
Abstract
Trisomy 5p syndrome is a rare chromosomal abnormality with about 40 documented cases. This abnormality is a result of a duplication of the short arm of chromosome 5. Most Trisomy 5p cases are the result of an unbalanced translocation between the duplicated material of chromosome 5 and another chromosome. This case study demonstrates the sonographic features found on a fetus affected with trisomy 5p. It also discusses how genetics play a role in fetuses affected by chromosome abnormalities and why it is important for sonographers to be aware of the contributing factors that can lead to anomalies.
Case Report
A white woman in her mid-30s, G9P2062, presented to the maternal fetal medicine department for an anatomical sonogram at 19 weeks with a history significant for six recurrent first-trimester pregnancy losses. Previous thrombophilia laboratory tests revealed homozygous methylenetetrahydrofolate reductase (MTHFR) variant, normal factor V and prothrombin genotype, normal protein C and S activity, and normal autoimmune lymphoproliferative syndrome panel. The patient was currently taking 4 mg folic acid and 81 mg aspirin daily. No previous cytogenetic studies had been performed on products of conception. Paternal history was significant for a sibling passing away within the first year of life with what was described as a “chromosomal abnormality.” The sonogram showed multiple abnormalities. Findings included bilateral clubfeet, umbilical hernia, echogenic foci in the heart, and mild bilateral pyelectasis (Figures 1–3). Amniotic fluid, placental location, and the rest of the anatomical survey were unremarkable. The patient did not have any maternal first- or second-trimester serum aneuploidy screening. Given the sonographic findings, the patient was referred to a genetic counselor. The patient was counseled that the presence of bilateral clubfeet and an abdominal wall defect elevated her risk of carrying a fetus with a chromosomal anomaly. A priori risk of aneuploidy based on maternal age alone would have been 1:275. The sonographic findings increased her risk of chromosome anomaly by at least by 30%. The option of amniocentesis for definitive chromosome analysis was offered, which the patient accepted. The karyotype demonstrated an unbalanced translocation involving the proximal short arm of chromosome 5 and the distal short arm of chromosome 9. This resulted in an extra copy of the short arm of chromosome 5 attaching to the distal arm of chromosome 9 (46 XY, der(9),t(5;9)(p12;p23)), or trisomy 5p. The known clinical features of trisomy 5p include umbilical hernia and bilateral clubfeet; trisomy 5p will also result in additional anomalies and severe developmental delays. The patient was informed of the variability in the presentation of trisomy 5p and the difficulty in predicting the severity. After much discussion with the genetic counselor and maternal fetal medicine specialist, the couple elected to terminate the pregnancy due to the poor prognosis.
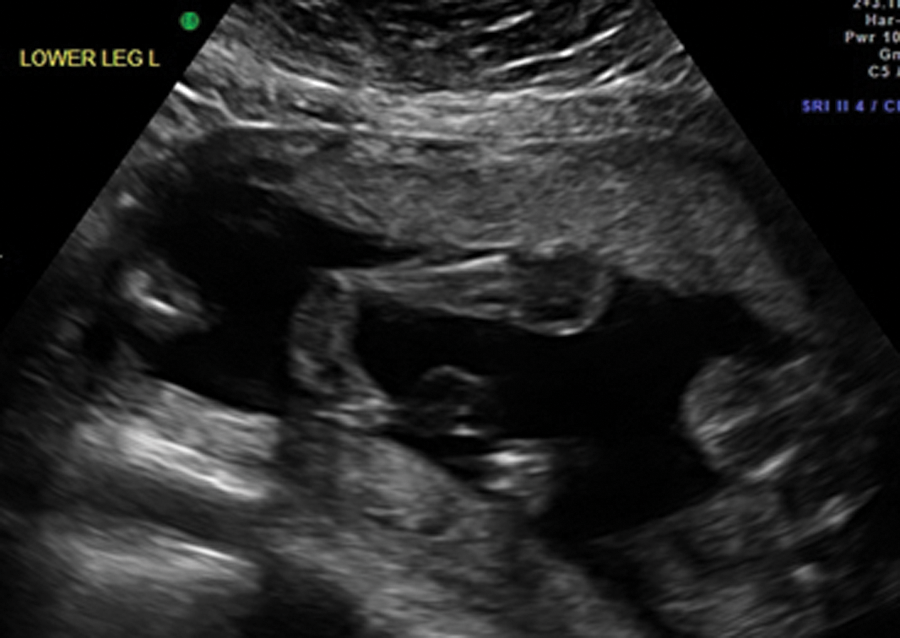
Two-dimensional image showing a clubfoot. The fetus presented in this case was found to have bilateral clubfoot.
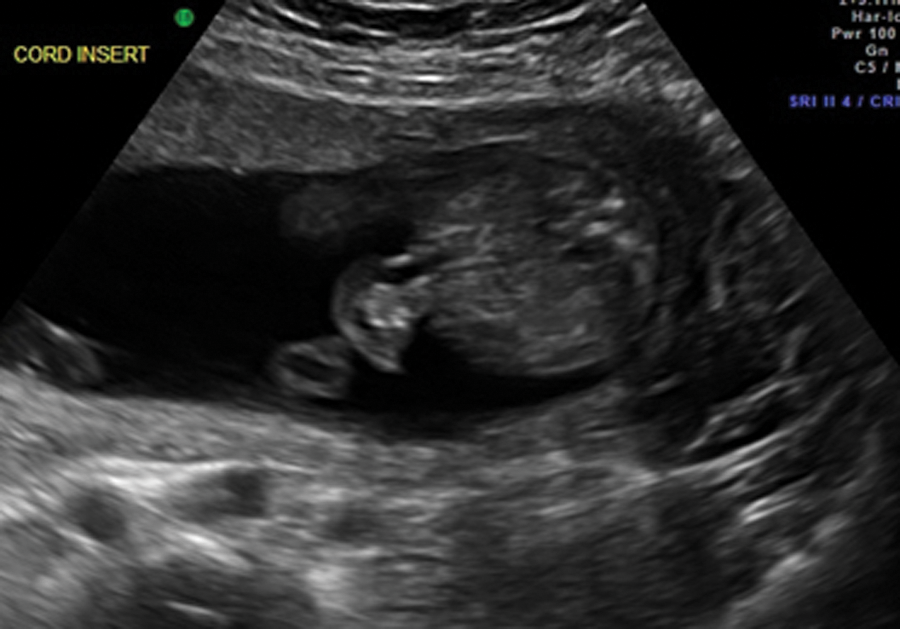
Two-dimensional image of the cord insertion in this fetus. The echogenic material present in the cord is bowel in the cord, representing the umbilical hernia.

Two-dimensional image of bilateral pyelectasis seen in the case presented. The umbilical hernia is also seen in this image.
Discussion
Trisomy of the short arm of chromosome 5 is very uncommon and typically appears in the literature as a case report. 1 The first documented case was in 1964, 2 and there have been only about 40 documented case reports since then.3–6 Most cases involve a translocation involving the short arm of chromosome 5 and another autosome. 7 A small percentage of chromosome anomalies are the result of inherited chromosomal rearrangement, making certain conditions such as trisomy 5p rare. Cases of trisomy 5p are frequently associated with craniofacial, cardiac, renal, and limb abnormalities.5,6,8 Craniofacial findings include macrocephaly, agenesis of the corpus callosum, hydrocephalus, low-set ears, hypertelorism, and micrognathia. Cardiac defects such as atrial-septal defect, renal abnormalities (including pyelectasis), and limb anomalies such as long fingers and clubfoot are also common.
This case involved an unbalanced translocation between chromosomes 5 and 9. Because most cases are often the result of parental chromosomal rearrangement, this couple was encouraged to have chromosome analysis. The father of the baby was found to be a balanced reciprocal translocation carrier. Unbalanced translocations occur in 1:2000 individuals. General population incidence of reciprocal translocation carrier is estimated at 1:625, 9 but 5% to 6% of couples with recurrent pregnancy loss are found to have a chromosomal rearrangement. People who are balanced translocation carriers tend to have histories significant for recurrent miscarriages and birth defects. Such was the case with this patient, who had multiple first-trimester pregnancy losses, and with the father, who had a sibling that died by one year of age from a chromosomal abnormality. This history, the sonographic findings, and genetic testing all led to the diagnosis of trisomy 5p.
As seen in this case report, the fetus presented with bilateral clubfeet and an umbilical hernia. These two anomalies appearing together directly relate to the chromosome 5 translocation. Sonographers need to be aware of associations such as these the better to document the many possible abnormalities that can be demonstrated by a thorough sonographic examination. 10 With the evolution of better technology, more fetal abnormalities are being observed on these targeted scans. These improvements have allowed sonographers to better visualize these defects and have made prenatal diagnosis of certain anomalies more common. With improved 3D sonography, these abnormalities can be demonstrated even more clearly, as with the clubfeet and umbilical hernia seen in Figures 4 and 5.

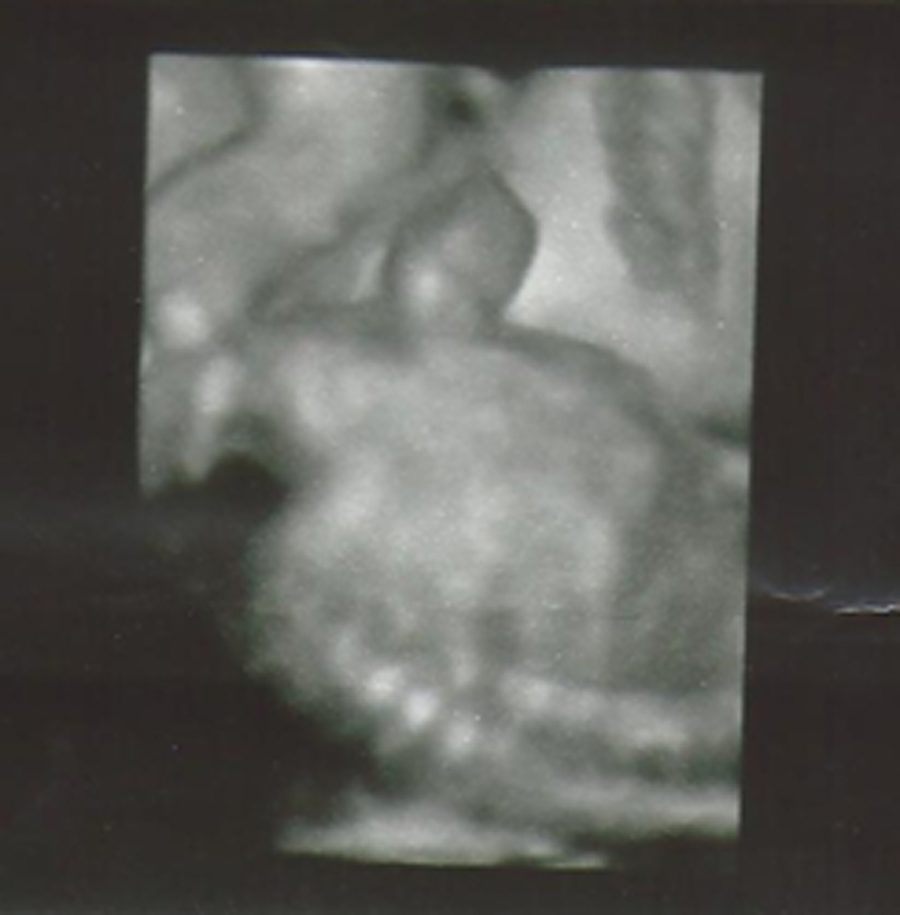
Three-dimensional image of the bilateral clubfeet seen on the fetus in the case presented, a finding known to be associated with the trisomy 5p syndrome.
Three-dimensional rendering of the umbilical hernia seen during the sonographic examination presented. Umbilical hernia is also a classic marker for trisomy 5p syndrome.
In addition to sonography, genetic testing also plays a significant role in prenatal diagnosis. New advancements in cytogenic testing have enabled us to make connections between genetic information and sonographic findings. The visualization of the clubfeet and umbilical hernia directly relates to the chromosome 5 anomaly. Sonographers need to remain observant of the many fetal abnormalities that can occur. In addition to sonography skills, we should be mindful of the supporting genetic information that can be used in conjunction with these targeted scans. By reviewing a complete history on these patients, whether completed by a genetic counselor or sonographer, the sonographer can be made more aware of the potential risk factors that can affect the fetus and allow a more complete evaluation of the pregnancy.
Conclusion
Routine screening for congenital abnormalities has become an established practice, and sonography is the major modality used for this. 5 Targeted anatomical sonography is used to demonstrate both structural abnormalities and soft markers that are used to identify certain fetal anomalies. The presence of clubfeet, pyelectasis, and umbilical hernia seen in the case presented demonstrates the potential impact of such abnormal findings on the outcome of a pregnancy. Improved sonographic technology showed the anomalies in both 2D and 3D. This enhanced the visualization of these abnormalities and provided the patient with a better understanding of the anomalies that were present. Because anomalies can present with many different findings, it is essential that sonographers pay particular attention to the findings of even a “routine” anatomical survey, which may include frequently seen abnormalities such as pyelectasis to more rare findings such as umbilical hernia. Sonographers need to remain aware of the presentation of different fetal anomalies and their association with genetic abnormalities. It is the sonographer’s role in performing these targeted anatomical scans to find these anomalies so patients can have the opportunity to make more informed decisions regarding their pregnancy.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.