of gallstones in the current study with that reported in other known epidemiologic reports.
Distribution of Gallstones According to Their Presentations.
Comparison of the Prevalence of Cholelithiasis in the Current Study With Published Epidemiologic Data.
Discussion
In this study, a total of 3501 subjects (n = 1770 women, 50.6%; 1731 men, 49.4%) were sonographically evaluated to derive epidemiologic statistics on gallstones specific to the Igbo population in Nnewi, Nigeria—a town predominantly inhabited by Nigerians of Igbo ethnic origin.
The results of this study show that gallstone disease may not be common in the locality, with only 4.4% of its adult Igbo population having the disease. This is markedly different when compared with reported statistics from other populations whom clinicians serve in Nnewi and the surrounding communities. In North America, Native Americans have a high prevalence of cholelithiasis, afflicting 64.4% of women and 29.5% of men.12,13 The overall prevalence of cholelithiasis in Caucasian Americans has been put at 16.6% in women and 8.6% in men,14,15 while black Americans have an intermediate prevalence rate, at 13.9% in women and 5.3% in men. 14 That cholelithiasis prevalence is lower in black Americans than Caucasian Americans is an indicator of an antilithogenic factor within black Americans that may be linked to heredity. The prevalence of cholelithiasis in the black Americans is, however, higher than what has been reported in native African populations and the present study and may be due to the influence of the Western-type diet. The reported prevalence of cholelithiasis is 11% in Italy 16 and 16% among Peruvian coastal natives. 17 It is 8.3% in Sweden, 18 9.3% in Pakistan, 19 and 10.7% in China. 20 The prevalence of gallstone disease in the United States, Europe, and Asia (cited in Table 8) shows that it is higher than the finding in our study. The findings of this study are similar to those of most studies on gallstone diseases in other native African populations. Gallstone prevalence was put at 2.1% in Ibadan (Nigeria), 21 4% in Tunisia, 22 5.2% in Sudan, 23 and 6.0% in South Africa. 24 The overall low prevalence of gallstone disease as found in this study and previous studies on other African populations may be the result of a combination of genetic, dietary, and environmental factors that are protective against gallstone formation.
The results of this study suggest that female sex is one of the risk factors for gallstone disease. The women were significantly more affected by gallstones than men. This may be due to other factors, such as pregnancy and sex hormones peculiar to women. Our study also showed that among the female participants, there was a significant (P < .05) link between parity and having cholelithiasis. For instance, the incidence of cholelithiasis among the nulliparous women is only 7.1%, whereas for parous women, the incidence is 28.3% for parity of one to three, 46% for four to six, and 18.6% for seven and higher. Previous studies also found that a high rate of gallstones is thought to be related to the number of pregnancies.12,16 Estrogen increases biliary cholesterol secretion, causing cholesterol supersaturation of bile. Thus, hormone replacement therapy in postmenopausal women is known to be associated with an increased risk for gallstone disease. 25
The results of this study share some similarities with findings from Europe and Asia. Our findings show that adult age is a risk factor for gallstone formation, as previously reported.26–28 This possibly explains the low occurrence of gallstones in the younger subjects as compared with their older counterparts that this study revealed. This finding is similar to previous reports indicating that long-term exposure to many risk factors, as is true for elderly, may increase the risk of gallstone disease.29,30 It is important to note here that sedentary lifestyles, which are more common among the elderly, may also increase the risk of gallstone disease. The results of this study further suggest an association between high BMI and gallstone disease. This is in agreement with a previous study establishing that in the Swedish population obese subjects had a significantly higher prevalence of cholelithiasis as compared with the reference population. 31 A study on pediatric obesity showed higher odds of gallstone prevalence among obese children, 32 probably because of the high level of plasma cholesterol in obese subjects. 33
The majority of the gallstones identified in this study were asymptomatic, in agreement with a previous report. 34 It is important that sonographic evaluation be repeated at some intervals for timely detection of complications. Individuals diagnosed with asymptomatic gallstones should avoid risk factors, to prevent progression to the symptomatic stage. A previous study revealed that age <55 years, smoking, female sex, greater body weight, presence of three or more gallstones, and presence of floating stones confer a high risk of progression from asymptomatic to symptomatic status. 35 The risk factors that are considered to be most controllable are smoking and body weight.
A cross-sectional design was adopted for this study; therefore, it has inherent limitations that cannot explain the effects of any of the risk factors implicated in the progression from asymptomatic to symptomatic gallbladder disease. The study also did not take into account the dietary pattern of the subjects, as well as any family history of gallstones, to account for the effect of diet and genetics. The number of elderly subjects recruited was low; therefore, the frequency of cholelithiasis in these age groups may have been unduly influenced by the population within them.
Conclusions
The prevalence of cholelithiasis in the Igbo adult population of Nnewi may be 4.40%. This correlates with earlier reports of the low prevalence of cholelithiasis in Africans. The findings of this study were that gallstone incidence was tilted in favor of women in the ratio of 2.8:1. Additionally, we found that in this cohort, BMI had a moderate influence on the prevalence of gallstones, which increased in subjects with high BMI values. This study indicated that the incidence of cholelithiasis among the female participants increased with parity, especially at three and above. The majority of the gallstones were asymptomatic and mainly noted as incidental findings. These findings may suggest that women and obese persons, who constitute the at-risk population in the locality, should be screened for gallstones at regular intervals. There may also be a need to screen at-risk populations in rural settings, where emergent care may not be readily available. Regular screening with sonography is quite possible in Nigeria, given the increasing availability of ultrasound equipment and the expertise to use it, even in rural locations. Sonography is currently the most widely available medical imaging modality in Nigeria, and the situation is likely to be the same in many other African countries. Cultural knowledge among health care providers when providing patient-centered care to diverse backgrounds is very important.
Footnotes
Acknowledgements
Many thanks to the academic board of the Department of Medical Radiography and Radiological Sciences, Faculty of Health Science and Technology, University of Nigeria, Enugu, for its useful criticisms of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.