
Abstract
Uterine scar dehiscence is a complication seen in pregnancy commonly from previous cesarean scars. It increases the risk for uterine rupture, which carries a high incidence for maternal and neonatal morbidity and mortality. Ultrasound is an effective method to monitor the defect closely throughout pregnancy to help predict uterine rupture or neonate complications. Repair of a dehiscence may be possible, allowing for future pregnancies.
Introduction
Asymptomatic lower uterine segment dehiscences are sometimes noted at the time of repeat cesarean delivery but are uncommonly diagnosed early in pregnancy. Uterine dehiscence is an incomplete separation of a uterine scar with an intact serosa layer. 1 Dehiscence increases the risk for uterine rupture; therefore, careful evaluation of the tissue surrounding the outpouching is imperative. Uterine rupture is the complete disruption of all uterine layers including the serosa and is associated with a high incidence of maternal and neonate morbidity and mortality. 1 Uterine surgeries such as cesarean sections put women at a higher risk for both dehiscence and rupture. The author reports two cases of uterine dehiscence and the role sonography played in evaluation and treatment planning.
Case Reports
A 27-year-old pregnant woman, G3P1102, presented to an outside clinic for initial prenatal care. The patient had a history of two prior cesarean deliveries. At 17 weeks 4 days gestation, she reported “not feeling right” with a gradual onset of right lower quadrant pain, which subsided within approximately 24 hours. An MRI was performed, and a myometrial defect was identified in the anterior lower uterine segment (Figure 1). The patient was hospitalized for monitoring and to discuss treatment options. An obstetric ultrasound was performed for further evaluation of the defect utilizing a Philips iU-22 ultrasound system with a C5-1 MHz transducer and a C8-4v MHz transducer.

Sagittal MRI image of patient No. 1 showing the defect in the anterior lower uterine segment (arrow).
Endovaginal sonography revealed a myometrial defect measuring 1.26 mm, with a portion of the amniotic sac protruding through the defect. The examination also showed the fetus in a breech position, normal amniotic fluid, and a placenta located on the posterior left aspect of the uterus, away from the defect. The fetal position allowed its foot to enter the defect (Figure 2). This additional strain and pressure on the unprotected amniotic sac led to increased concern for uterine rupture.
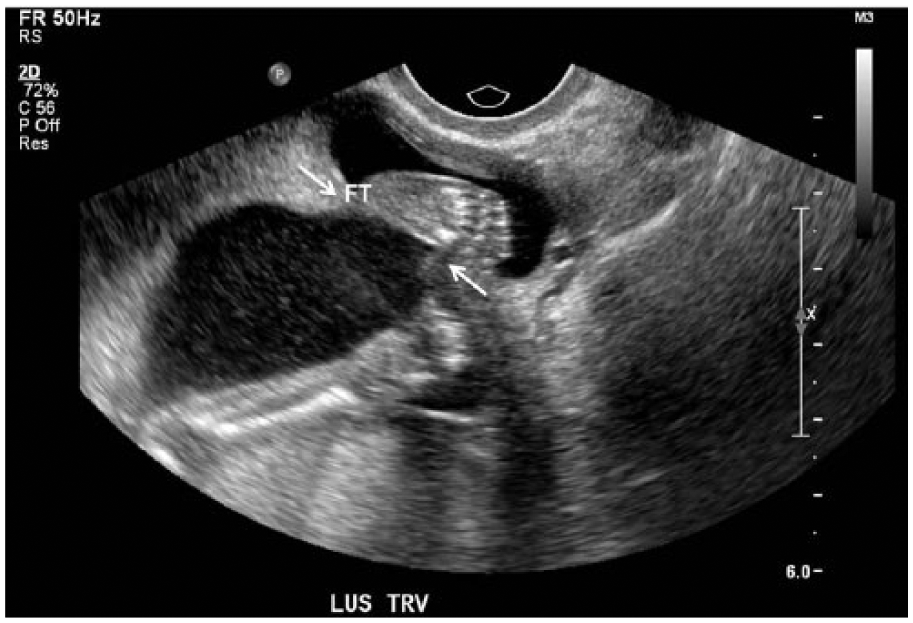
Transverse image of the anterior lower uterine segment of patient No. 1, showing the fetal foot extending into the defect (arrows).
The patient was counseled on management options, including pregnancy termination, attempted in utero repair of the defect, or expectant management with preterm delivery. Repair of the defect was not advised due to its location posterior to the bladder and because the patient was stable and asymptomatic. The patient declined termination. A follow-up ultrasound was performed at 18 weeks 0 days gestation and showed the defect to be stable. The patient was discharged with activity restrictions and weekly endovaginal ultrasounds for continued monitoring of the defect.
An early cesarean delivery was performed at 34 weeks gestation to avoid the onset of spontaneous labor or rupture of membranes. During delivery, the defect appeared to extend to the level of the internal cervical os but was successfully repaired. Tubal ligation was also performed. The delivery was without complication.
The second case occurred in a 33-year-old pregnant woman, G3P2002. The patient had a history of two cesarean deliveries. Prior to this pregnancy, the patient underwent a sonohysterogram and a pelvic ultrasound to evaluate the integrity of her uterus. The sonohysterogram showed fluid tracking outside the uterus. The patient had an MRI for further evaluation. No defect was found; however, the lower uterine segment was thin with absent myometrium identified. Surgical repair was planned, but the patient became pregnant before the surgery was performed.
Prenatally, the patient was monitored with serial ultrasounds for dehiscence of the anterior lower uterine segment. At 29 weeks 6 days gestation, she presented with left-sided groin pain that radiated to her buttock and down the back of her leg. An obstetrical ultrasound was performed utilizing a Philips iU-22 ultrasound system with a C5-1 MHz transducer and a C8-4v MHz transducer.
Endovaginal sonography revealed a myometrial defect measuring 3.5 cm, with a portion of the amniotic sac protruding through it (Figure 3). The examination also showed the placenta located on the anterior aspect of the uterus extending toward the defect. Due to the anterior and inferior location of the placenta, in addition to the lack of myometrium and close proximity to the bladder, the patient was at an increased risk for placenta percreta.
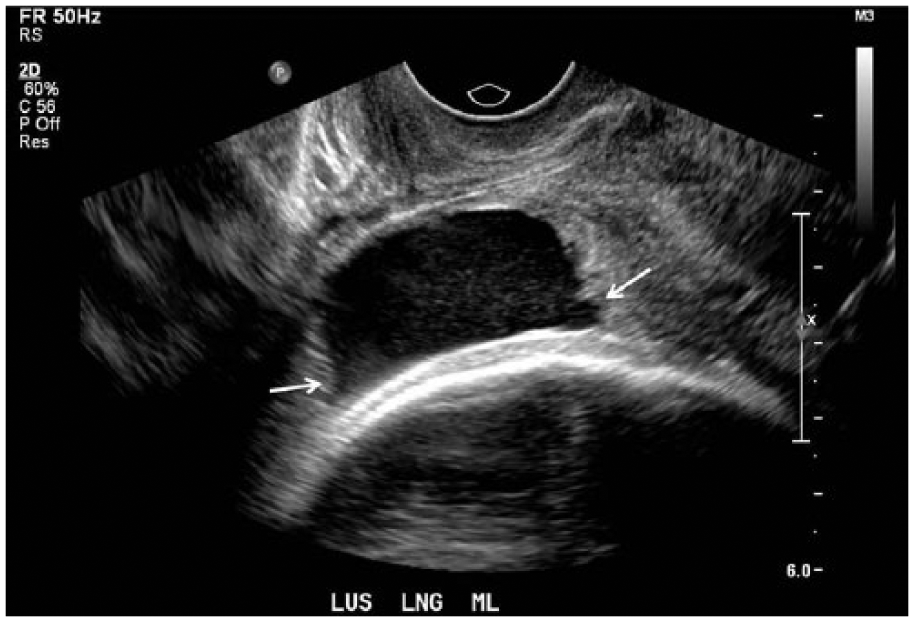
Longitudinal image of the anterior lower uterine segment of patient No. 2, showing the uterine dehiscence (arrows).
The patient was admitted for evaluation and to discuss management options. Due to the late gestational age of the fetus, expectant management with preterm delivery was considered the best option. The patient was discharged with biweekly non–stress test monitoring, weekly amniotic fluid index measurements, and weekly clinic visits with strict return precautions.
An early cesarean delivery was performed at 36 weeks gestation to avoid the onset of spontaneous labor or rupture of membranes. The defect was repaired at the time of delivery without complications to the mom or neonate.
Discussion
Uterine strength after cesarean section is very important for predicting the outcome of future pregnancies. This is especially important in women who have had repeat cesarean deliveries. Cesarean section scars put women at an increased risk for menstruation problems, ectopic scar pregnancies, uterine dehiscence, uterine rupture, and poor performance in labor. 2 Uterine incision closure methods may have a large effect on the strength of the uterus in future pregnancies. Patients who have had a “modified two layer closure” of their uterus report less bleeding, greater scar thickness at six weeks postoperation, and fewer instances of scar dehiscence. 3
A scar dehiscence develops as a weakened uterus, usually from a previous cesarean section, grows during pregnancy. As the gestation progresses and the uterus expands, the scar may lose integrity, leading to the separation of uterine layers, starting with the inner layers of the uterus and working outward. The defect is considered a dehiscence as long as the serosa layer of the uterus stays intact. Complications of uterine dehiscence are influenced by fetal position, location of the defect, and location of the placenta. Location of the placenta in relation to the defect may also put patients at risk for abnormal adherence of the placenta to the uterine wall. Placenta percreta occurs when placental vessels penetrate the uterine wall. If this occurs, the mother is at risk for severe hemorrhage, hysterectomy, organ reconstruction, and possibly death.
Separation of the serosa is considered a uterine rupture. The overall incidence of uterine rupture is increasing due to the increasing number of cesarean deliveries being performed. One study found that uterine rupture occurred in 5 of 1000 mothers with a history of cesarean section. 4 Uterine rupture has many adverse outcomes for both the mother and neonate. One study found that almost half of mothers diagnosed with uterine rupture after a trial of labor developed moderate postpartum hemorrhage, 15% developed severe postpartum hemorrhage, and 3.8% required a peripartum hysterectomy. In the same study, 57.7% of neonates were found to have perinatal complications, of which 9.3% were considered serious. These included perinatal death, severe asphyxia, and post-hypoxic encephalopathy. 4
The MRI is considered the gold standard for the diagnosis of uterine dehiscence. However, sonography is a useful modality used to follow patients and monitor changes in the defect throughout pregnancy. When evaluating a cesarean scar dehiscence in a pregnant woman, both transabdominal and endovaginal sonography are recommended. Depending on the location of the defect, the gestational age of the fetus, and the habitus of the mom, a transabdominal approach may provide a better overall view of the defect in relation to the fetus and the bladder. An endovaginal approach may provide more detail about the size of the defect and whether or not the serosa layer of the uterus is still intact. The neck of the defect should be measured in addition to the size of the sac protruding through the defect, when possible
There are several treatment options for uterine dehiscence, including pregnancy termination followed by repair of the defect, attempted repair of the defect with the pregnancy in utero, or expectant management with preterm delivery. Repair of the defect with the pregnancy in utero carries a significant risk of uterine rupture. This option should only be considered if the dehiscence is symptomatic. The more common practice is close monitoring of the pregnancy with weekly endovaginal ultrasounds and early cesarean delivery. Early delivery is imperative because the rupture of membranes and contractions increase the risk of uterine rupture, requiring an emergent cesarean delivery. At the time of delivery, the defect may be repaired; however, hysterectomy may be necessary if damage to the uterus is extensive. One study discussed the repair of a symptomatic cesarean scar dehiscence in a non-pregnant woman utilizing a da Vinci–assisted laparoscopic procedure. The procedure successfully repaired the defect and resolved the patient’s symptoms. 5
There is debate in the current literature as to whether prior uterine dehiscence or rupture puts patients at risk for recurrence. One case series followed 60 pregnancies in women with a history of rupture or dehiscence. The study found that uncomplicated pregnancies were possible as long as patients were closely monitored and delivered by elective cesarean section before the onset of labor. They had no patients with recurrent uterine complications, but 6.7% of the patients were found to have a uterine dehiscence at the time of delivery. 1
Conclusion
Dehiscence of a cesarean scar is rarely diagnosed early in pregnancy but is a complication that may lead to uterine rupture if not monitored closely or treated with early cesarean delivery. The MRI may be necessary for the diagnosis of uterine dehiscence, but sonography plays an important role in monitoring the uterine defect and documenting any changes. Repair of the defect may be possible at the time of delivery, and patients should be monitored closely during future pregnancies.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.