
Abstract
Assessment of the fetal heart during routine obstetrical screening remains a challenge for sonographers and physicians. Reliance on still images and nonstandard methods of acquiring images and assessing the fetal heart contribute to the relatively low rate of identification of congenital heart disease (CHD). A standardized assessment of the fetal heart using two cine-loop sweeps has been shown to address some of these challenges. Image acquisition using two cine-loop sweeps combined with a standardized five-step assessment is proposed to address the limitations of the nonstandard approach in place at most screening centers today.
Introduction
The majority of deaths from congenital defects in childhood can be attributed to congenital heart disease (CHD). Congenital heart disease is six times more common than chromosomal abnormalities and four times more common than neural tube defects. 2 The most common cause of birth defects, CHD is most frequently reported with an incidence of 0.8% of all live births. 3 Improvements based on technical advances in the management and therapy of CHD has resulted in a shifting of the outcomes such that adults living with CHD outnumber the number of children with CHD. 4
Typically, the role of the sonographer during routine obstetrical screening is to identify normal and abnormal features of the fetal heart and provide an image recording of these for the interpreting physician. The routine second trimester examination is performed in real time and documented as a series of still images archived electronically or on film. Most often, the interpretation of the cardiac images is performed by a radiologist or obstetrician using the still images. Present detection rates for CHD may vary widely depending on a number of factors: operator skills, maternal obesity, fetal position, inadequate image optimization, image acquisition protocol, and the nature of the CHD. 5 In order to clarify the recommended fetal heart structures for examination, the American College of Radiology (ACR) and the International Society of Ultrasound in Obstetrics & Gynecology (ISUOG) have published guidelines for routine second trimester screening. Both of these publications require the four-chamber view, also known as a basic assessment, and where possible, views of the left ventricular outflow tract (LVOT) and right ventricular outflow tracts (RVOT), commonly referred to as an extended examination.6,7 Prenatal detection rates using these methods are summarized in Table 1.
Prenatal Screening Detection Rate by Protocol and Population.
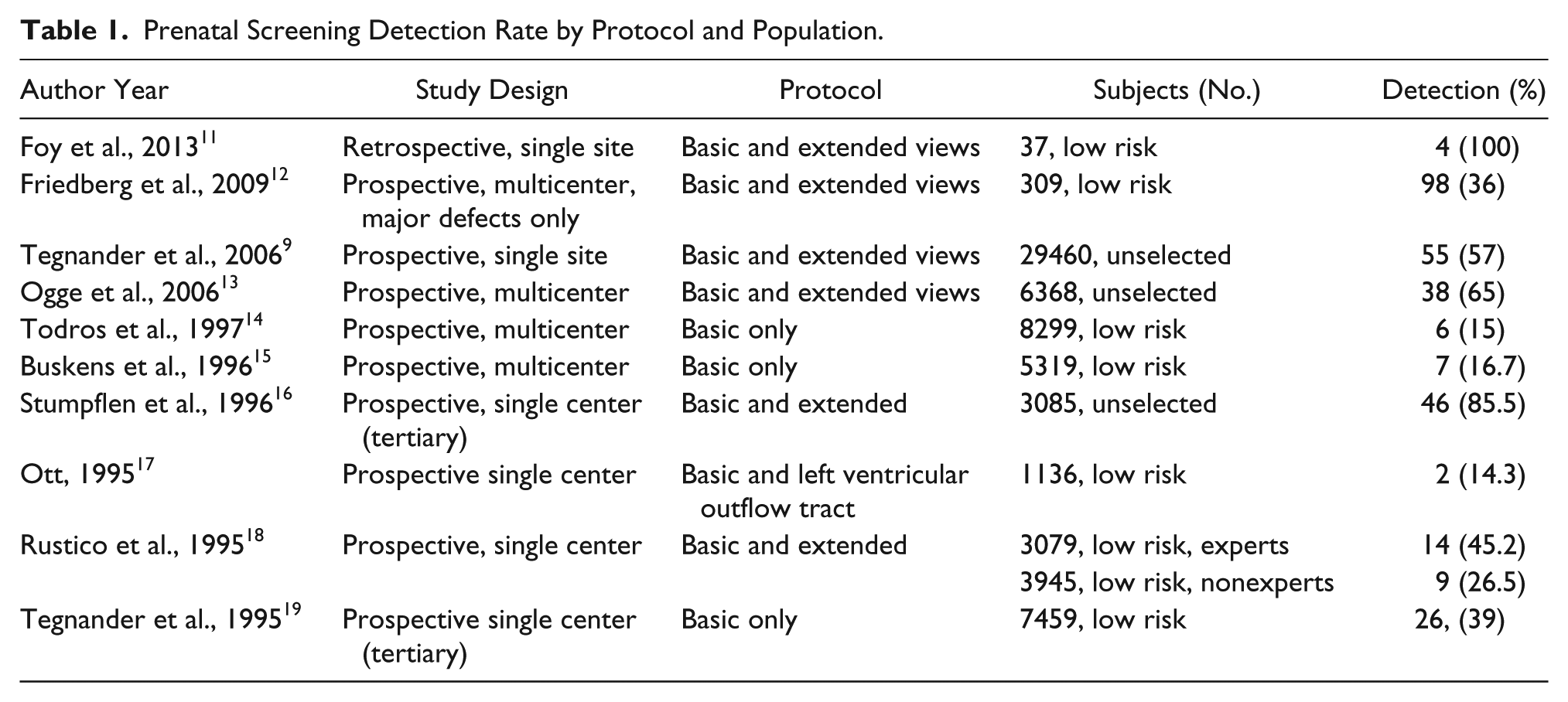
The range of detection varies widely by author and study type. Those studies that relied solely on the basic protocol ranged in detection from 15% to 39% while those that included the extended protocol demonstrated a higher rate of detection 26.5% to 86.5%. It is widely accepted that the extended examination will improve the detection rate of CHD compared with the basic examination only.8–10 Despite the inclusion of outflow tracts as part of an extended examination of the fetal heart, only three11,14,17 of the seven studies9,12,14,15,17–19 listed in Table 1 achieved a detection rate greater than 60%. There remains considerable room for improvement in detection rates, especially considering the impact of missed congenital heart disease during prenatal screening.
Standardized Assessment
Congenital heart disease is based on structural and functional deviations from normal embryological development. Screening the fetal heart, unlike other fetal organs, requires an evaluation of normalcy in functional terms as it beats and demonstrates the synchrony of the valves, chambers, and conduction system. Further, a complete exam of the fetal heart will expose the relationship of the ventricles to the outflow tracts, the outflow tracts with respect to one another crossing at approximately 70°, and clarify the function of other important structures such as the cardiac valves. 20 A thorough assessment of the continuity of these structures and their function is not feasible as a series of still images.
Current practices in routine obstetrical screening are limited in a number of important ways. Limited screening time is a significant constraint, and the design of a standardized method to detect CHD that enables adoption by sonographers and interpreting physicians must take this into account. The practice guidelines provided by the American Institute of Ultrasound in Medicine and the American College of Radiology clearly articulate what fetal cardiac structures should be imaged; however, they do not specify how or to what standard they should be documented.6,7 The guidelines do not specify that the interpreting physician observe a real-time assessment of the fetal heart, nor do they establish any specific relationships that must be observed such as that of the outflow tracts relative to one another and their continuity with the ventricles. It may be possible to observe the practice guidelines in ways that do not necessarily lead to effective screening of congenital heart disease.
A number of authors have identified the use of cine-loops as a practical means of improving the assessment of the fetal heart.21-23 Acquiring cine-loops as compared to still images only has the potential to significantly increase the visualization rate of normal fetal heart structures. 23 A standardized assessment can be performed if the image acquisition process is well structured and includes cine-loops.
Image Acquisition
A real-time assessment of the fetal heart can be completed using two sweeps and storing them as cine-loops (see Figure 1). The situs to four-chamber sweep begins in the transverse abdominal plane at the level of the stomach and ends at the four-chamber view. The four-chamber to outflows sweep begins in the four-chamber view and slides through the ventricular outflow tracts. Together, these two sweeps will provide the sonographer and the interpreting physician with a more complete set of images in real time for assessment compared with still images.
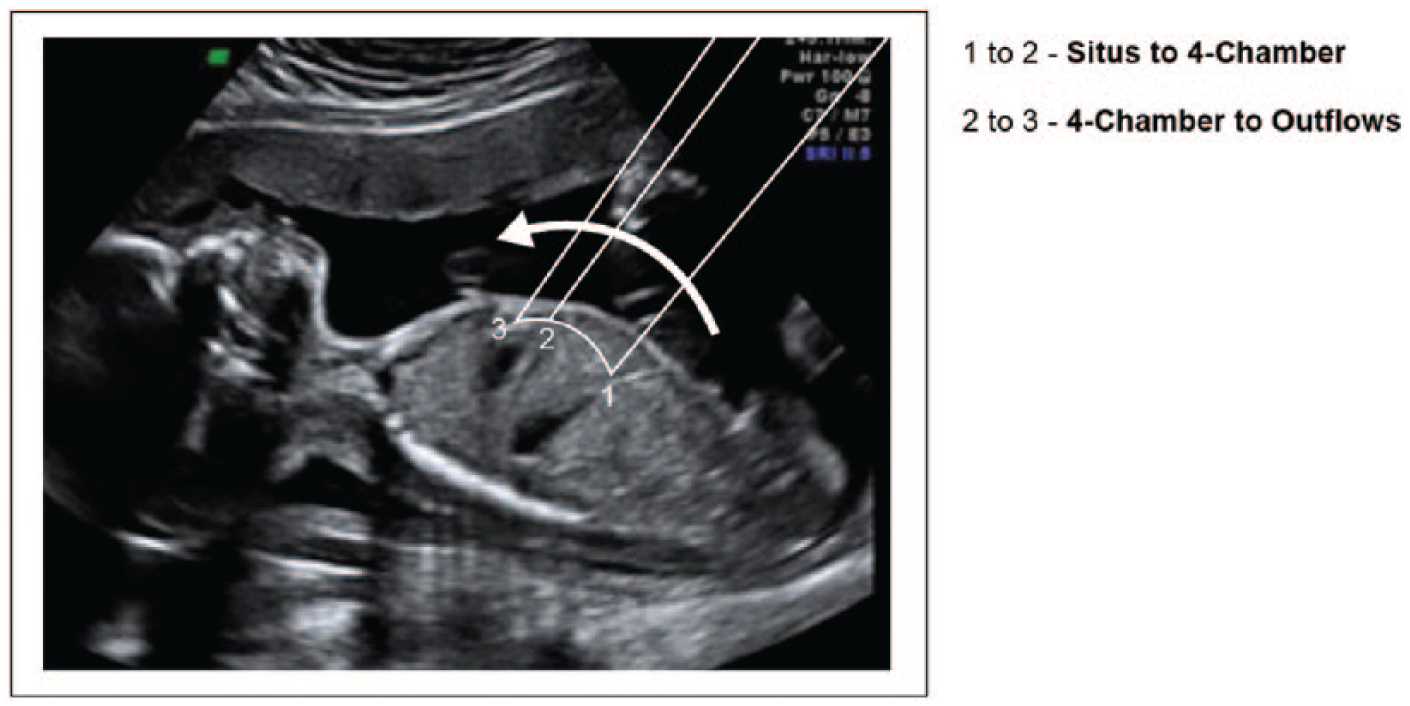
The first cine-loop sweep begins at the level of the stomach in the transverse plane sweeping into the four-chamber view of the fetal heart. The second cine-loop sweep begins at the level of the four-chamber heart indicated by the straight line at point 2 and continues through the outflow tracts. Line drawings provided by Ken K. Wong, graphic designer, Mohawk College.
Sonographic system settings should ensure that the fetal thorax fills 50% to 75% of the field of view (see Figure 2). The focus and frequency settings, including harmonic processing, should be optimized. Frame rate should be set between 30 and 100 Hz. 24 Cine-loops can be stored as DICOM files in either a MiniPACS or Radiology PACS application. In a prior study involving the use of cine-loop sweeps, the sweeps were captured as four-second clips, and the mean acquisition time was 4 minutes and 18 seconds, which was statistically equivalent to the time needed to capture three still images, the four-chamber image, and both outflow tract images. 23 Sharing cine-loops with experts can be accomplished within an enterprise application or as an exported video file, formatted as an AVI, MPEG, Quick Time, or similar standard. Typical video file sizes for a four-second, grey-scale cine-loop as a Quick Time and MPEG movie files range from 1 to 2 megabytes, while AVI files can be much larger in size, 40 to 50 megabytes. Given the storage capacity available as a local server, enterprise server, or cloud storage solution, cine-loops do not impose a burden on the storage capacity for most PACS applications.

The fetal thorax fills more than 50% of the field of view; transducer frequency and focus are optimized for spatial resolution. The harmonic signal processing option is selected, and the frame rate is set at 51 Hz.
To acquire the situs to four-chamber sweep, position the transducer in a transverse plane at the level of the stomach, slide the transducer cephalad from the abdominal circumference into the four-chamber view, without changing angles to the fetus; this can be likened to “moving up the elevator to the next floor.” A good four-chamber level will include one complete rib. 24 Acquisition of the image should begin showing situs and capture at least two beats of the situs in order to allow the viewer to be able to appreciate the pulsatility of the aorta. Next, slowly slide the transducer cephalad without changing the angle (see Figure 3). The inferior vena cava (IVC) should be shown to enter into the right atrium as the four chamber view approaches. The acquisition should end with at least two beats of the four chambers visible. Practice may be required to obtain a complete sweep. It is a good practice to acquire several sweeps and keep the best one. From the four-chamber view, rotate slightly toward fetal left shoulder and angle cephalad (see Figure 3). The first outflow tract visible is the left ventricular outflow tract (see Figure 4). Angling the transducer, more cephalad will enable visualization of the right ventricular outflow tract. The pulmonary artery is the most anterior structure in the heart, so often the bulk of the heart is not visible at this level.
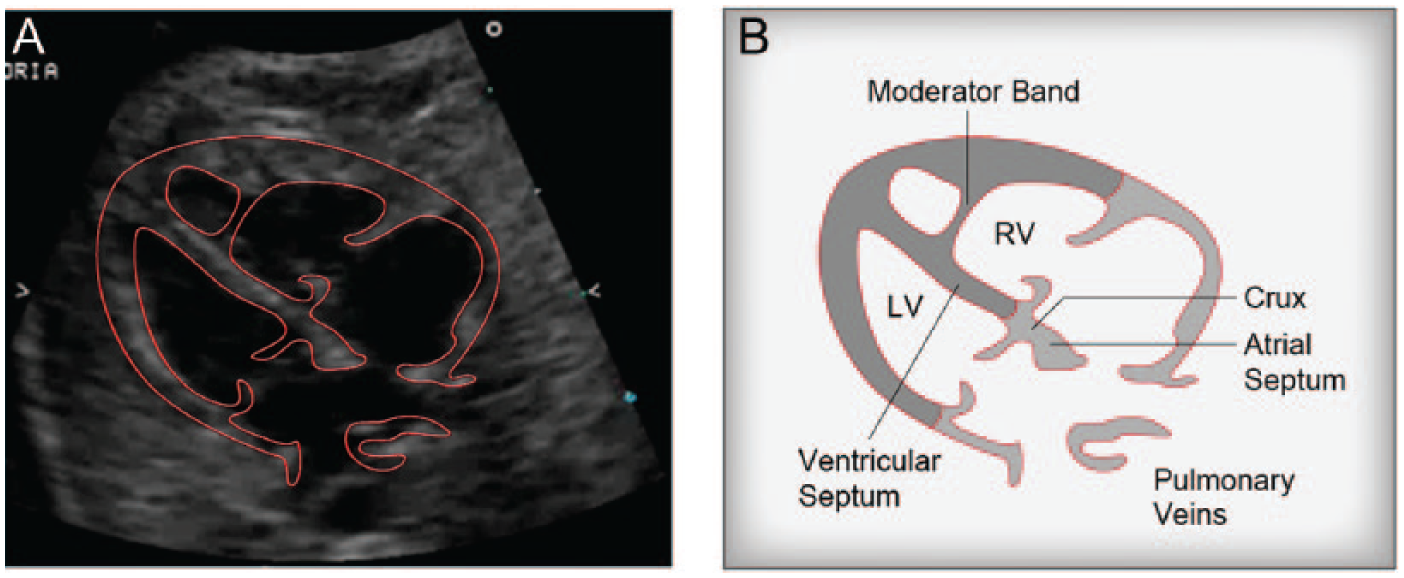
Still images representing key landmarks beginning with the situs-four chamber cine-loop sweep in 4A-4B. Line drawings provided by Ken K. Wong, graphic designer, Mohawk College.
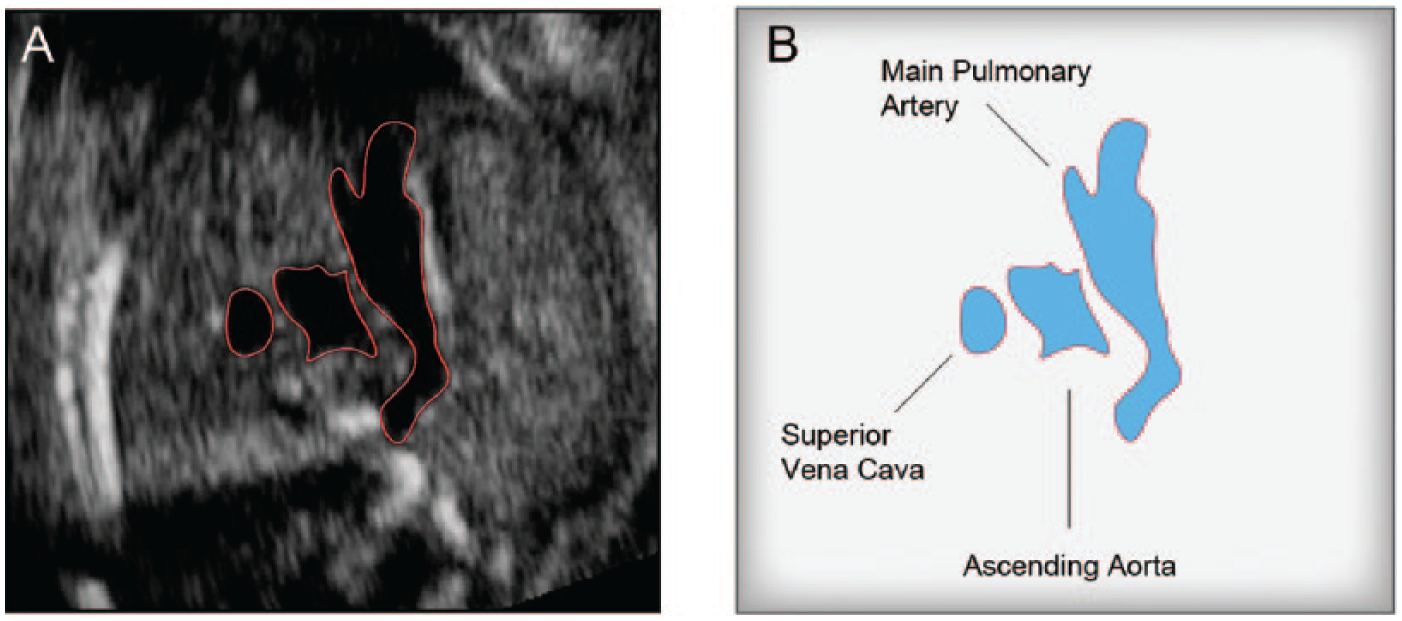
The four chamber through outflow tracts sweep represented by 5A-5B. It is often possible to include the three vessel view in this sweep. Line drawings provided by Ken K. Wong, graphic designer, Mohawk College.
Assessment
Before an assessment of the fetal heart is made, it is important to determine the fetal lie in order to enable identification of fetal left and right anatomy. Once this is determined, a five-step assessment can be undertaken to determine normalcy (see Figure 3).
Step 1
Assess the situs, axis, and size of the fetal heart. In a transverse section through the fetal abdomen, identify the unilateral organs (see Figure 3A):
A leftward descending aorta and stomach; aorta is circular and can be identified by its pulsations corresponding to the fetal heart rate.
A rightward IVC, slightly anterior and rightward of aorta; IVC is circular/oval in shape, is not pulsatile but is collapsible, and it may be seen to change size over the cardiac cycle in response to changes in cardiac pressures. The size can also be influenced by pressure exerted by surrounding organs. Careful inspection is required to locate this vessel since it may be difficult to see due to its small size. The IVC should be seen to enter the RA when performing the situs sweep.
Using the spine as a guide to the center of body, an imaginary line can be drawn from spine to anterior abdominal wall to form the antero-posterior axis; this axis divides the transverse section into left and right halves.
There are three types of situs that can be identified: situs solitus, situs inversus, and situs ambiguous. Situs solitus represents the normal arrangement as described previously. Situs inversus represents the complete inverse of normal anatomy; it is very important that the fetal left and right is identified to confirm this condition. There are two common forms of situs ambiguous: right atrial isomerism also known as asplenia and left atrial isomerism also known as polysplenia. When the aorta and IVC are found on the same side of the body, the arrangement is referred to right atrial isomerism, the liver is usually midline, and the stomach can be found on either side of the body. Left atrial isomerism occurs when the IVC is absent in the abdomen and replaced by an azygous vein, which runs parallel to the aorta and slightly posterior on either the left or right side.
The situs sweep provides the sonographer with the opportunity to assess the cardiac axis, stomach, and heart relationship. The cardiac axis can be defined as levocardia, mesocardia, or dextrocardia. Levocardia is the normal position of the heart in the left chest with the apex of the heart leftward and the interventricular septum forming a 45° angle relative to the anterior-posterior axis of the chest. A heart positioned centrally in the chest is referred to as mesocardia. Dextrocardia is a condition where the heart is found in the right chest. Dextrocardia can be defined by three types: (1) dextroversion, where the apex is rightward; (2) dextroposition, usually due to a space occupying lesion, apex remaining leftward; and (3) mirror image dextrocardia, the heart is completely inverted in the right chest.
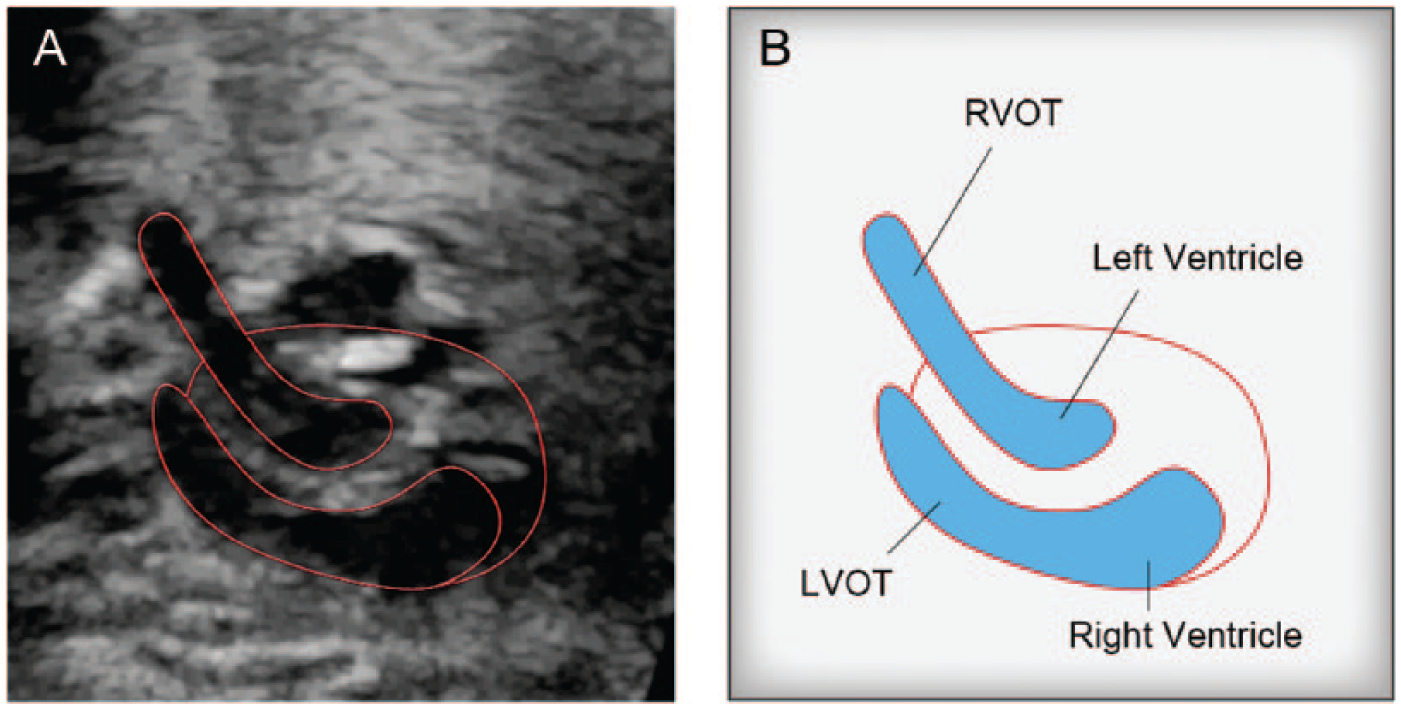
The blood flows out of the right ventricle through the left ventricular outflow tract (LVOT) while blood flow leaving the left ventricle passes through the right ventricular outflow tract (RVOT). The parallel configuration of the outflow tracts associated with the transposition spectrum of congenital heart disease (CHD) is defined.
Step 2
It will be possible to assess the four chambers in real time using both sweeps (see Figure 3B). Two atria should be visualized approximately equal in size and separated by an incomplete septum. The foramen ovale flap is seen in the left atrium with the septum primum forming one arm of the crux of the heart. The left atrium is anterior to the descending aorta and spine. The descending aorta should be the only vessel (seen as a pulsatile circle) between the left atrium and the spine. In over 50% of normal studies, at least two of the four pulmonary veins will be seen, usually one from each lung. 23 Two ventricles should be seen, approximately the same size, with symmetry in wall thickness and contractility. The right ventricle will become slightly larger than the left ventricle as pregnancy progresses. The ventricles will be divided by a complete septum; tricuspid and mitral valves should be about the same size and open freely. The tricuspid valve is inserted slightly closer to the apex than the mitral valve. This offset is best seen when the apex is facing toward or away from the transducer. Identification of this feature is significant as the tricuspid valve is always attached to the right ventricle (RV), and the mitral valve is always attached to the left ventricle (LV). The left ventricle will be conical in shape, and its walls will be relatively smooth. The right ventricle is closest to the anterior chest wall, pyramidal in shape, and its walls will be rougher due to the presence of trabeculae. The apex of the right ventricle may appear more “filled in” compared to the apex of the left ventricle due to the presence of the moderator band.
Step 3
The four chamber to outflows sweep will expose the outflow tracts and their connections to their respective ventricles (see Figure 4A). In this step, the LVOT will be assessed to confirm that the aorta is seen arising from the left ventricle. The inter-ventricular septum should continue as an uninterrupted wall and be continuous with the anterior aortic root wall. The base of the anterior mitral valve should be in close proximity to the point where the posterior aortic root begins, and the aortic valve leaflets should be thin and open well, appearing to disappear in systole.
Step 4
In this step, the normal position of the RVOT will be confirmed (see Figure 4B). The RVOT should be seen anterior to the LVOT; the pulmonary artery is seen arising from the right ventricle. The pulmonary artery and the aorta cross at their origins; further downstream, they do run parallel for a short distance. The pulmonary artery trifurcates into the ductus arteriosus and two smaller arteries, the right and left branches. The pulmonary valve leaflets are thin and open well, appearing to disappear in systole.
Step Five
This step will confirm that the outflow tracts intersect at their origins at approximately 70°. The pulmonary artery is slightly larger than the aorta; this becomes more evident later in gestation. The cine-loop will provide the opportunity to review the frames repeatedly to ensure that the orientation of the outflow tracts is normal. The presence of a parallel orientation of the outflow tracts indicates an abnormal fetal heart. A summary of the key points of assessment relative to the cine-loop sweeps and steps is provided in Table 2.
Summary of Steps, Sweeps, and Fetal Heart Structures Visualized.
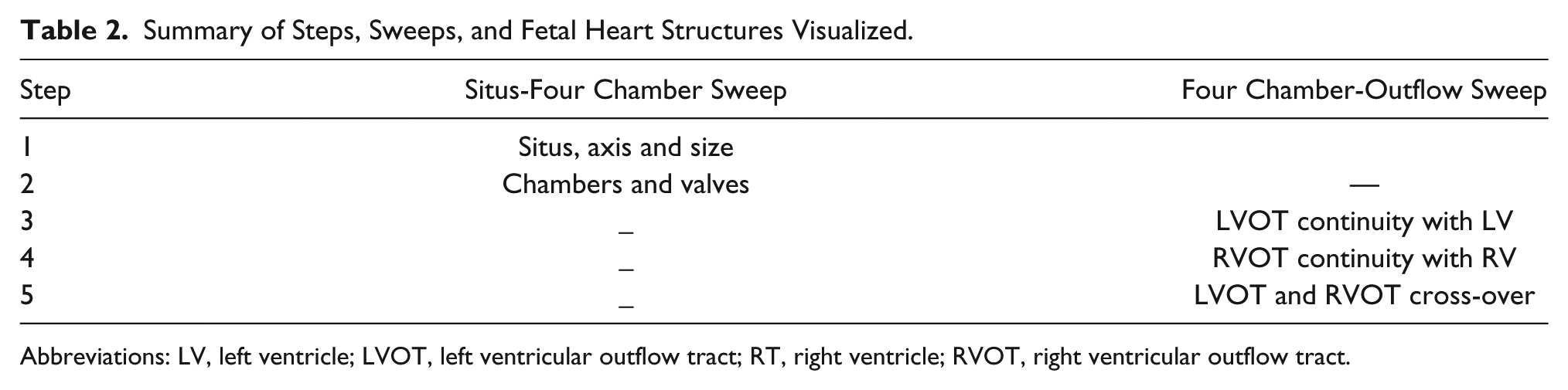
Abbreviations: LV, left ventricle; LVOT, left ventricular outflow tract; RT, right ventricle; RVOT, right ventricular outflow tract.
Summary
Assessment of the fetal heart during routine obstetrical screening is an important element of the examination. In practice, the detection of CHD remains comparatively low relative to the detection of pathology in other anatomical systems. 25 The importance of visualizing and assessing the relationship between the outflow tracts is depicted in Figure 1. In this example, a form of transposition of the great vessels is identified by the abnormally parallel course of the outflow tracts.
The use of cine-loop sweeps has been found to increase the detection rate of CHD by 38% for nonexperts (radiologists) and 36% for experts (pediatric cardiologist and pediatric cardiology sonographer) compared with the use of still images only. 1 The implementation of a standardized assessment technique of the fetal heart in real time, using cine-loop sweeps represents a practical approach that can be used by the majority of screening centers. 1 The standardized technique is limited to those centers with the capability of storing cine-loops as part of the clinical record. The sonographer must also become familiar with acquiring cine-loops in a systematic way ensuring that the cine-loop sweep start and endpoints are observed. However, if these constraints can be overcome, the benefits of a real-time assessment and an extended examination can be fully realized.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.