
Abstract
Obstetric sonography has a long-standing reputation assisting in the detection of chromosomal abnormalities in utero. Additional diagnostic testing can be performed to confirm a genetic anomaly, including noninvasive prenatal testing, nuchal translucency, and amniocentesis. Comprehensively studied chromosomal abnormalities include trisomies 21, 13, and 18 and monosomy X. Although chromosomal abnormalities cannot be treated, they can be managed and monitored by serial sonograms and genetic counseling prior to delivery, allowing for preparation for a special needs child. This case study presents a fetus with multiple anomalies, including a rare presentation of cystic hygroma. In this specific case, the patient refused a genetic amniocentesis, leaving the cause(s) of the multiple anomalies unknown.
Sonography is the most common imaging modality of choice for obstetric patients because it provides noninvasive, radiation-free images of fetal structures. Sonography has a long history in the detection of congenital and acquired anomalies in utero.1–4 Many of these anomalies are chromosomal in origin and can be detected through the use of ultrasound in correlation with blood testing, nuchal translucency, and genetic amniocentesis.5–9
Case Report
A 27-year-old gravida 3 para 2 (G3P2) patient presented to a high-risk maternal-fetal medicine (MFM) clinic with a history of preeclampsia and two previous caesarean sections. Current gestation dated 12 weeks and 1 day according to her last menstrual period (LMP) and 12 weeks and 3 days according to crown rump length (CRL) measurements, as seen in Figure 1. A viable fetus was seen in the uterus with a heart rate of 165 beats per minute (bpm). The first-trimester screening revealed a cystic hygroma and an abnormal amount of fluid with an enlarged space in the fetal neck measuring 5.08 mm, suggestive of an abnormal nuchal translucency (Figure 2). After discussion with a perinatologist and genetic counselor, the patient elected to have noninvasive testing to predict the risk for chromosomal abnormalities. The results showed low-risk marks for every category, including trisomies, and the fetal sex was genetically female. On the basis of these findings, the patient was referred back to the high-risk MFM clinic for an 18- to 22-week sonographic assessment to further assess the fetal anatomy.
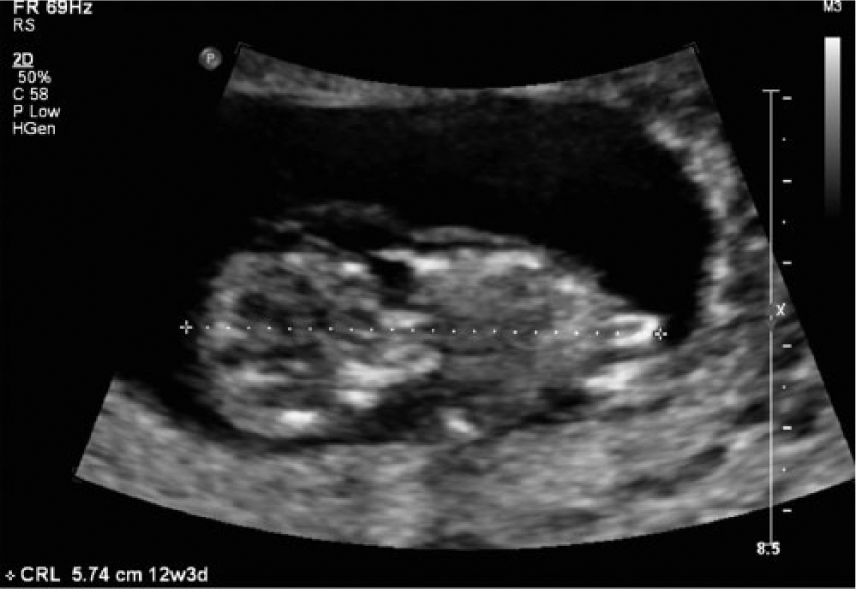
Gray-scale image of the fetal crown rump length measurement of 5.74 cm corresponding to fetal age of 12 weeks 3 days, which correlated well with the gestational age according to last menstrual period.

Measurement behind the fetal neck demonstrating an abnormal amount of lymphatic fluid with an enlarged (5.08 mm) space suggesting an enlarged nuchal lucency. (Note that the measurement in this image is not according to the necessary protocol for a true nuchal lucency measurement, which requires, among other parameters, that the measurement be obtained from the back of the fetal neck with the fetus in midsagittal plane and showing only the fetal head and upper thorax.).
The patient returned to the clinic 7 weeks later at the gestational age of 19 weeks and 3 days for a detailed morphology scan and to follow up the cystic hygroma. Indications for this examination also now included possible maternal cardiomyopathy and multiple congenital anomalies. A fetal heart rate of 144 bpm was measured. The fetus measured in the 62nd percentile for gestational age based on femur length (FL), abdominal circumference (AC), biparietal diameter (BPD), and head circumference (HC) measurements. Although normal heart rate and fetal growth were shown, multiple congenital anomalies were also visualized. The fetus appeared hydropic with a large cystic hygroma seen at the level of the BPD and HC measurements (Figure 3). Both pleural and pericardial effusions were visualized. The presence of abdominal ascites surrounding the bowel of the fetus was also demonstrated, with generalized anasarca (Figures 4 and 5). Clubbed and/or clenched hands were observed, the right foot appeared clubbed, and visualization of left foot was not possible. Echogenic lungs and abnormal curvature of the spine were also noted. Endocardial fibroelastosis of the ventricles in the fetal heart was probable. Throughout the examination, little to no fetal movement was seen.

Cross-sectional gray-scale image showing a large cystic hygroma. Measurements of the biparietal diameter of 4.52 cm and the head circumference of 16.17 cm demonstrate a normal growth pattern in the 19-week, 3-day fetus.

Cross-sectional abdominal gray-scale image showing the presence of ascites in the fetus surrounding the fetal bowel.

Cross-sectional abdominal gray-scale image showing an abdominal circumference of 14.39 cm, which appears consistent with a gestational age of the fetus of 19 weeks and 3 days. Also note the significant edema surrounding the fetal abdomen.
The sonographic findings of the first- and second-trimester sonograms were presented to the patient and discussed regarding the fetus’s increased risk for aneuploidy. The obstetrician recommended a genetic amniocentesis be performed to allow for a more accurate diagnosis; however, the patient declined to undergo the procedure. The patient elected to continue the pregnancy regardless of fetal condition. A follow-up sonogram in one week was recommended to evaluate any hydropic changes in the fetus, which showed a viable fetus with no significant changes compared with the previous sonogram. The patient later decided to seek a second opinion and discontinued care at the original high-risk MFM clinic. Because of this change in caregivers, a complete definitive diagnosis and follow-up is not available.
Discussion
Chromosomal anomalies can be observed by sonography and are some of the most commonly seen disorders in the field of obstetric sonography.2,4,10 Sonographic evidence of these anomalies is often followed up by other forms of testing such as noninvasive blood tests and/or genetic amniocentesis. The incidence of recognizable chromosomal abnormality in unselected newborns is 9.2 per 1000, of which 75% have autosomal and 25% have sex chromosomal abnormalities. 10
One of the most common first-trimester sonographic evaluations is testing for nuchal translucency, which can be evaluated in the 11th through 13th week of pregnancy. 11 Using appropriate techniques, the sonographer evaluates an area in the back of the fetus’s neck that contains lymphatic fluid.12,13 A normal amount of fluid is considered 3 mm or below. Common abnormalities associated with enlarged nuchal translucency are Down syndrome and Turner syndrome. Nuchal translucency usually also involves a blood draw that compares the patient’s age, race, and family history to establish risk for genetic disorders such as Down syndrome and spina bifida. The patient may choose to undergo a genetic amniocentesis after results have come back as high risk.
Cell-free fetal DNA is one of the blood tests used to screen for chromosomal anomalies and can be tested as early as nine weeks’ gestation. 6 DNA technology evaluates single-nucleotide polymorphisms, or SNPs, to distinguish maternal from fetal DNA. 7 Extra or missing chromosomes in the fetus’s DNA that are linked to genetic abnormalities can be detected; the typical accuracy of such screening tests is 98% to 99% when testing for Down syndrome, trisomies 13 and 18, and triploidy. 9 After determination of a high-risk pregnancy through cell-free DNA testing, the patient is commonly referred for amniocentesis or chorionic villus sampling later in the pregnancy.
Genetic amniocentesis is typically performed between weeks 15 and 22 of gestation. The procedure uses a fine needle that is inserted through the abdominal wall into the uterus using sonographic guidance. A sample of the amniotic fluid is taken from the amniotic sac, which can then be tested for genetic conditions. Amniocentesis is more than 99% accurate in detecting anomalies. In the case presented, the patient refused a genetic amniocentesis, which makes diagnosing the fetal anomaly more difficult.
Chromosomal abnormalities can be classified into variations, such as trisomy and monosomy. Trisomy is the addition of one chromosome within a normal pair. Well-known trisomies include trisomies 21, 18, and 13.10,14–16 Trisomies 13 and 18 present on prenatal ultrasound with multiple congenital malformations and commonly result in an intrauterine fetal demise (IUFD) or stillbirth. 15 Down syndrome is the mildest and most common form of trisomy (trisomy 21) and is survivable with mild to moderate physical and mental disability. Prevalence of Down syndrome occurs in approximately 1 in 700 births in the United States. 17 Trisomy 18, also known as Edward syndrome, is caused by meiotic disjunction. 10 The incidence of Edward syndrome occurs in 1 of every 2500 pregnancies in the United States and about 1 in 6000 live births. The occurrence of stillbirths becomes more common with trisomy 18 in the second and third trimesters. 15 Trisomy 13, or Patau syndrome, is the most lethal and causes severe mental and physical abnormalities.14,15 The incidence of trisomy 13 occurs in 1 in every 16,000 newborns, making it the least prevalent of the trisomies. Most cases of trisomy 13 are not inherited and result from random events during the formation of eggs and sperm in healthy parents. 14 Fetuses diagnosed with trisomy 13 will demonstrate heart defects, brain or spinal cord abnormalities, microphthalmia, polydactyly, cleft lip or cleft palate, and hypotonia. Many infants born with trisomy 13 die within the first days of life; only 10% of surviving infants with this condition will live past the first year. 15
Monosomy presents when there is a loss of one chromosome in the pair. The most common form of monosomy is Turner syndrome, also known as monosomy X. 18 Turner syndrome is classified as a sex chromosome abnormality. Cystic hygroma is strongly associated with Turner syndrome, trisomy 21, trisomy 18, and Noonan syndrome. 18 Fetal cystic hygroma associated with nonimmune hydrops fetalis (NIHF) has a higher incidence of aneuploidy, particularly Turner syndrome or trisomy 21. About 30% to 70% of fetuses with cystic hygroma have chromosomal aberrations. 19 Cystic hygroma accompanied by NIHF in the second trimester is associated with a very poor prognosis as described in a case report from 2006. 19 A sonogram done in this case showed a large cystic hygroma, bilateral pleural effusions, pericardial effusion, ascites, and polyhydraminos. Following an amniocentesis, the pregnancy was terminated and a fetal autopsy was performed. The female fetus dated 16 weeks’ gestation with remarkable multiloculated cystic hygroma. Severe generalized edema was present. Upper and lower limb shortening was also demonstrated, measuring two weeks behind gestational age. Facial dysmorphism in the form of low-set ears, hypertelorism, depressed nasal bridge, and micrognathia was apparent. Karyotyping of the fetus revealed the 45X chromosome was affected, diagnosing Turner syndrome.
Trisomy and Turner syndrome primarily occur by nondisjunction or translocation. Nondisjunction trisomy occurs with an error in cell division resulting in a reproductive cell with an abnormal number of chromosomes. Translocation trisomy can be inherited. A person with a balanced translocation involving a specific chromosome has an increased chance of passing extra material from that chromosome to his or her children. 20
Genetic counseling is an important step in the process of understanding chromosomal anomalies as these types of genetic anomalies can be explained and understood by the patient with this help. 20 Genetic counselors are provided by MFM clinics to educate the patients on specific disorders that have been confirmed by sonograms and other tests and procedures. Genetic counselors assess the probability of transmittance of disease by researching family medical histories and the etiology of genetic disorders. Counselors also provide information and support to the patients so that they may make informed decisions about their health care and the well-being of themselves and the fetus.
Conclusion
Sonography plays a critical role in the evaluation and detection of chromosomal anomalies observed in the fetus. The first-trimester scan suggesting an enlarged nuchal translucency also showed a cystic hygroma, predicting the high possibility of a chromosomal abnormality. In this instance, noninvasive blood testing did not demonstrate specific chromosomal abnormalities, and an amniocentesis procedure would have been beneficial to correlate with obstetric sonography to obtain a better diagnosis. Based on the sonographic data, possible diagnoses include trisomy 13, trisomy 18, or Turner syndrome, but because of the patient’s decision to discontinue care at the MFM clinic, the outcome of the pregnancy is unknown.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.