
Abstract
A case study of a fetal goiter with successful in utero treatment is presented. The incidence of fetal goiters is rare and can have poor neonatal outcomes due to tracheal and esophageal obstruction. This makes prenatal diagnosis and treatment pertinent. In this case, a solid, homogenous, hypervascular mass is seen protruding from the anterior fetal neck causing hyperextension of the cervical spine. With the use of a percutaneous umbilical cord sampling (PUBS) procedure, the diagnosis of fetal hypothyroidism was established. Successful treatment of the fetal goiter and hypothyroidism with intra-amniotic injections of synthroid prevented tracheal obstruction and the need for an ex utero intrapartum treatment (EXIT) procedure at delivery.
Introduction
A fetal goiter is an abnormal enlargement of the fetal thyroid gland.1–3 Sonography is very useful at detecting fetal neck masses, and the use of 3D technology provides an in-depth evaluation of the mass. Fetal goiters can be easily detected in the sagitial profile view of the fetus. When a sonographer detects a fetal goiter, it is important to document the size and vascularity of the goiter.1,2 More importantly, when a goiter is detected, the measurement of the trachea and the presence of fetal swallowing should be noted. Early detection and treatment of a fetal goiter helps to prevent adverse outcomes, such as polyhydramnios, tachycardia, tracheal and esophageal obstruction, and even neonatal death. 1
Case Study
A patient presented at 21 weeks 5 days for an enlarged fetal neck with a possible neck mass. The patient was of advanced maternal age and was a gravida 2 para 1. The patient’s maternal laboratory values and pregnancy screening laboratory values were normal. The only medication that the patient was taking was a prenatal vitamin and folic acid. The patient’s first child was diagnosed with hypothyroidism shortly after birth with newborn screening and with no evidence of a goiter.
A transabdominal sonogram was performed using a GE Voluson E8 (GE Healthcare Ultrasound, Waukeshaw, Wisconsin, USA). The transducers utilized were curved array RAB4-8-D and the curved array RM6. The examination showed a solid, homogenous, hypervascular mass protruding from the anterior fetal neck causing hyperextension of the cervical spine (Figures 1 and 2). The right lobe of the fetal thyroid measured 2.3 cm × 1.3 cm × 1.3 cm, and the left lobe measured the same at 2.3 cm × 1.3 cm × 1.3 cm. Color Doppler imaging with 3D image processing utilizing glass body rendering showed the fetal thyroid to be somewhat hypervascular (Figures 3 and 4). Three-dimensional imaging was utilized further to demonstrate the large anterior mass protruding from the fetal neck (Figure 5). There were no other fetal anomalies identified.

A gray-scale sagittal image of the fetal profile showing the large fetal goiter (arrows).
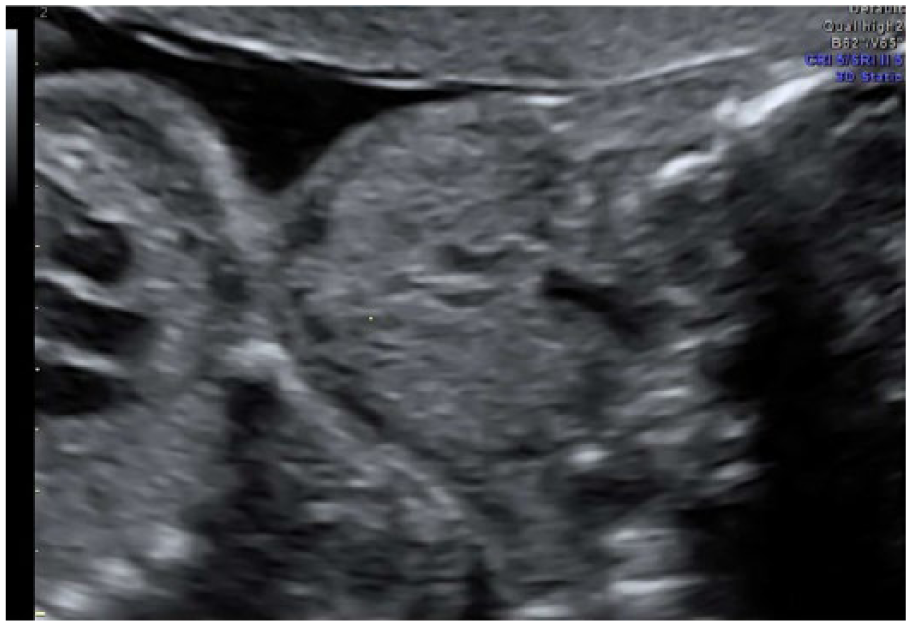
A gray-scale coronal image of the fetal neck showing the bilaterally symmetrically enlarged fetal thyroid.
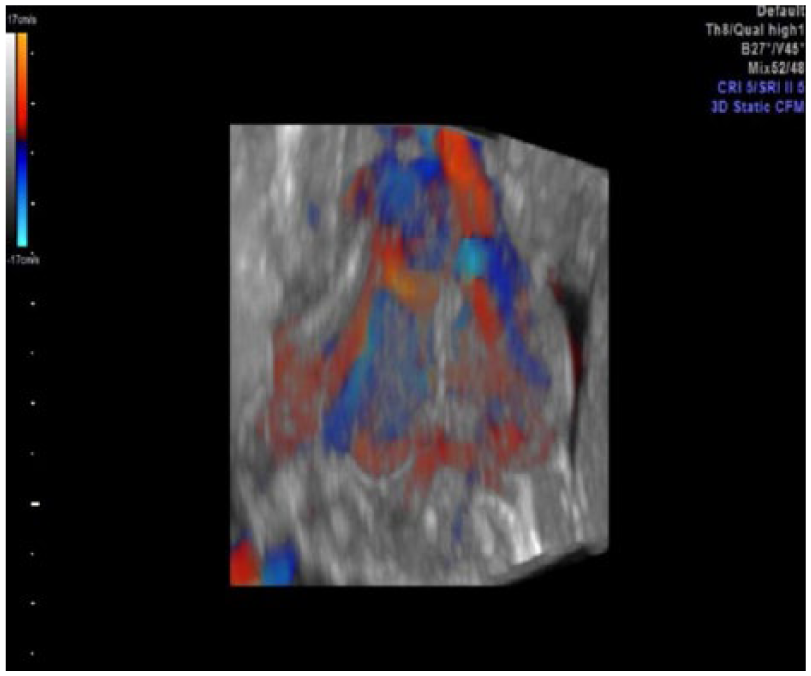
A 3D image of the fetal neck supplemented with color Doppler and using glass body rendering to show the significant hypervascularity of the thyroid.
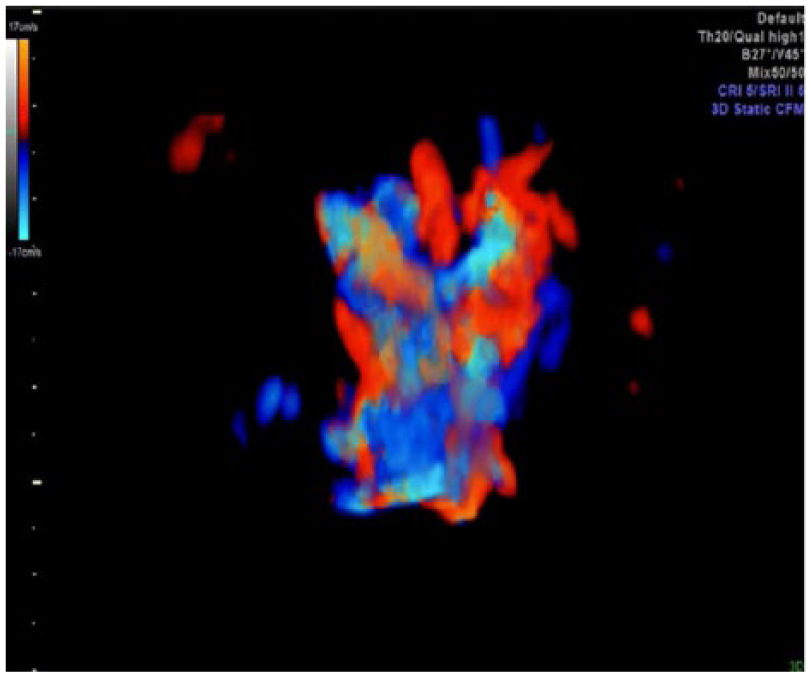
A 3D image of the fetal neck supplemented with color Doppler and using glass body rendering, with removal of soft tissue information, showing the significant hypervascularity of the thyroid.
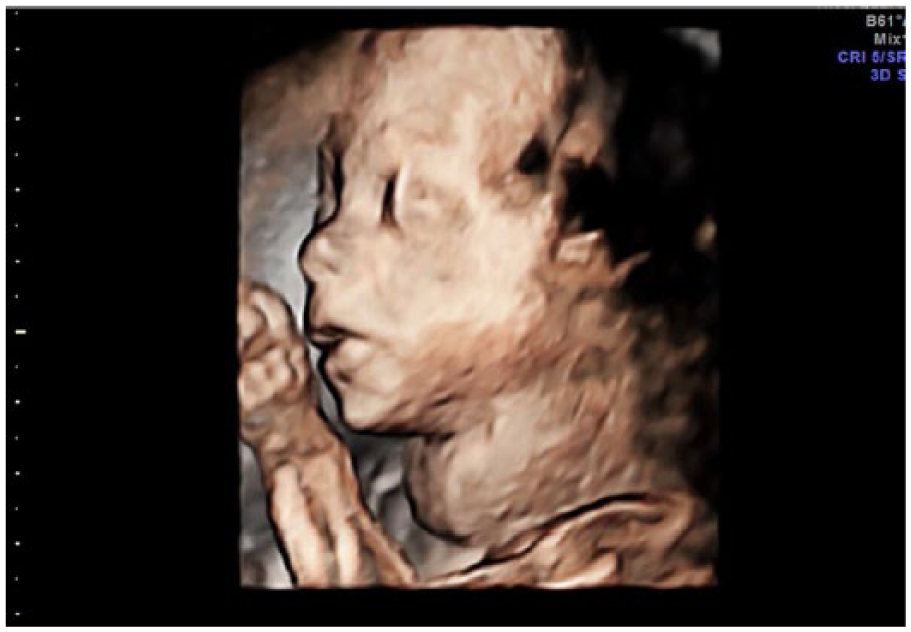
A 3D surface rendered image of the fetal profile at 21 weeks 6 days clearly showing the appearance of a neck mass caused by the fetal goiter.
A percutaneous umbilical cord blood sampling procedure (PUBS) was performed at 24 weeks to evaluate the fetal thyroid levels. The fetal thyroid levels showed hypothyroidism with abnormally low levels of tri-iodothyronine (T3) and tetra-iodothyronine (T4) and a high thyroid-stimulating hormone (TSH). The laboratory values were used to determine the amount of synthroid, a drug used to treat hypothyroidism, which should be injected through an amniocentesis infusion. The first infusion was performed at 24 weeks 6 days with 400 microgm of synthroid injected. Weekly amniocentesis infusions of synthroid were subsequently performed. A follow-up PUBS procedure was performed at 31 weeks 6 days to reevaluate the fetal thyroid laboratory values. The thyroid laboratory levels remained abnormal, and the synthroid injections were increased to 600 microgm. A third PUBS procedure was performed at 33 weeks 5 days and indicated little change in the thyroid laboratory values. Injections of synthroid were increased to 800 microgm, and the amniocentesis infusions of synthroid were continued until delivery at 37 weeks 6 days. The sonogram prior to delivery showed the thyroid to be significantly decreased in size with the right lobe measuring 2 cm × 0.9 cm × 0.98 cm and the left lobe measuring 2 cm × 0.9 cm × 1.1 cm (Figure 6). The fetus was delivered via caesarean section with no need for an ex utero intrapartum treatment (EXIT) procedure.
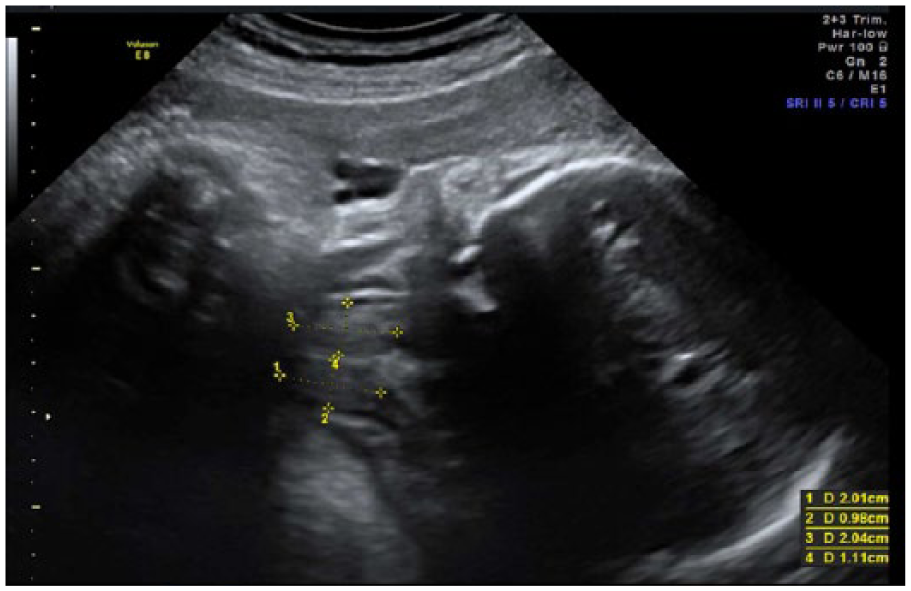
A gray-scale coronal view of the fetal thyroid just prior to delivery showing the reduction in size to a more normal 2 cm × 1 cm.
Discussion
Fetal goiters are rare. They can arise from maternal Grave’s disease, Hashimoto thyroiditis, iodine ingestion, propylthiouracil exposure, and methimazole exposure. Fetal goiters can also be caused from primary fetal hypothyroidism.1,2 The prevalence of congenital hypothyroidism presenting with thyroid enlargement is approximately 1 per 40 000 and is found in only 10% to 15% of all cases of congenital hypothyroidism. 3 An enlarged fetal thyroid can cause tracheal and esophageal compression that can result in polyhydramnios. At delivery, respiratory compromise can also occur as a result of trachea compression by the enlarged thyroid gland. 4 Fetal hypothyroidism may cause intrauterine growth restriction, with accelerated bone maturation, intrauterine death secondary to cardiac failure or thyrotoxicosis, and craniosynostosis. 5
Sonographically, fetal goiters typically present as anterior, midline, symmetrical, homogenous, hypervascular neck mass. 1 Sonographically, a cervical teratoma may appear similar to a fetal goiter. However, a cervical teratoma will present as a hypovascular, heterogeneous, cystic, and solid mass that may have calcifications; they are typically anterolateral but can cross the midline. 1 In contrast, a cystic hygroma appears as an anechoic structure with septations that is typically located on the back of the neck or can be bilobed and extend off both sides of the neck. 6 Other potential differential diagnoses of a fetal goiter include thyroglossal duct cysts, lymphangiomas/hemangiomas, branchial cleft cyst, and other developmental lesions.7,8 The use of 3D sonography can help in differentiating a fetal goiter from other lesions. Three-dimensional sonographic imaging allows multiplanar imaging to help identify the exact location of the lesion by giving a sagitial, transverse, and coronal view with one acquired volume. A rendered image of the fetal thyroid can also be acquired (Figure 5). The use of glass body rendering with 3D imaging supplemented by color Doppler allows detailed views of the goiter’s vascularity, demonstrating the degree of vascularity and whether it is peripheral vascularity or central vascularity (Figures 3 and 4).
Once the diagnosis of a fetal goiter is established, it is important to evaluate the function of the fetal thyroid via percutaneous umbilical cord blood sampling, also known as a cordocentesis. In the case presented, a PUBS procedure was used to determine the diagnosis of fetal hypothyroidism. Although prenatal treatment of fetal hypothyroidism is considered controversial, treatment of a large fetal goiter is essential because of the risk of neonatal death because of tracheal obstruction and mechanical issues at delivery caused by fetal neck hyperextension. 9 Once fetal hypothyroidism is diagnosed, it can be treated with direct administration of thyroid hormones to the fetus, with intra-amniotic administration of synthroid being the least invasive approach to fetal treatment. 10
Conclusion
A case of a fetal goiter with hypothyroidism diagnosed after a PUBS procedure is described. At 24 weeks, weekly injections of synthroid were administered with fetal thyroid levels evaluated at 31 weeks 6 days and 33 weeks 5 days. The levels of the synthroid were increased at each PUBS procedure. On the last prenatal sonography examination, the size of the fetal thyroid appeared within normal range for gestational age. At delivery, there were no complications, and an EXIT procedure was not necessary. The use of prenatal imaging allowed for the early detection of the fetal goiter and prompt treatment via amniocentesis infusions to reduce the fetal goiter and prevent adverse outcomes, which may have included neonatal death.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.