
Abstract
We report the results of a joint thyroid clinic with a consultant surgeon and consultant radiologist to offer “triple assessment” for patients on a single visit. All new referrals from September 2011 to December 2013 were reviewed. Among 228 patients referred, 163 patients underwent ultrasonography (US) on the same visit and 66 fine needle aspiration cytology (FNAC) studies (57 under US guidance) were done. One hundred ninety-eight (87%) patients made a single visit to the clinic for diagnosis. One hundred twenty-five were discharged or referred elsewhere after the visit and 21 underwent surgery; the remaining 52 patients were followed up. There were 7 thyroid cancers and 2 lymphomas diagnosed. We have concluded that the joint ultrasound-surgery clinic provided an effective outpatient thyroid service with fewer hospital visits.
Thyroid nodules are a very common finding. Palpable nodules affect about 3–4% of the population, nonpalpable nodules up to 25–40% of the population, and over half the population with clinically normal thyroids have nodules identified at autopsy.1–5 Although the vast majority of these nodules are benign, the number of patients referred for secondary care appears to be increasing. Probable reasons include increased health awareness, incidental thyroid nodules found on imaging performed for other reasons, and the difficulty in reassuring patients based on clinical assessment only in primary a care setting as there is a risk of missing a cancer. Thyroid cancer incidence is increasing, which has been mainly ascribed to increasing detection of papillary carcinoma using ultrasonography (US) and fine needle aspiration cytology (FNAC).6,7 However, the incidence of clinically important thyroid cancer (cancers that can affect the life expectancy of the patient) appears to be relatively stable, as the mortality from thyroid cancer had been constant since 1975. 7
There are similarities between palpable breast lesions and thyroid nodules with regards to assessment. Both usually require triple assessment: clinical (history and examination), imaging, and biopsy (FNAC or core biopsy). Certainly the concept of multidisciplinary breast clinics is not new; rapid-diagnosis or “one-stop” clinics staffed jointly by breast surgeons and breast radiologists that offer triple assessment on a single visit have been in place in the United States and United Kingdom for many years. They provide an excellent diagnostic service with a very low incidence of missing a cancer diagnosis. 8 All diagnostic investigations are performed on a single visit. Patients with benign conditions are discharged. In the usual outpatient setting for a thyroid nodule, however, patients will have to make multiple hospital visits; first to see the surgeon and then for imaging and/or needle biopsy studies. We are reporting the results and performance of establishing a one-stop thyroid clinic staffed jointly by a consultant endocrine surgeon and consultant head and neck radiologist.
Methods
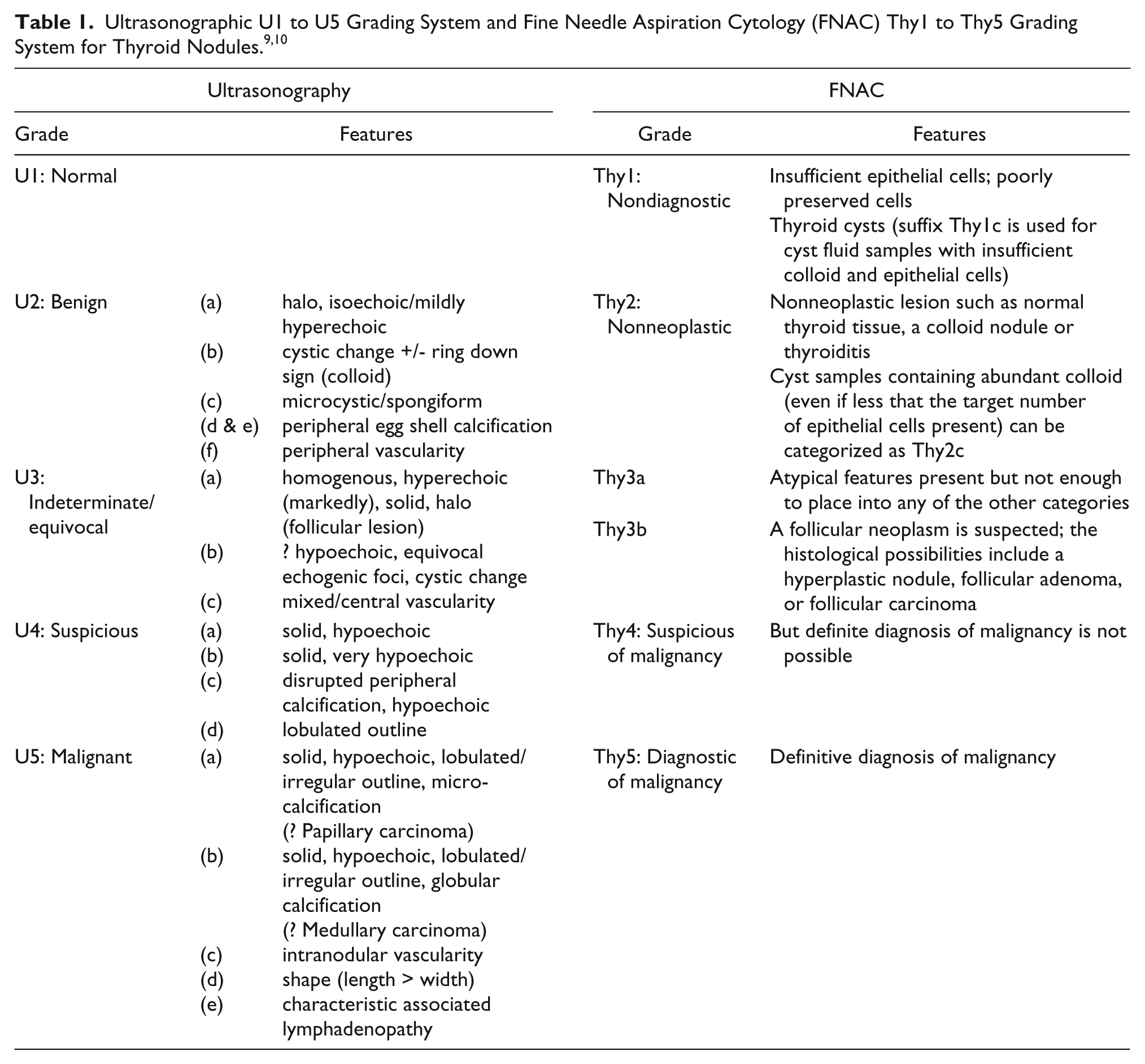
The electronic case notes and other records on all new referrals to the thyroid clinic were reviewed over a period of 14 months from September 2011 to December 2013. (The clinic was established in 2010.) Data collected included the patient population referred, tests done prior to referral, presenting complaint, assessment process, and the outcome. All patients were initially seen by the surgeon and, if indicated, an US examination was done by the consultant radiologist. FNAC, when deemed necessary, was done under US guidance. If US was done, patients were seen again by the surgeon with a formal written scanning report available. The US appearances were coded from U1–U5 depending on the degree of suspicion (Table 1). 9 Patients were informed of the clinical and US assessment results in the clinic. Patients who had a FNAC were either given a follow-up appointment for results (if the lesion was clinically or sonographically worrying) or were contacted by letter with the results. FNAC results were also coded from Thy1 to Thy5 by the reporting pathologist depending on the degree of suspicion (Table 1).9,10 The electronic case notes of all study patients were reviewed again at the end of March 2015 to see whether there were any thyroid cancers missed in the original assessment.
Results
Two hundred twenty-eight patients were seen; 219 were referred by general practice physicians and 9 by other hospital physicians. Of these, 183 were referred with a history of a neck lump and others with a multitude of neck symptoms. In 163 out of 228 patients, a neck lump was present on clinical examination. Nearly a quarter (24%) of the patients referred had not had a recent thyroid function test performed and most (93%) had no thyroid antibody levels done. Twenty patients had already had the US done (usually at the request of the referring doctor) at the time they were first seen. Among the other 208 patients, 163 underwent US on the same visit. US was not considered necessary in 20 patients and 25 patients came back on a separate occasion for the US, thus did not receive a true “one-stop” service. This was due to multiple factors, such as the scanning facility being overloaded with more than the expected number of patients requiring FNACs or patients arriving late for their appointment. US was sometimes requested even when a neck lump was not palpable to investigate other symptoms. Sixty-six FNACs (57 under US guidance by the consultant radiologist) were performed. Patient outcomes are summarized in Table 2.
Outcome of Assessment Process.
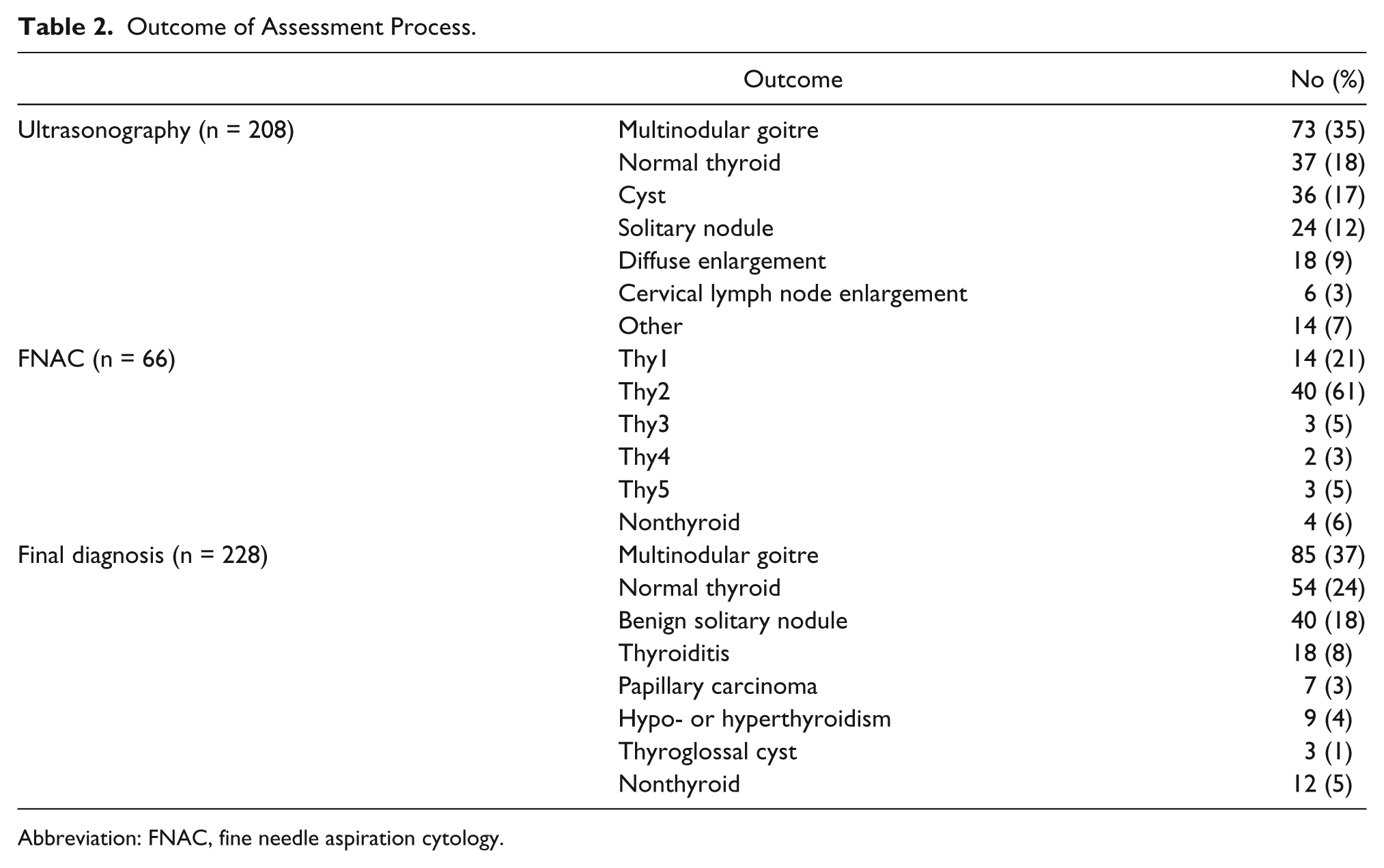
Abbreviation: FNAC, fine needle aspiration cytology.
One hundred and ninety-eight (87%) patients made a single visit to the clinic for diagnosis. Among 228 patients, 125 were either discharged back to their primary care physician or referred to an appropriate specialty (such as endocrinology or oncology) after the visit, 21 underwent surgery and others were followed up. There were 7 thyroid cancers and 2 lymphomas. No missed thyroid cancers were reported in those patients who were discharged by the time of final review in March 2015.
Discussion
Many thyroid nodules require ultrasonographic (US) assessment often with US-guided fine needle aspiration cytology (FNAC). In the usual outpatient setting, patients make several hospital visits, first to see the surgeon, and then for the US +/- FNAC. Despite the fact some patients in this study (11%) did not receive a one-stop service, 87% of patients seen in this specialist combined clinic only made a single visit to the clinic for diagnosis and 55% of patients seen were either discharged or referred to another specialty following assessment. The majority of the patients (96%) were referred by primary care physicians with a suspected thyroid nodule. There were some inappropriate referrals in that 66 patients turned out to have a normal thyroid or a nonthyroid problem following assessment (Table 2). In addition 24% of patients did not have a thyroid function test (TFT) requested by the physician who made the referral; in these patients TFT had to be requested from the clinic. Having a recent thyroid function result when the patient is in the clinic allows further reassurance of patients and avoids the need to contact the patient after the visit with the results. Thus improvement in the referral practice is likely to further improve the efficiency of this clinic.
Clinical assessment alone is not adequate to rule out thyroid cancer in a patient presenting with a thyroid nodule and US has now become an important part of the assessment. It can help distinguish benign from malignant nodules, help to determine which nodule(s) would require FNAC and allows better targeting, improving the diagnostic accuracy compared with palpation-guided FNAC.11,12 To meet this need for combined assessment, surgeon-performed US guided FNAC is increasingly used in some countries. The adequacy and diagnostic accuracy rates of FNAC performed by these physicians appear to match that done by radiologists.13,14
However, US was not used just to improve the quality of the FNAC. Significant weight was placed on the expert radiologist’s opinion on deciding whether to perform repeat FNAC, a core biopsy or diagnostic surgery when the cytology was indeterminate (Thy3 or 4) or thought to be nonrepresentative (discordant result with US appearances or clinical findings). As no single US feature is diagnostic of thyroid malignancy, a number of factors as well as a comparison with previous imaging (when available) is necessary for the decision-making process. Such expertise may not be provided by the relatively short training required for nonradiologists performing US. In addition, more advanced and evolving US techniques such as elastography are useful in differentiating malignant nodules from benign 15 may be beyond the scope of training of nonradiologists. Assessment of cervical lymph nodes in cases of suspected thyroid cancer with FNAC of suspicious node(s) can also be done by a radiologist in the same sitting. 9 In this multispecialty clinic scans were done by a trained consultant head and neck radiologist. As a result of such service, the clinic was able to reassure and discharge the vast majority of the patients after a single visit with confidence in this study. The opportunity provided by this joint clinic to discuss difficult/complex cases promptly with the radiologist also proved very useful.
Immediate reporting of cytology was not available from this clinic. Addition of this service likely would have reduced the relatively high inadequacy rate (Thy1 results) of 21% in our study. 16 It would have also reduced the need for patients to make a return visit to the hospital for repeat FNAC and further improved the diagnostic efficiency of the clinic. In addition patients could be discharged with all results being available on the day of the visit, avoiding an anxious wait on their part. In this study patients were subsequently sent the results of the FNAC when it became available; immediate reporting of FNAC would make this unnecessary.
Conclusion
Although multidisciplinary clinics are not a new concept, we could not find any reference to a combined thyroid clinic in the literature. Setting up of this clinic did not require any additional resources as there was no extra work for the surgeon or the radiologist. Historically ultrasonographic scans requested by the surgeon from the surgical clinic were performed by the consultant radiologist on a different day to when the surgical clinic took place. It required only some simple adjustment in the work schedules of the surgeon and the radiologist to bring the surgical clinic and the ultrasonography together to set up the joint clinic. In conclusion, in a group of patients referred with thyroid nodules to a specialist combined sonography-surgery clinic staffed by a consultant head and neck radiologist and thyroid surgeon, 87% of patients only made a single visit to the hospital for diagnosis. A joint “one-stop” thyroid clinic appears to be a very effective way of providing an outpatient thyroid service. The majority of patients would likely be diagnosed on a single visit and most could be discharged following the assessment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.