
Abstract
Annular pulley injuries are commonly found in the 3rd and 4th fingers under extreme strain in rock climbers. Here is presented a case of pulley rupture in the 5th finger following surgery to the wrist with no specific injury to the finger itself. The mechanism of injury here is likely to be a combination of repetitive strain during rehabilitation, partial injury during initial fall, and possibly irritation to the tendon caused by surgical hardware. Diagnosis was inconclusive or not possible by other modalities (clinical and imaging) and ultrasound has proved useful here given the correct technique and a good knowledge of anatomy and pathology.
Introduction
Investigation of finger pulleys is a less common musculoskeletal area to scan with ultrasound in general practice, and they require specialist knowledge to recognize and identify. 1
The digital flexor tendon is held in place along the curved surface of the phalanges by way of a retinacula portion of the tendon sheath. This retinacula section is made up of fibrous tissue which forms pulleys which wrap around the tendons. There are 5 annular pulleys and 3 cruciform pulleys. Pulley injuries, especially in the 3rd and 4th fingers, are most common among rock climbers when there is a foot slip, excessive strain on one finger or repetitive strain. Among rock climbers, injuries to the hands and fingers are prevalent with flexor tendon pulleys being the affected area in 20% of cases. 2
This case report aims to introduce the sonographer to the techniques and appearances involved in recognizing pulley rupture in an unusual injury etiology.
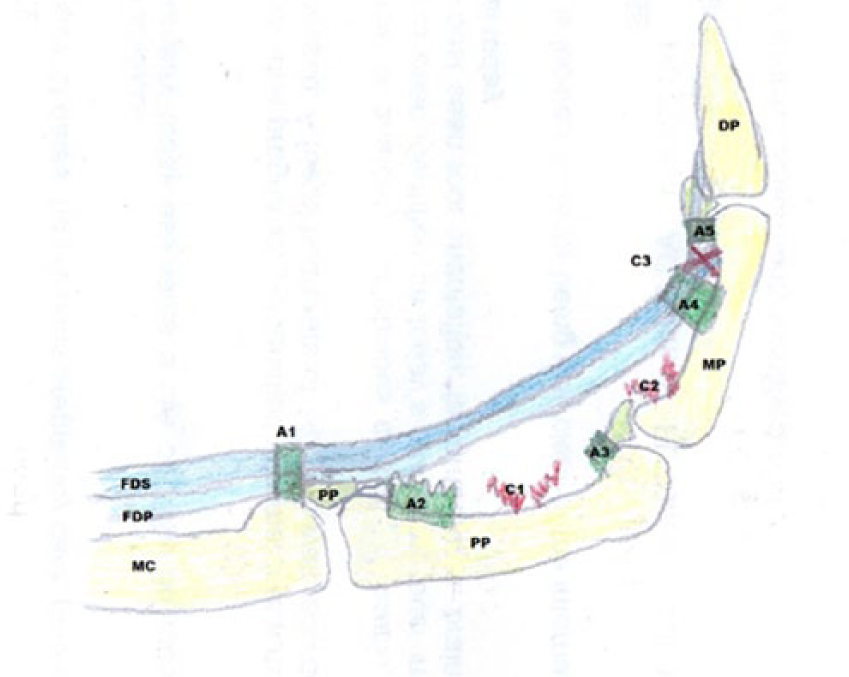
The normal anatomy of the annular (dark green) and cruciate (red) pulleys is introduced in Figure 1. Annular pulleys 1, 3, and 5 (A1, A3, and A5) arise from the palmar plates (PP) and stabilize the flexor tendons (flexor digitorum superficialis [FDS] and flexor digitorum profundus [FDP]) at the joints. Annular pulleys 2 and 4 (A2 and A4) and cruciate pulleys (C1, C2, C3) stabilize the tendons along the length of the proximal, mid, and distal phalanges (PP, MP, and DP).
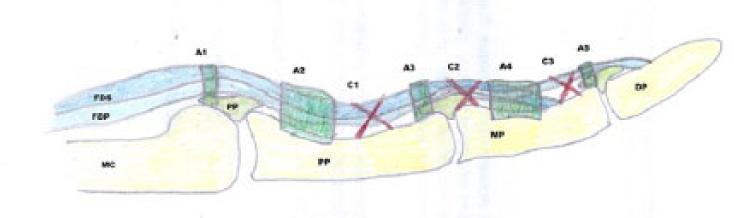
Annular and cruciate pulley system.
Case Report
A middle-aged, right-hand-dominant woman presented for sonography with a permanently flexed left little finger. Her history is that of a fall onto the outstretched hand with fractured distal radius and surgical plate insertion. The plate and screws were then later removed. After the removal, there was development of complex regional pain syndrome (CRPS). Subsequently, after the treatment for CRPS, the 5th metacarpal region became sore and the 5th finger began to curl. At first, the finger could be straightened with force but would curl back at rest. But after 1 year, the finger could no longer be straightened actively. She could not recall a particular injury to the finger but rather it gradually became fixed in that position over a few months.
After a return visit to her hand surgeon, she was sent for a sonogram, but no diagnostic images could be obtained due to the size of the probe and the difficulty of the location. She was then sent for a CT scan of the area, but the images were not useful as the distal phalynx was obscuring the view of the middle phalynx.
She then returned to her local hand specialist, where she was referred for a sonogram at the local clinic. On presentation to the clinic, it was noted that the contracture of the finger had appearances similar to those seen in Dupuytren’s contracture (Figure 2). However, with clinical examination and sonographic imaging, there was no evidence of the nodules typically identified with Dupuytren’s contracture.

Curling of the 5th finger similar to that seen with Dupuytren’s contracture.
Similar contracture of the 4th and 5th fingers also occurs with claw hand caused by entrapment or compression of the ulnar nerve, usually at the wrist. Due to the location of injury and surgical plate positioning, this was a possible cause of contraction. However, a true claw hand caused by ulnar nerve compression is accompanied by sensory complaints in the hand, of which there were none at the time of presentation.
As the finger could not be straightened, scanning access was difficult; however with the use of acoustic stand-off and a 9–12 linear array transducer, pictures were obtained demonstrating a bowstring tendon with ruptured annular pulleys (Figures 3–5).
Bowstring tendon due to injury to the flexor pulleys.
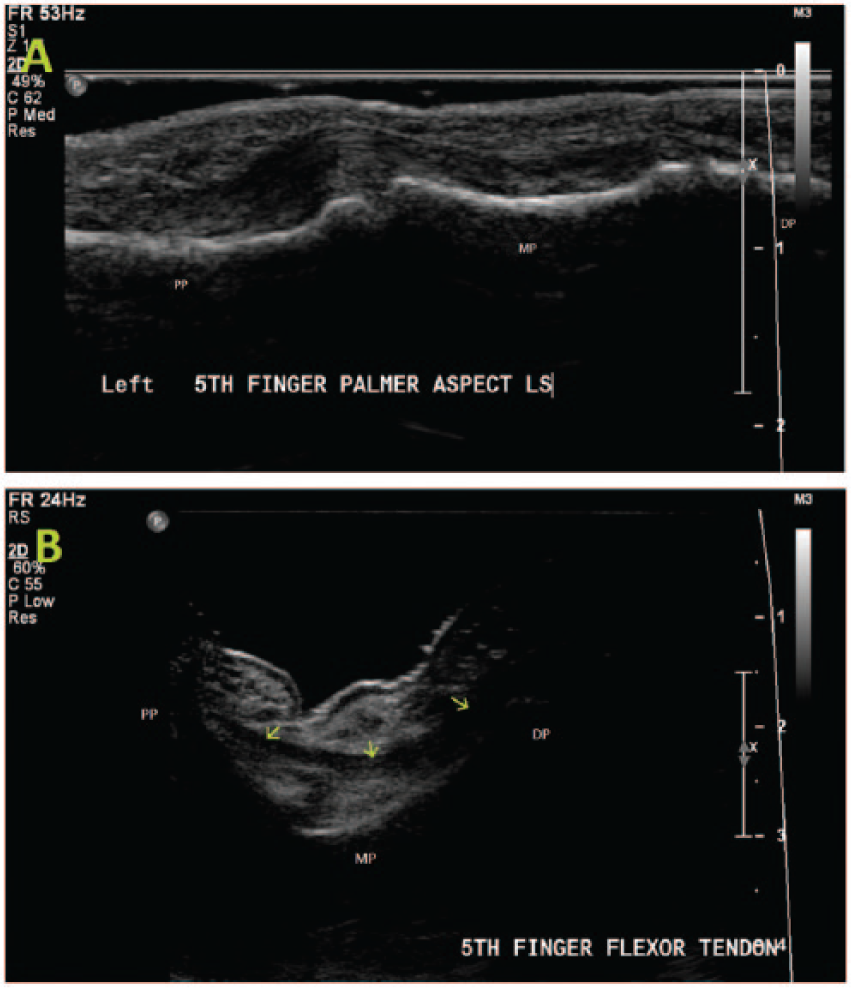
A normal (A) and a bowstring (B) flexor tendon (green arrows) with ruptured A2 and A3 pulleys. DP, distal phalynx; MP, middle phalynx; PP, proximal phalynx.
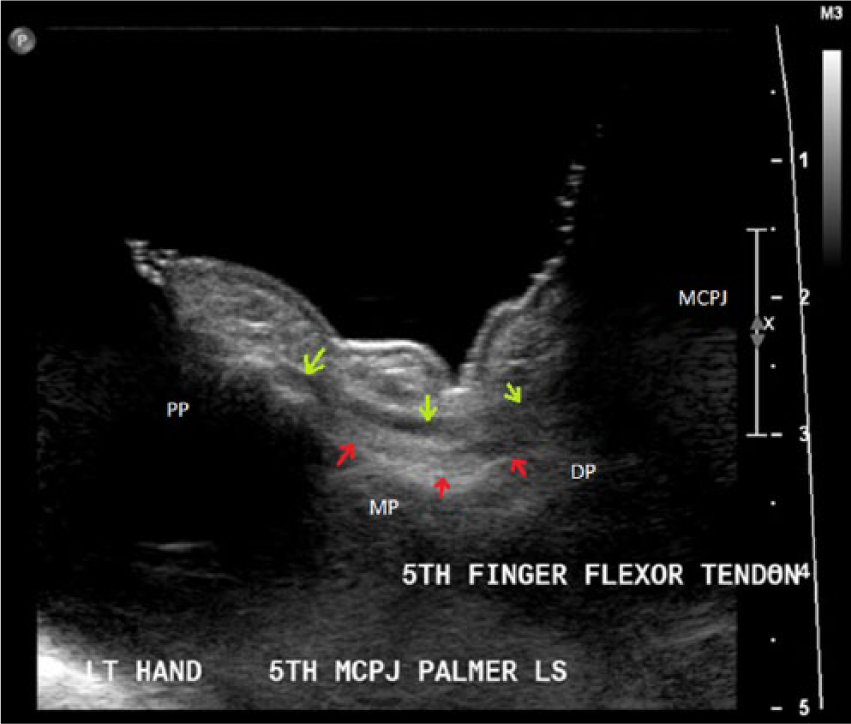
Use of an acoustic stand-off water bath demonstrating the extent of finger flexion and the distance between the tendon (green arrows) and bone (red arrows).
Discussion
As previously mentioned, clinically, this case appears similar to Dupuytren’s contracture. Dupuytren disease is characterized by nodular thickening of the palmer aponeurosis, which causes limited movement of one or more of the fingers. It has a prevalence of 1–2% and is more common in men than women. The most commonly affected digit is the ring finger. On sonography, it is demonstrated as sharply demarcated, hypoechoic nodular thickenings of the palmer aponeurosis, with no blood flow, between the skin and the flexor tendons.3,4
Compression or damage to the ulnar nerve in the Guyon’s canal is rare and the clinical symptoms can include sensory loss and motor deficiency in the digits. The leading cause of compression on sonography is wrist joint ganglion, which accounts for 30–40% of symptomatic cases.3,5
Apart from the original fall onto the outstretched hand, the cause of the radial fracture, there was no direct injury to the affected finger. A number of possible causes for this patient’s presentation exist and are discussed below.
CRPS is a chronic neurological disorder causing disabling pain, swelling and impairment of the affected limb. Treatment for CRPS can include desensitization of the area by brushing or massaging the skin, applying hot and cold or exercising the muscles. 6 The deformity of the finger now seen, may have been caused by an inflammation and swelling of the tendon sheath and subsequent pressure on the annular and cruciate ligaments. 3 Repetitive exercise of the region as treatment for CRPS or as rehabilitation following surgical repair of the facture may also have been a contributing factor or cause.3,6
Otherwise the original fall injury may have partially damaged pulleys and then subsequent exercise gradually worsened them, eventually causing the bowstring tendon rather than it appearing immediately following the original injury. 3
It has been documented that in several cases, close contact of the metal plate or screws, bone fragments or screw loosening, may lead to irritation of the flexor tendons and subsequent injury to or rupture of those tendons.7-10 Although in this case the flexor tendon appears intact, an irritation may have led to swelling of the tendon and/or sheath, placing pressure on the pulleys thus causing damage, triggering, and/or stress through repetitive strain. 3
Overall, the cause of this injury is unknown but is thought to be related in some way to the original injury or subsequent treatments.
Pulley rupture is common in rock climbers due to the level of strain on the flexed fingers and can be demonstrated with ultrasound.2,3,11,12 On sonography, the annular pulleys can be difficult to visualize as they lie flat along the flexor tendon sheath. The finger should be scanned in a straightened position where possible, with very light transducer pressure, plenty of gel or an acoustic stand-off pad. Triggering of the finger can be ruled out or demonstrated with dynamic imaging with flexion and extension.1,3 If there is excessive or permanent curling of the finger/flexion of the joints, the stand-off pad can be a useful tool. A water bath has been used as an acoustic stand-off. The use of water eliminates air from the space around the curvature of the finger, and allows for better angling of the transducer and easier imaging during flexion and extension. 1 Care must be taken in using a water bath due to issues of electric shock and equipment warrantees. A large moist acoustic stand-off pad can achieve the same flexibility and increase in image quality.
Swollen or hypoechoic pulleys are often identified on sonography in cases of trigger finger. Pulley rupture is identified as an anechoic defect or area of hematoma noted at the tendon sheath or between tendon and bone, or as a deviation of the tendon from its usual path along the curvature of the bone. 3
Partial strains of the pulleys may occur and cause only a slight swelling and pain but with repetitive strain they can develop into a rupture. 3 If given the appropriate conservative treatment, pulley strains, partial tears and singular pulley ruptures will heal themselves over time. However multiple completely ruptured pulleys require specialist reconstructive surgery.3,13,14 A number of effective surgical techniques have been developed. One such technique is the “loop and a half” technique of Widstrom and colleagues, which, when tested on cadavers, produced an average load to failure of 22.5 kg-force.13-15 Due to the bowstringing demonstrated in this particular case, it was diagnosed as multiple pulley rupture and therefore surgical repair would be the appropriate course of action. 14
Conclusion
Pulley ruptures are demonstrated on sonography by a significant gap or bowstring of the tendon away from the surface of the underlying bone. As pulley injury frequently leads to finger curling, an acoustic stand-off pad will provide the opportunity to increase image quality as well as detect this particular pathology. This particular case study demonstrates the value of how to use problem solving in the clinical setting and how the results could be helpful in cases where there is an unusual etiologic pathway to injury. It is through this adaptation of sonographic technique that musculoskeletal sonography will be recognized as an increasingly important diagnostic tool for patients.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.