
Abstract
Congenital pulmonary airway malformation (CPAM) is a rare congenital lung mass of the fetus that can present as solid or cystic. This is often diagnosed prenatally with sonography and routinely followed through the term of the pregnancy. Congenital pulmonary airway malformation is now classified into five different types that all originate from different areas of the lung and can vary in appearance. CPAM does present with a few differentials that need to be assessed, including bronchopulmonary sequestration, bronchogenic cyst, and congenital diaphragmatic hernia. It is vital to fully assess the fetal thorax and determine if there are any abnormalities present and if so the originating vasculature. This case report demonstrates a type 3-CPAM and its sonographic appearance as well as the classifications of CPAM and the possible differential diagnoses.
Keywords
Introduction
Congenital pulmonary airway malformation (CPAM) is a benign nonhereditary congenital mass of the lung that can present as cystic or solid mass.1, 2 This lesion is described as an overgrowth of terminal bronchopulmonary tissue. 3 Congenital cystic lung lesions are rare; however, CPAM is the most common fetal lung lesion. 4 Congenital pulmonary airway malformation is now classified into five different types that vary, depending on origin of the mass as well as presence of cysts, dimensions, and the sonographic appearance. 2 This particular lung mass is typically unilateral and most often discovered in the lower lobes of the lungs. Bilateral CPAM is rare and is associated with a poor prognosis. 5 Congenital pulmonary airway malformation occurs in approximately 1 in 11 000 to 1 in 35 000 pregnancies. 6 The average gestational age for discovery of the lung mass is 22 weeks. The following case report demonstrates a type 3-CPAM and its associated sonographic appearance.
Case Report
This case involves a 32-year-old female patient, gravida 5 para 4 with no prior pregnancy complications. The estimated gestational age of this singleton fetus is 21 weeks and 2 days, based on last menstrual cycle. The patient presented to the department for a routine anatomy scan of a 21-week fetus. A General Electric P5 (GE Healthcare, Milwaukee, Wisconsin, USA) ultrasound equipment was utilized and a curved linear array transducer. The frequency was shifted to 5.2 MHz. The sonogram showed an echogenic, homogenous, wedge-shaped mass that was discovered in the area of the fetal thorax, just superior to the fetal diaphragm (Figure 1).

Sagittal sonographic view of a wedge-shaped echogenic lesion in the thorax of a 21-week gestational fetus.
This patient was sent for a targeted sonogram of the suspected lung lesion. It was discovered during the targeted sonogram that the lung lesion measured 2.16 × 1.99 × 1.71 cm and was located in the right lower chest (Figures 1 and 2). No mass effect was visualized on surrounding structures or the vasculature. The mass had no sonographic evidence of cystic architecture. During the targeted sonogram, the vascular origin of the mass was thoroughly assessed to aid in the diagnosis of this lesion. It was determined that the mass originated from the pulmonary vasculature versus the thoracic aorta (Figure 3).

Transverse sonographic view of the same echogenic lesion in the thorax of a 21-week gestational fetus.
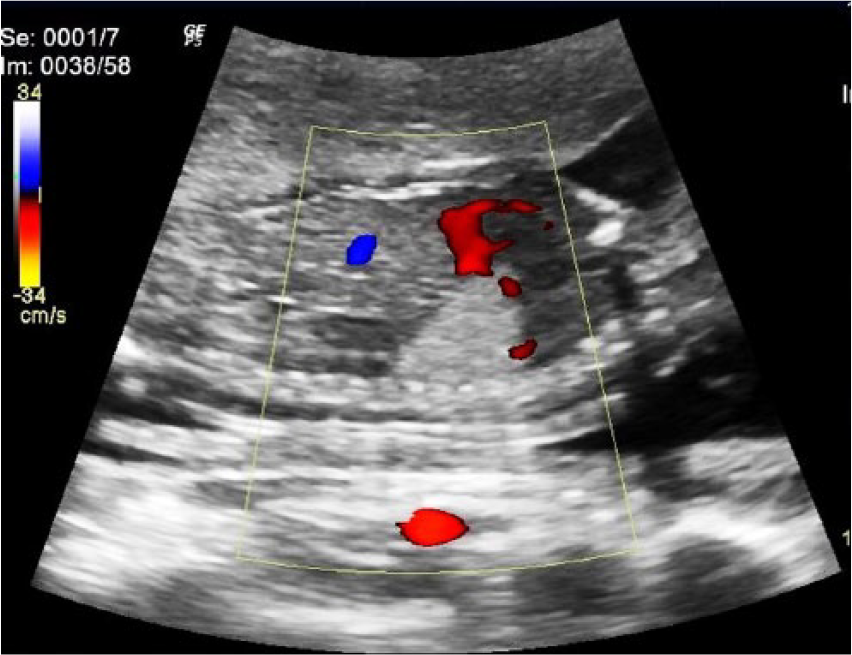
Color Doppler interrogation of a wedge-shaped echogenic lesion in the thorax of a 21-week gestational fetus, in the sagittal plane.
Determining the origin of vascularity helped to differentiate the diagnosis from a CPAM versus a bronchopulmonary sequestration. 7 Interrogating the vascular origin of the mass allowed the sonographer to discover if the mass originated from pulmonary vasculature or systemic vasculature. A CPAM is provided blood flow from the pulmonary artery. Bronchopulmonary sequestrations have a blood supply that originates from the thoracic aorta. Therefore, the vascular origin of the mass should be thoroughly assessed to differentiate the mass from other possible pathologies. In 1977, Stocker et al. 8 classified three different types of congenital cystic adenomatoid malformation (CCAM). It was broken down into types 1 to 3. In the year 2002, the Stocker classification was updated to add two additional classification types and changed the name from CCAM to CPAM. 9 The update was based on the discovery that there were two additional classifications of the lung lesion and that not all of the lesions were cystic or of adenomatoid origin. It additionally allowed for distinguishing where the lesion arose relative to the bronchial tree. 9 The additional classifications are referred to as type 0 to 4. Therefore, CCAM is more recently renamed and reclassified to CPAM with five different distinct categories. 9
Based on the Stocker classification, a type 3-CPAM is the best differential diagnosis for this particular case. 2 A follow-up sonogram was ordered for this patient in four weeks to check the size of the lesion and see if there were any changes in its sonographic characteristics. Four weeks later, there were no sonographic changes to the lung lesion. The patient was asked to come back in four more weeks for further follow-up. Unfortunately, the patient discontinued the follow-up appointment, and the mass could not be observed for any possible regression in size.
Discussion
Sonography is the gold standard imaging modality for obstetrics. There are certain situations where other imaging modalities may be useful to aid in a definitive diagnosis. In the situation of a CPAM lesion, sonography is the imaging modality of choice with MRI being an alternative option.10,11 Sonography is used to determine the size, shape, echogenicity, circulation origin, and any possible changes that may occur in the mass throughout the pregnancy. A MRI is useful in determining the exact anatomy of the lung where the pathological process is located. In a study that was reported by O’Conner et al., 10 sonography was advocated as a superior imaging choice for demonstrating the feeding circulation of the mass. 8
Congenital pulmonary airway malformation is broken down into five different types. Type 0 arises from the trachea or the bronchus of the lung, and it is the least common form of CPAM, occurring in approximately 1% to 3% of cases. Sonographically, this type will present as a solid echogenic mass with lungs that are small. This form of the condition is typically considered lethal. Type 1-CPAM is the most common form and arises from the distal bronchus or the proximal bronchiole. Fifty percent to 70% of CPAM cases are type 1. The sonographic appearance of type 1 is identified as one to a few large cysts present in the lung mass. Type 2-CPAM comes from the terminal bronchioles and accounts for approximately 15% to 30% of cases. This type of lesion contains cysts that are smaller in size and also has solid areas. The abnormality most associated with other fetal anomalies is type 2-CPAM. Type 3-CPAM arises from the alveolus and is rare. This type only occurs in about 5% to 10% of cases. Sonographically, this type of mass appears as an echogenic and solid mass because these cysts are microscopic. Type 4 arises from the alveolar and contains multiple large cysts. This type accounts for 5% to 15% of CPAM cases. In the past, type 4-CPAM has been associated with malignancy.12,13
There are a few differential diagnoses to CPAM. The most important differential diagnosis is a bronchopulmonary sequestration. Bronchopulmonary sequestrations are nonfunctioning lung tissue masses that are fed by the systemic vasculature. They are usually present in the lower lobes of the lungs. It can be very difficult to differentiate CPAM from a pulmonary sequestration. A bronchopulmonary sequestration appears as a solid, echogenic, homogenous, well circumscribed mass that can be round or wedge-shaped sonographically. The most difficult type of CPAM to differentiate from a pulmonary sequestration is type 3-CPAM. It is very important to identify the vascular origin of the mass to determine if the mass is fed from the pulmonary vasculature or if it is fed by systemic vasculature. Pulmonary sequestration is also associated with other fetal anomalies. An additional differential diagnosis to CPAM is a bronchogenic cyst. In a bronchogenic cyst, abnormal budding occurs during the development of the tracheobronchial tree. The least likely differential diagnosis for this entity is a congenital diaphragmatic hernia.2,6,14
A CPAM lesion typically cannot be found with sonography until 17 weeks’ gestation. 15 When a CPAM is found sonographically, routine sonograms are performed on the fetus to closely watch the lung mass. Changes can present in the mass, and it is important to follow and document any changes that may occur. It is typical for the mass to regress in size, and this usually begins to occur between 25 and 28 gestational weeks.7,14,16 Prognosis is going to depend on the CPAM classification and if there are other fetal anomalies present. 7 A larger sized lesion that does not regress in size is more likely to lead to a fatal outcome. 17 Hydrops fetalis could develop in the fetus from the mass compressing other structures; this will typically require an emergency cesarean section. 16 Other possible fetal anomalies that could be present with type 2-CPAM are gastrointestinal defects, defects of the abdominal wall, fetal heart anomalies, and anomalies of the central nervous system, spine, and kidneys. 13
A type 3-CPAM case study was reported by Bennett 1 in 2003. The patient was in her early 30s at the time of her second pregnancy. A sonogram was performed on her 20-week 6-day fetus, and a hyperechoic mass was visualized in the inferior posterior left lung. It was noted that there were no cystic structures visualized. This was considered to be most likely a type 3-CCAM, with a possible differential diagnosis of pulmonary sequestration. This patient went for MRI, and it was determined that the mass did not demonstrate any vessels that were originating from the thoracic aorta. This particular patient had routine sonograms once a month to follow the progress of the CCAM lesion. There was a sonogram performed a few days prior to birth, and the lung lesion was difficult to image and appeared to be significantly smaller in size from the original finding. The fetus had a good prognosis at birth. Although these cases are similar, the 2003 case could not demonstrate a vascular origin of the mass sonographically. With the quality and resolution of current ultrasound equipment, it is feasible that it could be easier to determine the vascular origin of a fetal lung mass. 8
An additional fetal lung mass case was reported by Fulghum and Vasquez. 13 This particular case was a case of triplets with no maternal complications. During a routine sonogram, a cystic lung mass imaged in the lower lobe of the left lung of fetus C. Sonographic measurements determined that the cyst was 3 × 4 cm. This lesion was followed by routine sonography throughout the term of the pregnancy. There were no further complications documented throughout the pregnancy, and the lung mass of fetus C remained unchanged. A chest CT was performed on this infant, and images showed a mass that covered half of the lower lobe of the left lung. The CT confirmed what had been discovered sonographically. Three months later, this infant underwent surgery to resect the lung mass. Upon pathologic evaluation, it was determined that the lung mass was CCAM. This case is another example showing that sonography is a good imaging modality for identifying fetal lung lesions. This case differs from the one being reported in that the mass appeared to have cystic components on the sonogram. A chest CT was the modality of choice as opposed to the use of imaging the mass with MRI. 10
Based on these descriptive cases, sonographers should consider the importance of thoroughly assessing the fetal lungs as part of a routine obstetric sonogram. It is important to realize that CPAM can present in several different variations depending on the lesion’s typology. When performing a sonogram, it is important for the sonographer to image and document the echogenicity of the fetal lungs and assess for areas of localized increased echogenicity. If a mass is found in the lung, besides marking, measuring, and applying color Doppler to the lesion, it is also important to determine the circulation of the mass. Documenting the circulation afforded the mass helps to provide information that could differentiate it from pulmonary sequestration. It is also important to measure the mass as precisely as possible to establish a basis for assessing any changes that may be seen in follow-up sonograms. Measuring the mass from leading edge to leading edge repeatedly would be helpful to ensure measurement accuracy. The sonographer wants to check for cystic components in the lesion to help better differentiate the diagnosis. If possible, Harmonic tissue imaging can also be applied to help in determining if cystic components are present in the lesion. The recent change in designation and classification of this entity has provided two additional classifications than were originally determined with CCAM; therefore, this is important information for sonographers. A list of the different types classified based on their sonographic appearance 11 is provided:
- Type 1: cystic with large cysts
- Type 2: cystic and solid with other anomalies
- Type 3: echogenic solid mass
- Type 4: large cystic mass
- Type 0: solid mass with small lungs.
See Figure 4 for a diagram comparing the different types of CPAM.
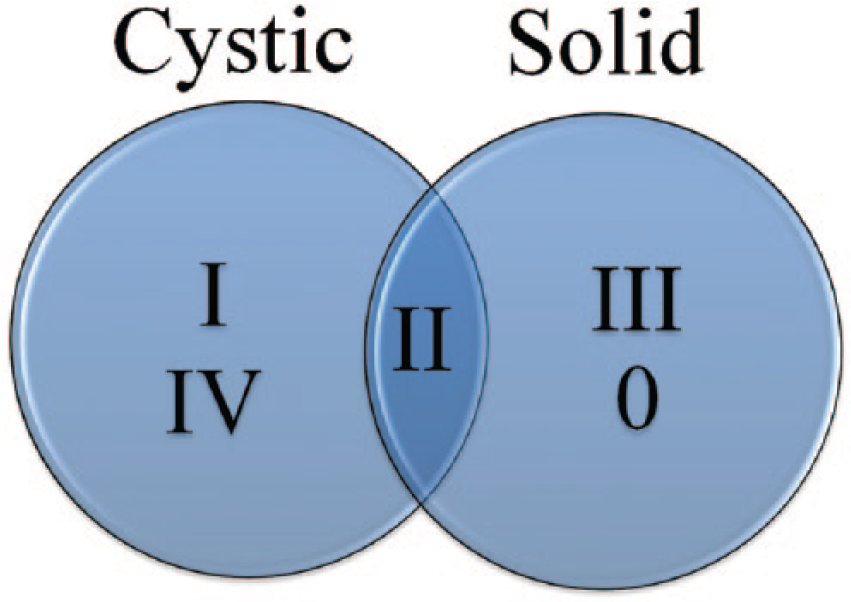
Scheme for categorizing the sonographic appearances of congenital pulmonary airway malformation (CPAM).
Conclusion
Congenital pulmonary airway malformation, once referred to as CCAM, represents approximately 25% of congenital lung lesions. CPAM is classified into five different types depending on origin, cyst presence, and cyst size. The most common differential diagnosis to CPAM is the bronchopulmonary sequestration. CPAM is typically found at around 22 gestational weeks and is followed up with routine sonography through the term of the pregnancy. CPAM can vary in sonographic appearance as well as prognosis depending on the classification of the lesion. Sonography plays a vital role in the identification and screening for CPAM. Sonography and MRI are recommended as imaging modalities for classifying the type of mass that is present.
Footnotes
Acknowledgements
The author would like to thank Jacqueline Monaco, RDMS, RVT, El Centro College, and family for their support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.