
Abstract
Dermoid cysts are thought to be slow-growing tumors. This case series provides 2 clinical examples of sizeable growth of benign ovarian dermoid cysts in premenopausal patients. These patient cases were imaged initially; however, adnexal masses were not present on computed tomography images of the pelvis. Follow-up examination with sonography did demonstrate the presence of sizeable adnexal masses, which were confirmed by histology to represent benign dermoid cysts. Therefore, it may be wise to still consider ovarian dermoid cyst in the differential diagnosis in the setting of an adnexal mass that demonstrates the sonographic characteristics of a dermoid, even when absent on prior recent examinations.
Introduction
Dermoid cysts, also referred to as benign mature teratomas, are the most common primary ovarian neoplasm and account for 15% to 20% of all ovarian neoplasms. The highest prevalence is in patients 20 to 40 years of age. 1 These tumors originate from totipotent germ cells, which possess the ability to develop into well-differentiated tissue from embryonic germ layers. There are various sonographic features suggestive of dermoid cysts, including echogenic shadowing (calcification) in a predominantly cystic mass, a cyst with a fat-fluid level, a complex mass with echogenic material, and hyperechoic lines and dots, to name a few of the appearances.2,3 In fact, if two of the classic features are present in an ovarian mass, there is a high positive predictive value that the mass is a cystic teratoma.3,4
Most patients with dermoids are asymptomatic, although ovarian torsion, peritonitis from rupture and spillage of sebaceous contents, bowel obstruction, and malignant transformation can occur.5-7 Dermoid cysts are thought to be very slow growing, with an average growth rate of 1.8 mm/year in premenopausal women. 4 In fact, rapid growth of an ovarian mass, greater than 2 cm per year, has been used to exclude ovarian teratomas as a diagnostic consideration. 4 Based on a review of current literature, the rapid growth of ovarian dermoids has not been described. Two patient cases are presented that illustrate the potential to consider rapidly growing dermoid cysts.
Case Reports
Case 1
A 35-year-old woman presented to the emergency department for evaluation of acute right lower quadrant and right flank pain with associated nausea for approximately 1 week. The pain had progressively worsened and was associated with subjective fevers and urinary urgency. Physical examination was notable for tenderness to palpation over the right lower quadrant and right flank. A computed tomography (CT) scan of the abdomen and pelvis without contrast was ordered for presumed nephrolithiasis. The CT scan demonstrated a 4.2 × 4.9 cm right ovarian mass with focal area of fat attenuation strongly suggestive of a dermoid cyst (Figure 1A). A follow-up study was recommended that included a transvaginal sonogram. At the time of the sonogram, it demonstrated a large (5 cm) right adnexal complex cyst with an echogenic focus suggestive of the presence of fat. There was a fat-fluid interface, and peripheral blood flow was noted on sonogram (Figure 1B). Approximately 2 years prior, the patient was evaluated by CT for suspected appendicitis. No right ovarian mass was identified on this CT evaluation (Figure 1C).
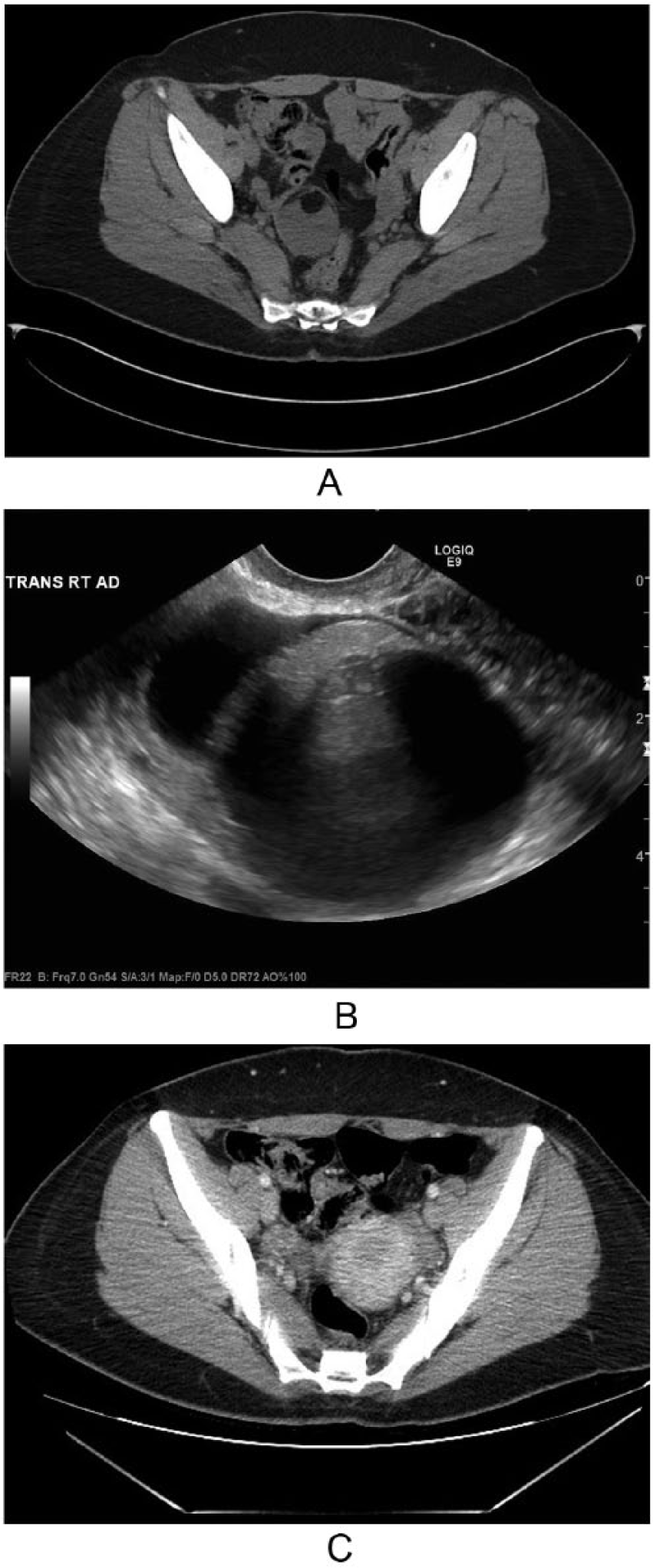
Case 1 imaging. (A) Noncontrast computed tomography (CT) axial image through the level of the ovaries demonstrated a rounded right adnexal mass with heterogeneous soft tissue and fat density contents (arrow). (B) Transvaginal gray-scale sonographic image of the right adnexal region demonstrated a complex cystic lesion containing an echogenic component with posterior acoustic shadowing. (C) Contrast-enhanced axial CT at the level of the ovaries, performed 2 years prior, demonstrated a normal ovary and failed to demonstrate a right adnexal mass (arrow).
Given clinical concern of ovarian torsion at this most recent encounter, the obstetrics/gynecology department was consulted, and a laparoscopic right ovarian cystectomy was performed without complications. Postoperative diagnosis was consistent with dermoid cyst without evidence of torsion. Gross inspection was consistent with pathological diagnosis of a mature teratoma.
Histologic examination of the prepared specimens confirmed the diagnosis of dermoid cyst and did not demonstrate evidence of malignancy. The patient was discharged to home after the first postoperative day.
Case 2
A 23-year-old woman presented to the emergency department with left lower quadrant abdominal pain. A transvaginal sonogram was ordered, which demonstrated a moderate amount of free fluid within the pelvis. The right ovary was unremarkable whereas the left ovary was viewed as being normal in size and without visible mass. There was an echogenic structure in the left adnexa with shadowing, which measured close to 4 cm (Figure 2A). No ovarian mass was detected on CT scan performed 5 years earlier, and an ovarian mass should have been observed on CT scan (Figure 2B). The patient was discharged to her home. The patient returned the following day with worsening abdominal pain associated with nausea, dysuria, and anorexia.
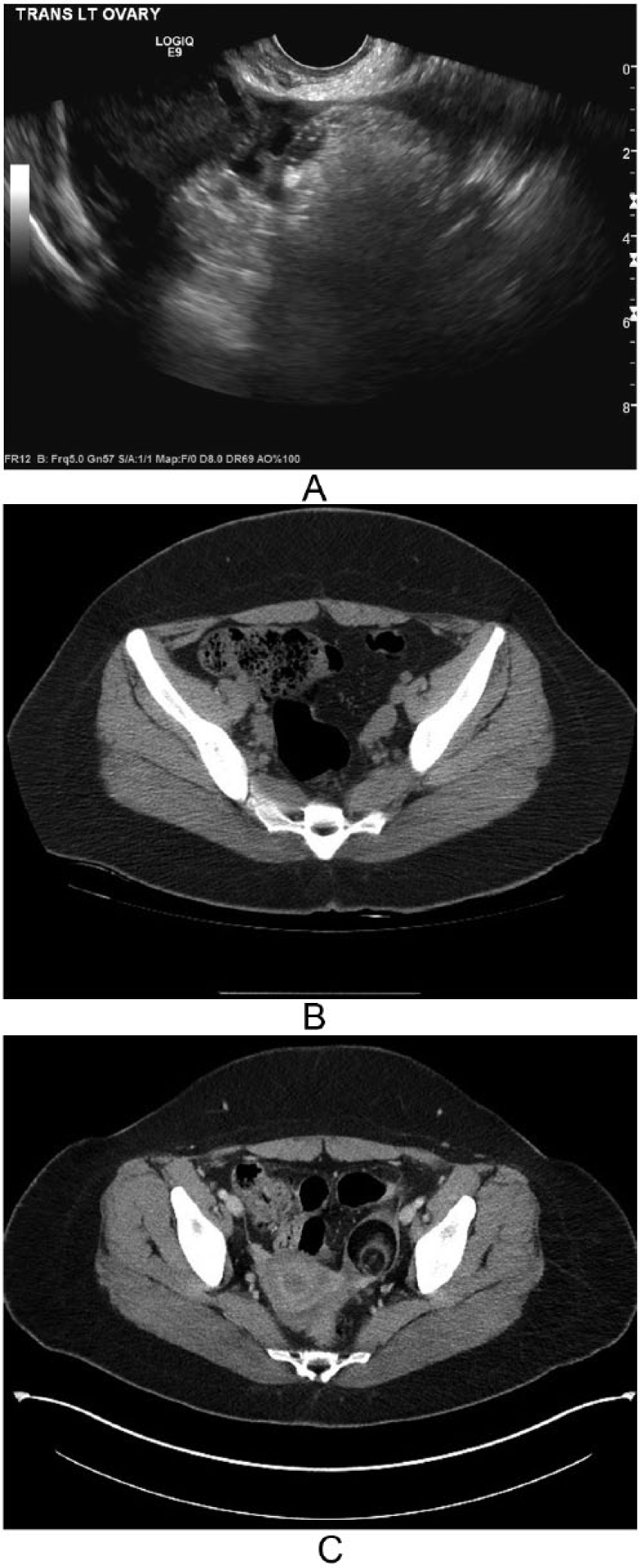
Case 2 imaging. (A) Transvaginal sonogram through the left adnexal region demonstrated a rounded echogenic mass in close proximity to the left ovary. This was interpreted as representing bowel gas, given the absence of a dermoid seen on the prior computed tomography (CT) examination. (B) Noncontrast axial CT at the level of the ovaries performed 5 years prior demonstrated a normal appearing left ovary (arrow) without evidence of a mass. (C) Contrast-enhanced axial CT image at the level of the ovaries demonstrated a left adnexal mass with predominance of fat-density contents (arrow). A small amount of fat stranding was seen surrounding the mass with accompanied free pelvic fluid.
Physical examination was notable for moderate discomfort and tenderness to palpation in the left lower quadrant with voluntary guarding. Pelvic examination was positive for left adnexal tenderness and fullness with no appreciable mass. The CT scan showed a 3.8 cm left adnexal mass with fat attenuation (Figure 2C) and an adjacently located ovarian cyst measuring 2.2 cm. Free fluid was noted in the pelvis. In light of radiologic features consistent with a dermoid cyst and the patient’s worsening abdominal pain, there was concern for ovarian torsion. The patient underwent laparoscopic cystectomy, and the left ovary was de-torsed without complication. Histologic examination was consistent with a mature teratoma without evidence of malignancy. The patient was subsequently discharged without complications after her hospitalization.
Discussion
Dermoid cysts are considered slow-growing tumors. 1 Ovarian dermoids have been reported to grow at a rate of 1.8 mm/year in premenopausal patients. 5 However, this case series provides two clinical examples of pathologically proven sizeable benign dermoid cysts in which prior CT examination failed to demonstrate their macroscopic preexistence, indicating much more rapid growth than 1.8 mm/year. The first patient case may have experienced a growth of almost 5 cm in a 2-year timeframe, or 25 mm/year. The second case may have grown to 4 cm in 5 years, or about 8 mm/year, which is much greater than the expected rate previously reported. To date, there is limited literature discussing the phenomenon of de novo, or rapidly growing, ovarian dermoid cysts. Whereas some reports have excluded ovarian dermoids from consideration of a more rapidly growing ovarian mass, there are other reports that show that dermoids may have more rapid growth. 4 Dermoid cysts appear to respond to hormonal changes during reproductive maturity, which stimulates sebaceous tissue within the cysts. 8 In particular, elevated levels of estrogen have been postulated to influence growth rate. 8 This is evidenced by a slightly higher growth rate in premenopausal women when compared with their postmenopausal counterparts. 5
Rapid growth of a previously diagnosed sublingual dermoid cyst was observed in a patient during pregnancy and eventually required surgical management. 8 In addition, a large dermoid cyst was observed in a pregnant patient during prenatal sonography at 22 weeks gestation and was not noted during imaging at 12 weeks gestation. 9 The authors postulated that abnormal estrogen/progesterone receptor expression in dermoid tissue could account for the rapid growth. 9 Furthermore, Tohma et al. 10 presented a case of a patient with de novo spinal teratoma, which was originally thought to be a drop metastasis of a previously diagnosed midline mixed germinoma with teratoma components. They concluded that the teratoma was de novo, owing to histologic examination and a difference in response to chemoradiotherapy when compared to the original intracranial lesion.
It is also noteworthy that the ACR Appropriateness Criteria suggest that CT is usually not appropriate for imaging a suspected ovarian mass, on initial examination. 11 They do suggest that transvaginal, transabdominal sonography and Doppler are usually appropriate for this clinical presentation and this certainly may have influenced the outcomes of these case studies.
Even though elevated hormone levels are believed to play a role in rapid growth of dermoid cysts, these two patients did not have a history of pregnancy between interval imaging sessions.
Therefore, the reason for the suspected rapid growth is unclear in these cases. Previously, rapid growth was thought to be a worrisome feature of malignant degeneration or, possibly, a different ovarian neoplasm. These cases raise the point that rapid growth may occur with nonmalignant dermoids. However, the larger sizes of the mass may predispose the patient to ovarian torsion, as described in this study.
The characteristic sonographic appearance of dermoid cysts is a complex or cystic adnexal mass that may contain a hyperechoic nodule (dermoid plug), fat-fluid level, thin echogenic lines (hair), or echogenic focus with shadowing (teeth), as an example. It can also appear as an echogenic lesion with posterior acoustic shadowing (tip of the iceberg), which can mimic bowel.
It has been shown that if classic features of a cystic teratoma are seen on sonography, there is a 100% positive predictive value in this mass being a dermoid. 3 Slow growth is most common, but more rapid growth should not exclude the diagnosis of a cystic teratoma (dermoid).
Conclusion
In summary, a benign mature cystic teratoma should still be considered when a new ovarian mass is identified in a patient with prior imaging that revealed no ovarian lesion. The presence of rapid interval growth may not necessarily indicate malignant transformation, even in the absence of hormonal stimulation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.