
Abstract
Intrauterine devices (IUDs) have had a controversial history but are regarded as a safe, effective form of contraception for all women. IUDs have many benefits, but at the same time, risks and complications may occur in a small percentage of women. The case study first presents a patient with an IUD that perforated the uterus and then offers a discussion of the risks and benefits of IUD contraception.
An intrauterine device (IUD) is a contraceptive device that is positioned in the endometrial cavity, and it is designed to prevent a fertilized egg from implanting into the uterus. The IUD has taken many forms since it was first utilized as a method of contraception. Using an IUD for contraception has many benefits and, at the same time, associated risks.1–4
Case Report
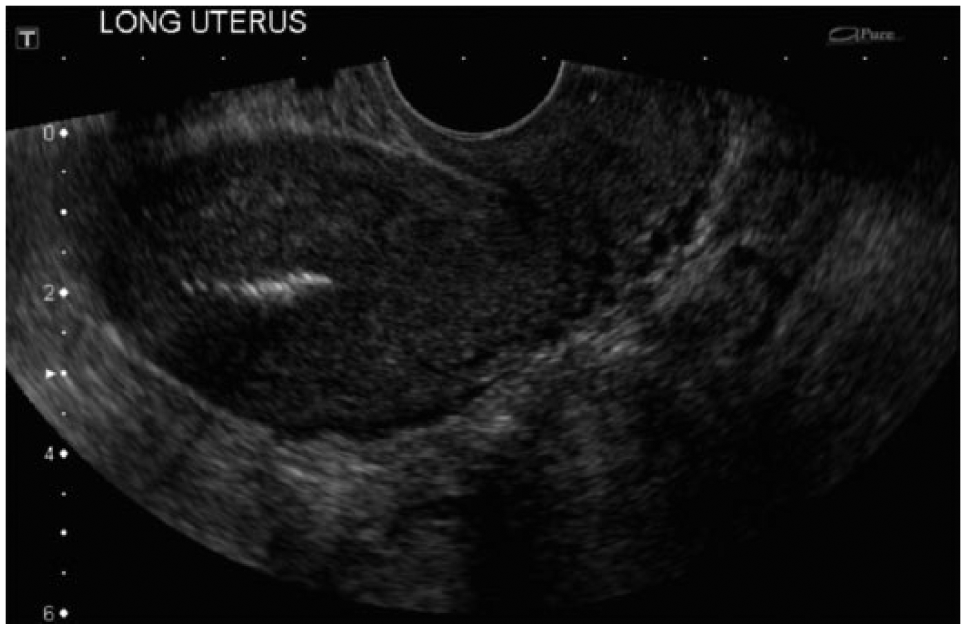
A young woman in her midthirties presented to the emergency room with abdominal pain and an inability to feel the strings of her IUD. The emergency room physician ordered a pelvic sonogram and an abdominal/pelvic radiograph to check the position of the IUD. The pelvic sonogram was done with a Toshiba Xario system (Toshiba Medical Systems, Otawara, Japan), with 5-MHz transabdominal and 9-MHz transvaginal probes used for imaging. The pelvic sonogram showed an echogenic focus with shadowing noted within the endometrium (Figures 1-3). Per the original interpretation of the radiologist, this echogenic area and shadowing were reported to be the IUD itself. The abdominal/pelvic radiography, which was performed immediately after the pelvic sonogram, showed a displaced IUD perpendicular to the uterus (Figure 4); the ultrasound report was subsequently amended with this new information. The patient was taken to surgery, where the IUD was removed. Unfortunately, follow-up was unavailable after the patient was discharged from the facility.

Longitudinal transvaginal gray-scale image of the uterus, showing echogenic foci with significant acoustic shadowing initially reported as the patient’s intrauterine device.
Similar longitudinal transvaginal gray-scale image of the uterus, showing the same echogenic foci with acoustic shadowing initially reported as the patient’s intrauterine device.
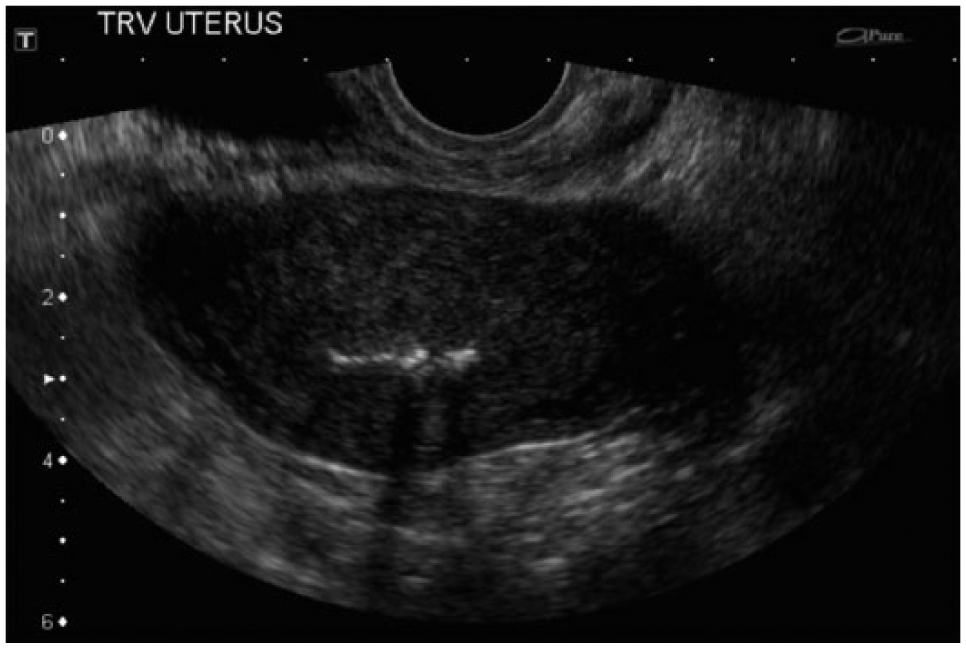
Transverse transvaginal gray-scale image of the uterus, showing that same echogenic foci with more punctate acoustic shadowing initially reported as the patient’s intrauterine device. (This report based on Figures 1–3 was later amended according to the plain film radiograph shown in Figure 4.)

Plain film abdominal/pelvic radiograph showing a displaced intrauterine device, oriented perpendicular to the uterus.
Discussion
Many forms of contraception, or birth control, are on the market today—including not only hormonal and nonhormonal methods but also daily and long-acting reversible options.1–7 Hormonal methods comprise daily pills, dermal implants, injections, and IUDs with hormones, and nonhormonal contraception devices include barrier methods and copper nonhormonal IUDs. The IUD has been available for contraception for >50 years in various forms. Modern IUDs are considered a highly effective and safe method of contraception for all women (comparable with oral contraceptive pills for some women), including nulliparous women and adolescents.5–7 The popularity of the IUD has varied over that time because of a number of factors and associated complications, such as perforations of the uterus and infections.
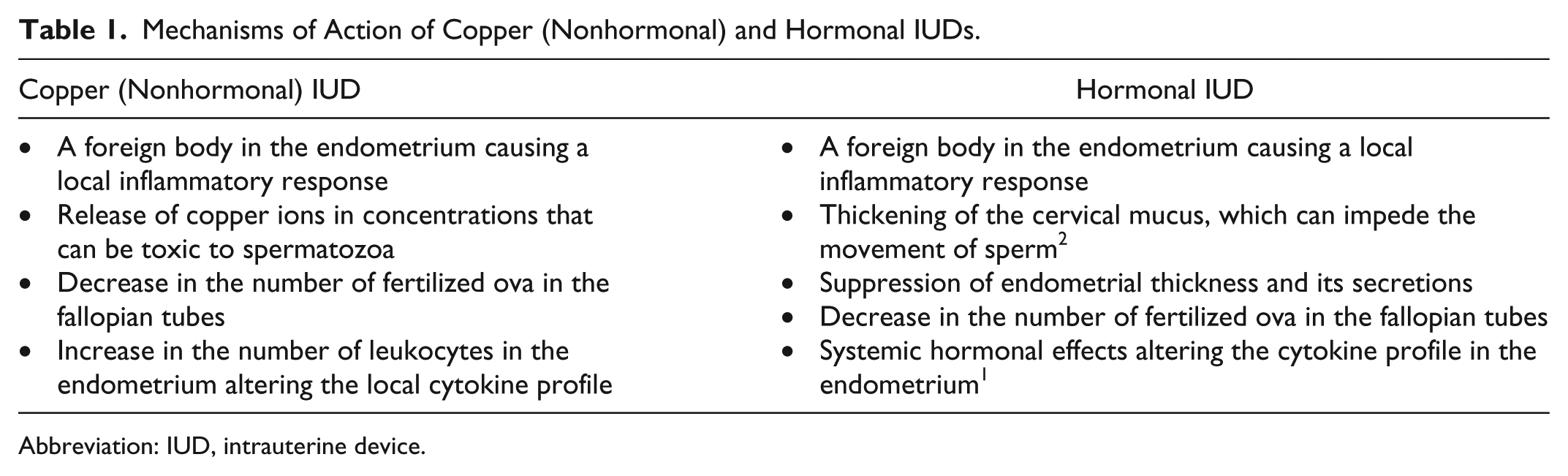
Two main forms of IUDs are in use today, with their functions summarized in Table 1.1,8 Both copper (nonhormonal) IUDs and hormonal IUDs cause local inflammatory reactions that help to prevent pregnancy. Furthermore, copper ions released from that type of IUD become concentrated enough in the genital tract fluids to be toxic to spermatozoa. In addition to the local inflammatory effects of hormonal IUDs, these devices are able to release their drug and cause some systemic effects. Both types of IUDs are primarily thought to decrease the rate of fertilization and negatively affect the survival an embryo prior to reaching the uterus, rather than the outright destruction of an embryo in the uterus.
Mechanisms of Action of Copper (Nonhormonal) and Hormonal IUDs.
Abbreviation: IUD, intrauterine device.
Several benefits are associated with the use of IUDs. The patient does not need to remember to take daily pills or get repeated contraceptive hormonal shots. The IUD remains highly effective in the prevention of pregnancy for an extended period. In the case of adolescents, the Food and Drug Administration has approved the use of IUDs in women as young as 16 years old.5,6 IUDs also do not interfere with the metabolism of oral medications, such as antibiotics. IUDs are safe to insert in the immediate postpartum period (with both vaginal and caesarean deliveries) and are safe to use while breast-feeding, with no differences between the volume or type of milk produced and the length of breast-feeding time, unlike some other forms of birth control. 7 Finally, some health care providers are also using hormonal IUDs for the treatment of abnormal uterine bleeding, and IUDs have been proposed for use in the treatment of endometrial carcinoma. 9 The slow-releasing hormones of the hormonal IUDs—often levonorgestrel, which has progestogenic, androgenic, antioestrogenic, and antigonadotropic biological activities 9 —have been shown to decrease endometrial thickness, consequently decreasing abnormal bleeding and increasing a patient’s quality of life.
Potential side effects and disadvantages have been documented with IUDs as well.3,4,6,10,11 For example, expulsion of the IUD is more common with insertion during the recent postpartum period and so depends on the skill of the health care provider inserting it. The uterus may perforate, which also appears to depend on the proficiency of the health care provider. Additionally, IUDs may be the cause of dysmenorrhea with abnormally heavy bleeding, and ectopic pregnancies have been reported with an IUD in place.
Besides the complications above, several contraindications exist for IUD insertion and use—primarily, current pregnancy, pelvic inflammatory disease, postpartum or postabortion sepsis in the past 3 months, current sexually transmitted infections, undiagnosed abnormal vaginal bleeding, malignancy of the genital tract, and any distortion of the pelvic tract that would make the insertion of the IUD problematic.5,7
When patients do experience complications with their IUDs, such as pain and abnormal bleeding, the physician first checks to see if the IUD strings are visible through the cervix. If they are not, the provider may order pelvic sonography to visualize the position of the IUD. The IUD should be located within the endometrium of the uterus, with no part extending into the myometrium or cervix. The main shaft of the IUD is typically easily seen on standard sonography; however, the arms of the IUD may not be seen as readily, because of their position relative to the ultrasound beam. The advent of three-dimensional sonography has allowed the sonographer and radiologist to visualize the endometrium in multiple planes, allowing one to see if the IUD is in its proper location or if it has migrated to an abnormal position with some part of it penetrating outside the endometrial cavity. 10
If the IUD is not visualized by pelvic sonography, then a plain film radiograph is often ordered to see if the IUD has perforated the uterus and is in an ectopic location. IUDs are made of a radiopaque material that allows them to be readily visualized on a radiograph. The radiograph lets one determine where the IUD has migrated and if it has indeed perforated the uterus. 11 Other imaging modalities, such as computed tomography, can be used if there is a concern for an abscess, fistula, adhesions, or some other complication. A computed tomography also allows the physicians to see if the IUD has damaged any other organs (e.g., bowel or bladder) after it left the uterus. If the patient is possibly pregnant (due to the movement of the IUD), magnetic resonance imaging can be used to assess the position of the IUD—for either the copper IUD or the plastic hormonal IUD, depending on the strength of the magnet. All these imaging modalities work in conjunction to allow for the best diagnosis and treatment of the patient and will ideally move toward a better outcome for the patient in the long run.
Conclusion
The use of IUDs over time has shown them to be a safe and effective form of contraception for all women, including nulliparous women and adolescents, and assists in the treatment of abnormal uterine bleeding for some women. Despite the risks associated with the use of IUDs, their benefits seem outweighed for most women. In the event of a complication, a variety of imaging studies can be utilized to find the location of the IUD, with sonography typically being the first choice
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.