
Abstract
The detection of intraductal breast papillomas can be difficult; however, it is very important for diagnosis and treatment. Although intraductal papillomas are usually benign growths, a small percentage may be malignant. No imaging modality can distinguish between benign and malignant papillomas; that is done only with a biopsy. The symptoms vary greatly, ranging from asymptomatic to nipple discharge to a palpable mass. Multiple modalities, including mammography and ductography, have been used to identify papillomas, while magnetic resonance imaging is used to further evaluate known papillomas. Sonography has been proven crucial in identifying these masses, thereby providing information for proper treatment including ultrasound-guided biopsies. The uses of various sonographic techniques, such as color Doppler, harmonic imaging, ballottement, use of stand-off pads, echo palpation, and elastography, have improved the detection of these masses.
Intraductal breast papillomas are benign growths arising from the lining of the ducts, whereas intraductal papillary carcinomas are malignant growths within the ducts. Both lesions have similar symptoms and characteristics. Although intraductal breast papillomas account for less than 10% of benign breast lesions and invasive papillary carcinomas account for less than 2% of all breast cancers, recognizing papillomas is very important. 1 Ultrasound is used not for distinguishing between these benign or malignant masses, but for properly demonstrating the mass’s qualities. The sonographer must demonstrate the size, vascularity, ductal dilatation, and other distinguishing characteristics of the mass. This will help the radiologist with the differential diagnosis as well as recommendations for treatment.
Benign Intraductal Papillomas
There are two types of benign intraductal papillomas: solitary and multiple. Solitary papillomas are also called central papillomas, which often form in the larger ducts near the nipple. A solitary papilloma appears as a round or oval small mass within the duct. It grows in a frond-like pattern and has a central vascular stalk (Figure 1). The larger lesions dilate the duct and extend along the long axis of the duct (Figure 2). These can appear to be more oval in shape. Papillomas may be pedunculated or broad based, similar to an endometrial polyp. Most intraductal papillomas occur in perimenopausal women aged 35 to 55 years. 2 The causes and risk factors are unknown. Solitary intraductal papillomas are the most common cause of nipple discharge, which can be either clear or bloody. 3 They are most often only 2 to 3 mm in diameter; however, some can grow quite large and may be palpable (Figure 3).

Gray-scale image of a typical small papilloma (arrow) near the nipple region causing mild ductal dilation.
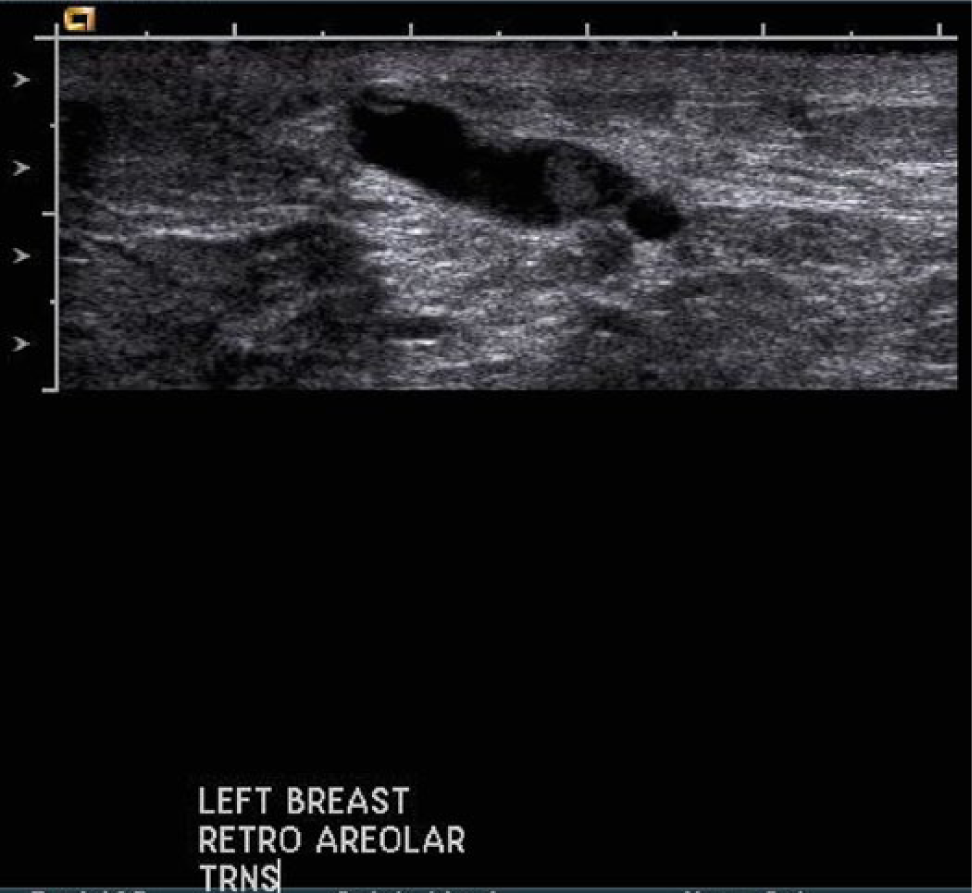
Gray-scale image of a large papilloma near the nipple region showing extension along the duct and causing significant ductal dilation.
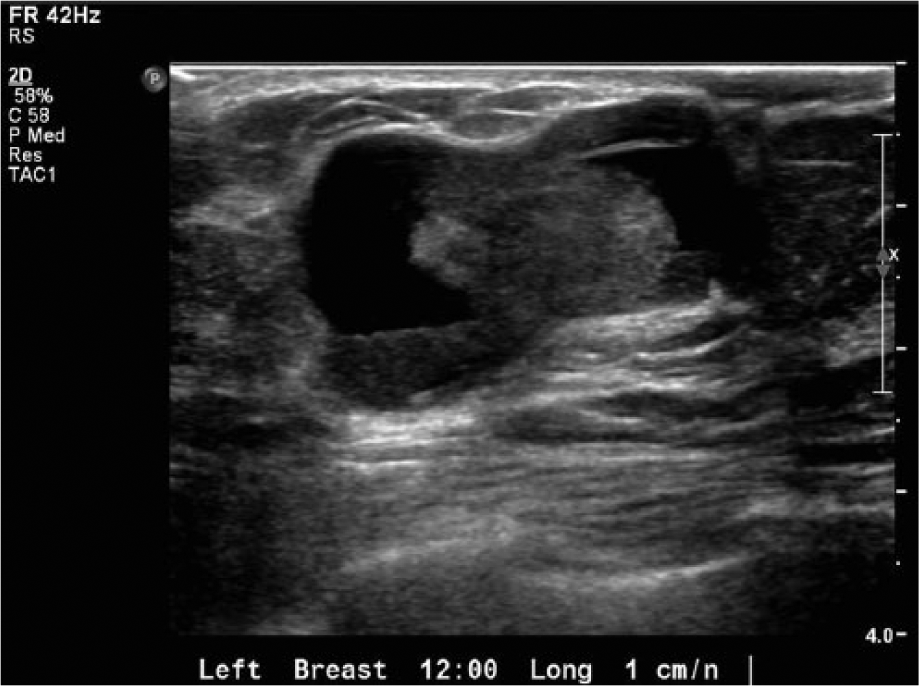
Gray-scale image of a very large, palpable papilloma with significant extension along the duct and marked ductal dilation.
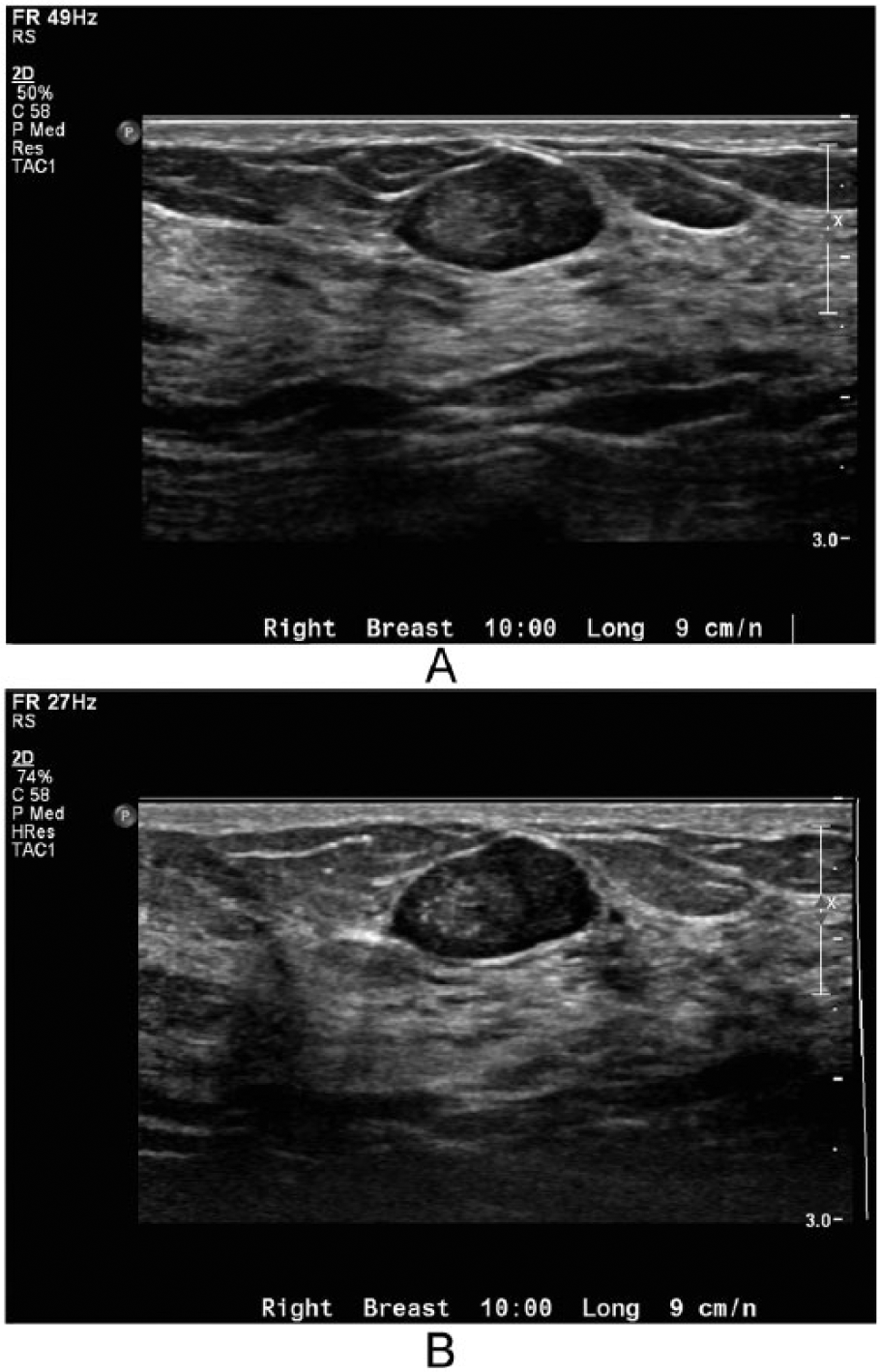
Multiple papillomas are also called peripheral papillomas and are found in the smaller ducts further from the nipple. The term peripheral does not refer to the distance from the nipple but rather the relationship to the duct. These papillomas are found on the outer portion of the duct and involve the terminal ductal lobular unit (Figures 4 and 5). Multiple papillomas are found in clusters and tend to be in younger patients. 4 They are not commonly associated with nipple discharge and usually present as a palpable mass. Multiple papillomas are less common than solitary papillomas; however, some studies show a relationship to an increased risk of breast cancer. One study cited a relationship of multiple papillomas to breast cancer as high as 10% to 30%. 1
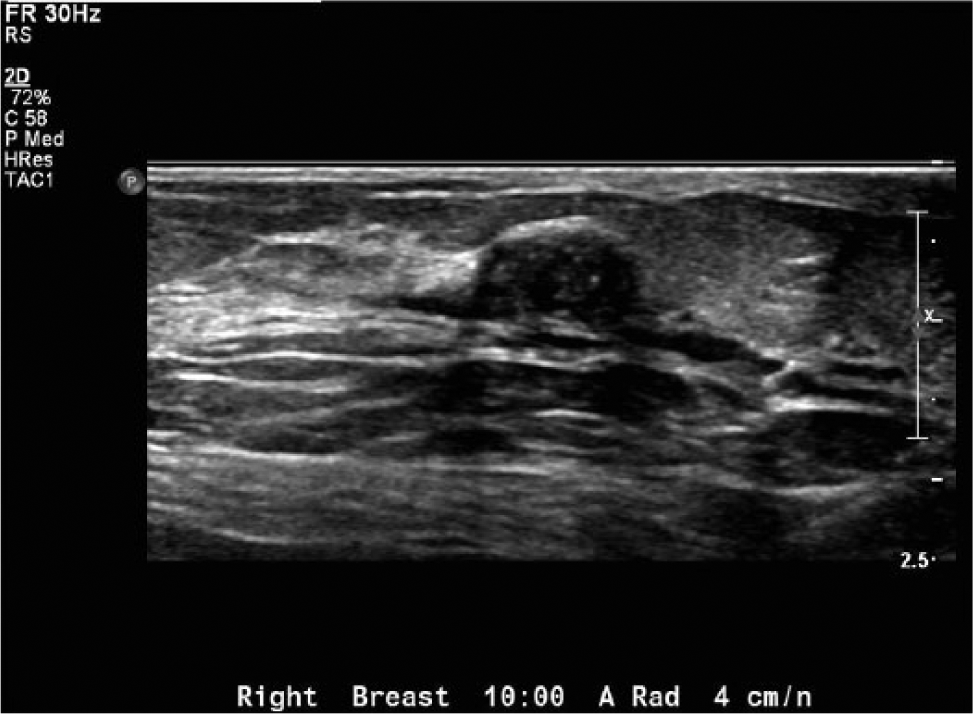
Gray-scale image of a palpable peripheral papilloma involving the terminal ductal lobular unit
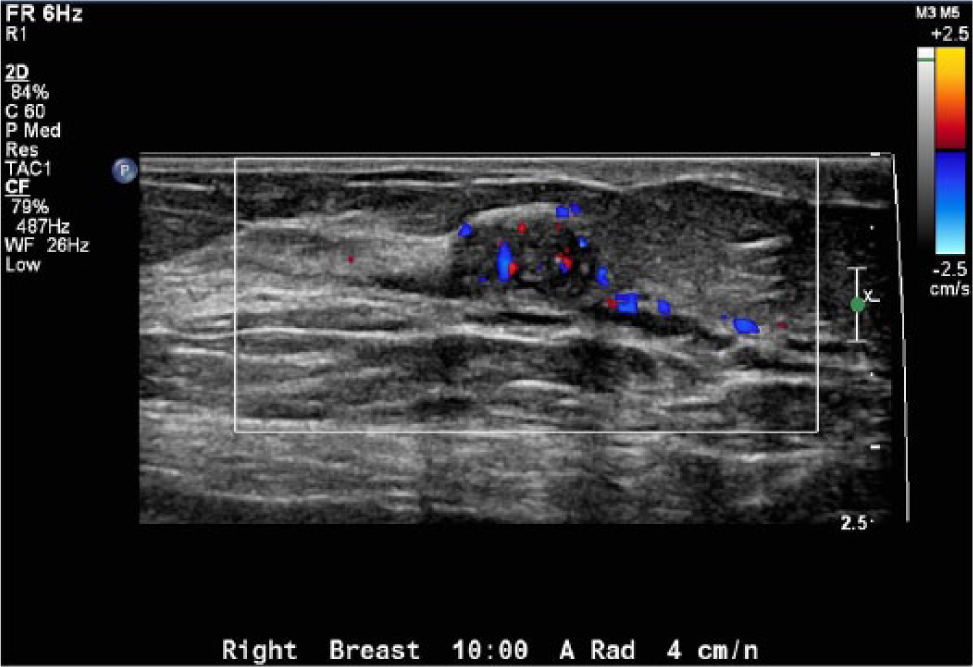
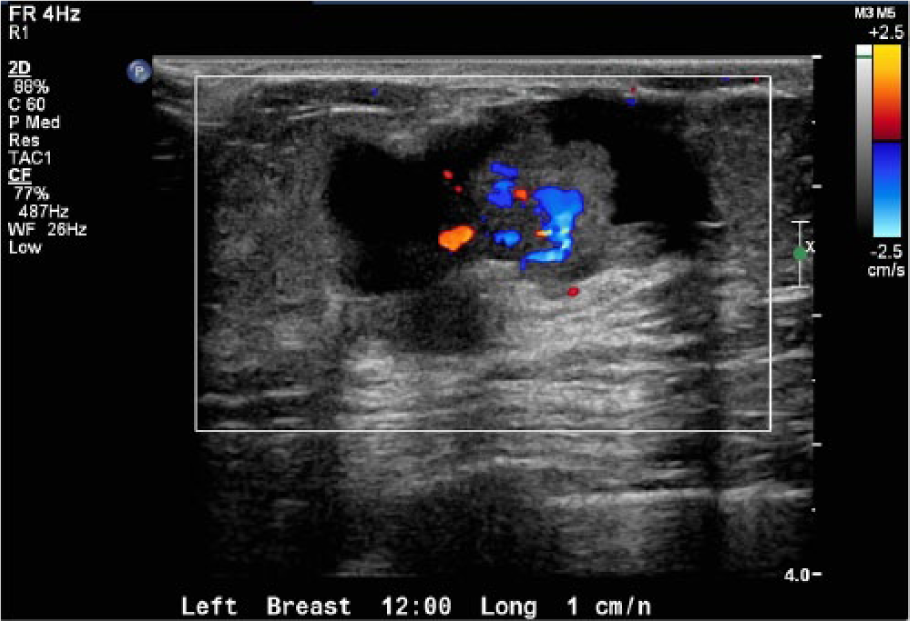
Color Doppler image of the peripheral papilloma showing the vascularity within the lesion.
Intraductal Papillary Carcinoma
Intraductal papillary carcinomas are defined as neoplastic cells growing around the internal lining of the duct space with papillary projections. Essentially, they are cancerous solitary papillomas (Figure 6). Intraductal papillary neoplasms are commonly associated with microcalcifications, which may be seen on mammography. 4 Papillary carcinoma is rare and found in only 1% to 2% of all invasive breast cancers, and bloody discharge is found in approximately 22% to 34% of patients. 2 Like benign papillomas, papillary carcinoma is highly vascular; however, the malignant lesions tend to bleed centrally. 4 During a core biopsy, proper tissue sampling of the entire lesion, not just the center, is essential for diagnosis. If a sample is taken from only the center of the mass, the cancer cells may not be present.

Clinical Symptoms and Treatment
The clinical symptoms for all papillomas, both benign and malignant, are the same. Symptoms include breast enlargement, palpable breast lump, breast pain, or nipple discharge, or the patient may be asymptomatic. 4 If the nipple discharge is bloody, it is most likely a result of the twisting of the fibrovascular pedical or stalk. 5 Clinical symptoms need to be thoroughly evaluated, so that the proper imaging is ordered.
In the early 20th century, little was known about intraductal papillomas, and some physicians performed a mastectomy as treatment. 6 Today, biopsy or surgical removal is recommended for all detected papillomas because of the similar characteristics of benign and malignant masses.6,7 The biopsy may be performed in one of two ways: excision biopsy or core/vacuum biopsy. The more invasive choice would be an excisional biopsy done in the operating room; this procedure would completely remove the mass. An excisional biopsy can be truly definitive because a pathologist can evaluate the entire mass, although this procedure is more expensive and has a greater risk to the patient, including those associated with anesthesia and increased risk of infection/seroma secondary to a larger incision. An ultrasound-guided biopsy, either vacuum-assisted or core needle, typically uses a 9- to 14-gauge needle to obtain adequate and accurate tissue samples. The larger-gauge needle is recommended to reduce sampling error because the most aggressive elements of the cancer are located peripherally and not in the center of the lesion. Studies have shown that the vacuum-assisted biopsy devices obtained a better sample for evaluation when compared with the core needle biopsy devices.7–9 A core biopsy device is usually 12 to 14 gauge, whereas a vacuum-assisted device may be only 9 to 12 gauge. An ultrasound-guided core biopsy is less invasive and poses less risk to the patient than an open surgical procedure. 7 Ultrasound-guided biopsies are generally preferred as opposed to mammography (stereotactic) or magnetic resonance image (MRI)–guided biopsy because of the real-time imaging. This procedure is also less time-consuming, and compared with biopsies using other modalities, it is more comfortable. The biopsy device is imaged for placement of the needle and is imaged throughout the procedure, including the placement of a surgical clip if necessary. In both stereotactic and MRI-guided biopsies, the patient is in a prone position, which may be impossible for many patients.
After an ultrasound-guided core or vacuum-assisted biopsy is performed, the papillary lesions can be designated into three categories: benign, malignant, or atypical. 6 This diagnosis can be challenging for the pathologist since there are no universally accepted criteria for distinguishing between atypical papilloma and malignant papilloma. 10 Malignant and atypical lesions are treated the same, and the consensus is that all of the lesions should be excised. However, there is still some debate about the need for excision of biopsy-proven benign papillomas.6,11
Diagnostic Imaging
Mammography, ductography, MRI, and sonography can all be used in the detection and diagnosis of breast papillomas.4–6,9–12 Mammography should be performed first if the patient presents with nipple discharge or a palpable lump. Most small papillomas are not detected on conventional mammography (Figure 7); however, mammography can detect dilated ducts, which are an indicator of an intraductal papilloma. Mammography can detect larger papillomas, which are seen as a mass (Figure 8). Also, mammography can detect microcalcifications, which can be an indicator of an intraductal papillary neoplasm. Some intraductal papillary neoplasms present as architectural distortion, which would further indicate a need for sonography. Mammography alone has a sensitivity/specificity rate of approximately 78%, but combined with targeted ultrasound, it increases to approximately 91%. 13
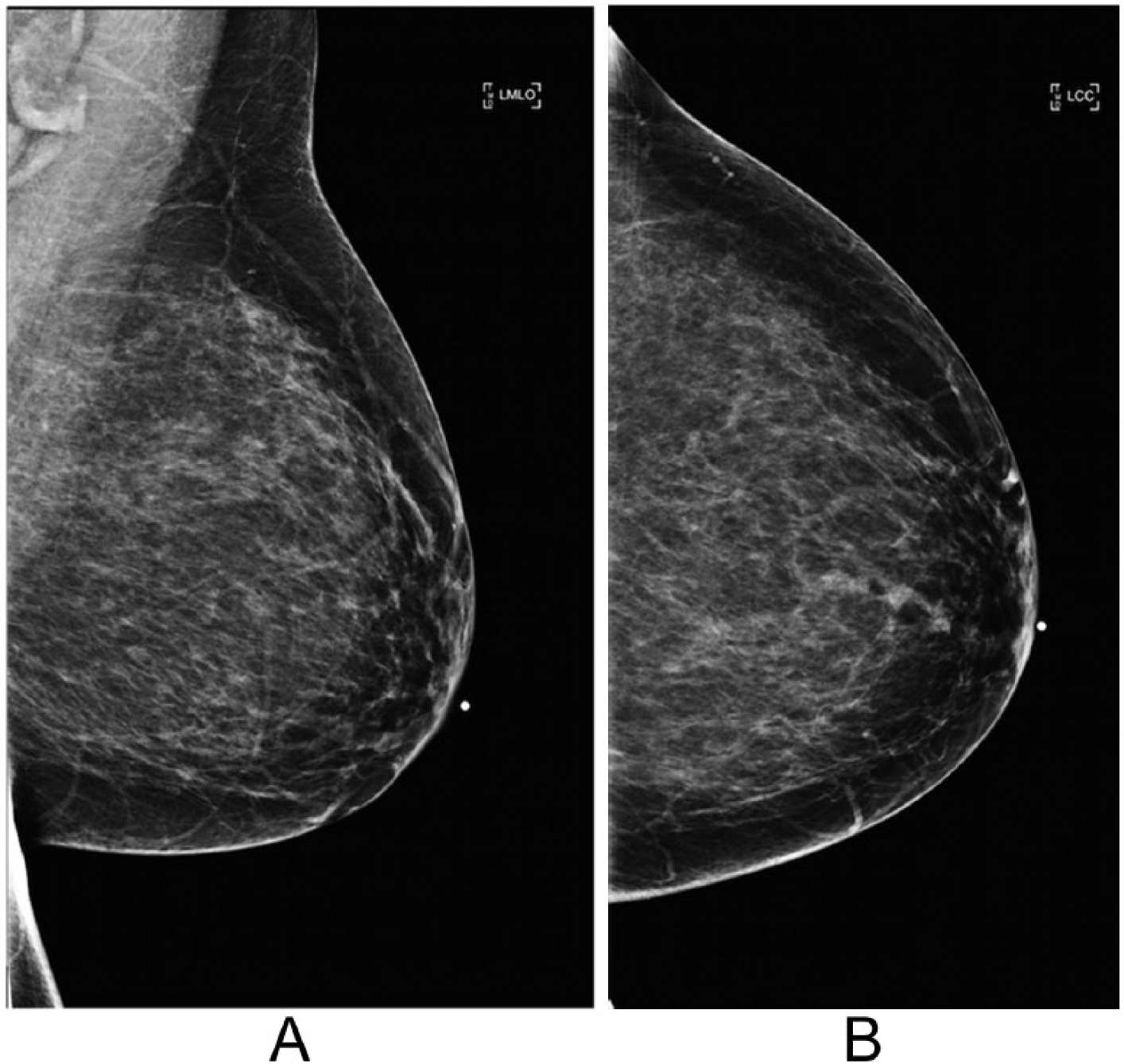
Mammogram of a patient with a biopsy-proven papilloma. Note that the lesion was not seen in either the mediolateral oblique view (A) or the craniocaudal view (B).
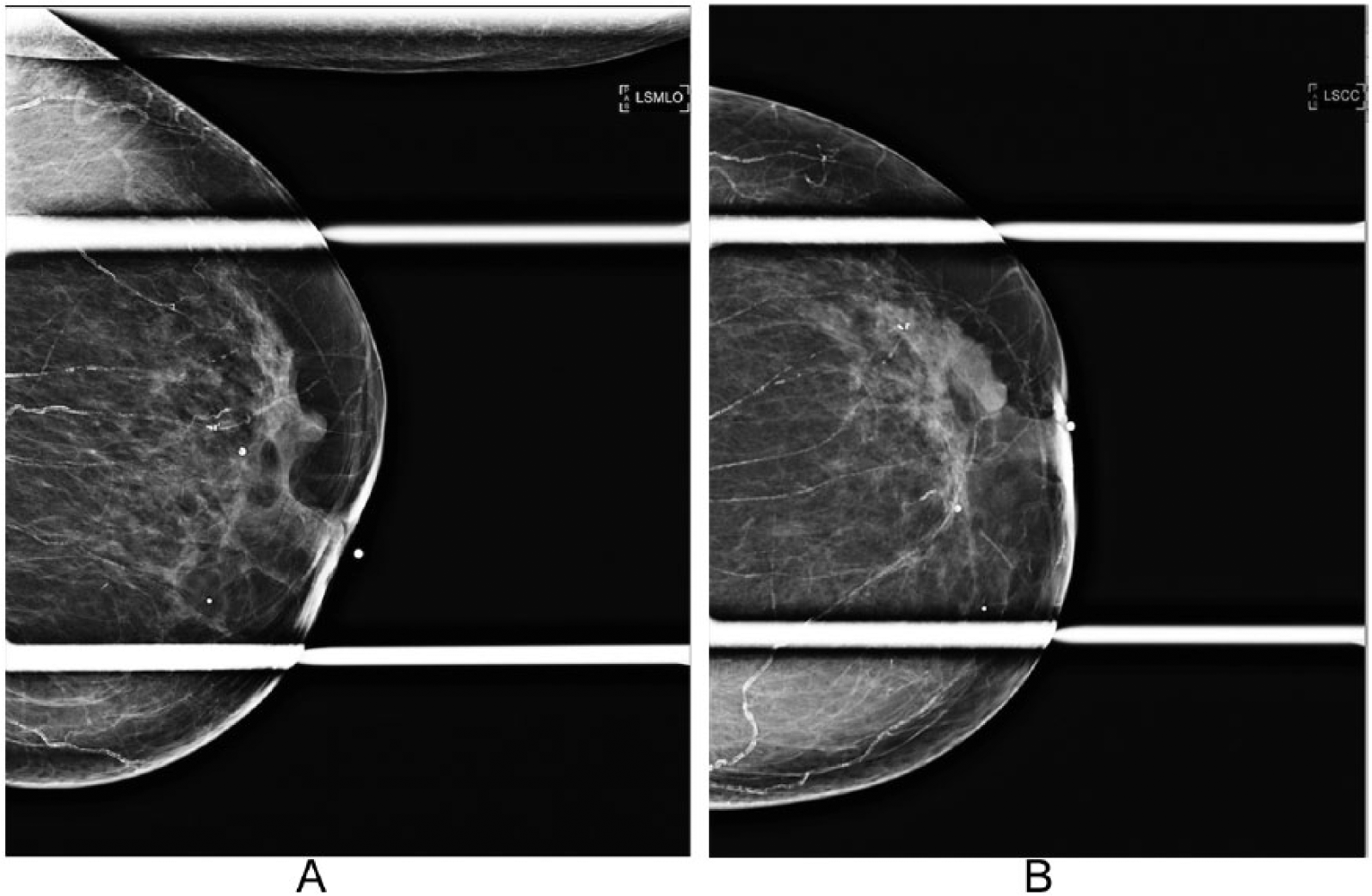
Magnification mammogram of a patient with a large biopsy-proven papilloma causing ductal dilation. In this patient, the lesion can be identified in both the mediolateral oblique view (A) and the craniocaudal view (B).
Ductography, also known as galactography, can also be helpful in detecting papillomas, but it has many limitations. 5 Ductography is a radiographic procedure that requires a contrast agent to be injected into the breast (Figure 9). This procedure can be performed only if a discharge can be elicited from the breast. When the discharge has been elicited, a cannula is placed directly into the duct via the nipple. After the contrast has been injected, a mammogram is performed. A papilloma is visualized as a filling defect within a dilated duct, although nonobstructing lesions will not be identified, increasing the false-negative results. It is also a fairly painful procedure.
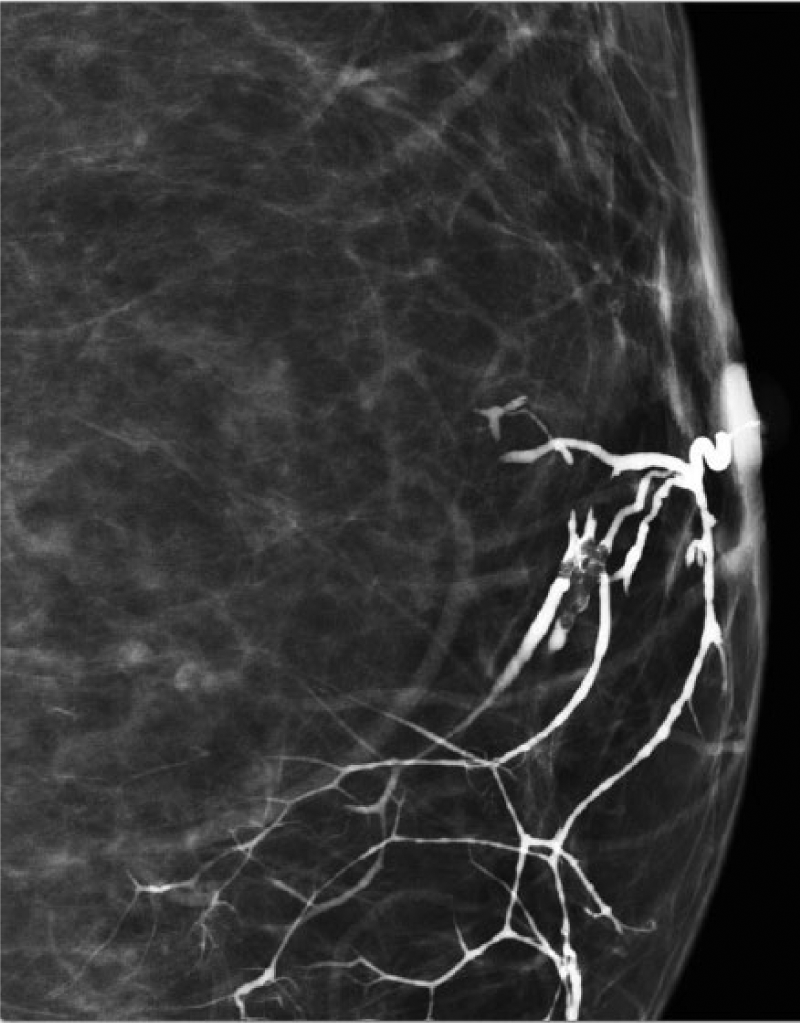
Galactogram (or ductogram) showing a filling defect in the duct. An ultrasound-guided biopsy provided the tissue diagnosis of benign intraductal papilloma.
Breast MRI use has grown substantially over the past few years as an adjunct to mammography and sonography 9 (Figure 10). MRI is not used for the detection of papillomas because they can have a variable appearance on MRI, which significantly reduces lesion specificity. Studies do show high specificity, up to 98%, for invasive carcinomas but not specifically for papillomas. 9 MRI can note dilated ducts, and if T1- and T2-weighted series demonstrate hyperintensity, it can be assumed that the hyperintensity is due to a small hemorrhage, which is common in the center of papillary lesions.12,13 In some smaller studies, almost all biopsy-proven papillomas have the characteristics of a well-circumscribed mass with homogenous early enhancement, while other studies show no difference between enhancing papillomas and nonenhancing papillomas.4,9,12,13 There are no definitive predictive MRI characteristics that have been proven for papillomas.
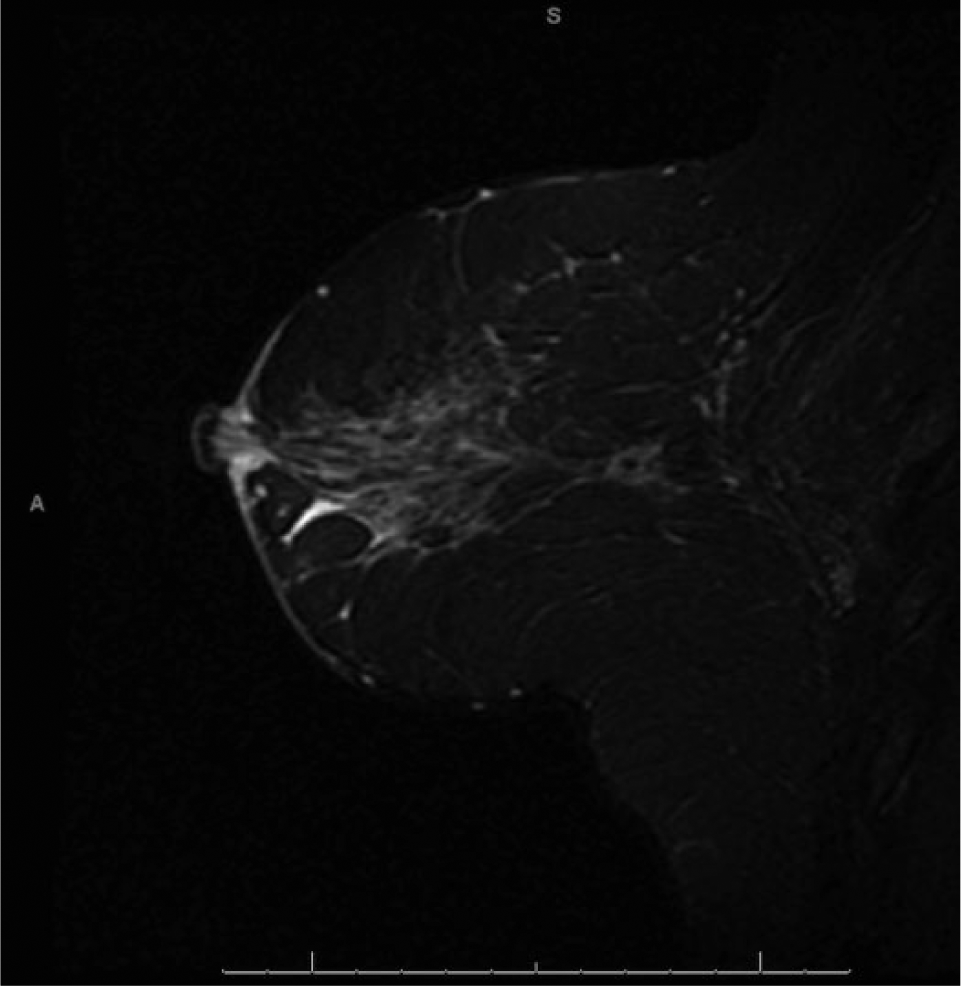
Magnetic resonance image of a normal breast showing the typical ductal pattern.
Sonography is the imaging of choice for identifying intraductal papillomas following mammography.4,5 Using as high a frequency probe as possible, ideally in the 12- to 17-MHz range, high-resolution sonography can detect papillomas quite readily. Sonography has been noted to have an approximate 85% to 90% sensitivity and specificity for the detection of papillomas.14,15 When a dilated duct is detected, the length of the duct is followed noting any intraductal mass or debris. Papillomas can have a varying appearance on sonography, ranging from homogeneously hypoechoic to complex and from normal sound transmission to posterior acoustic shadowing. 5 Like the other modalities, there are no specific criteria for distinguishing a benign papilloma from an atypical or malignant papilloma. No sonographic features were sensitive or specific enough to allow for differentiation between benign and malignant papillomas.15,16 Some studies have surmised that there is an increased risk of malignancy if the papilloma is not oriented parallel to the duct or demonstrates posterior acoustic enhancement, but these were somewhat smaller studies and have not been conclusive.1,15,16 The use of harmonic imaging also can help define the characteristics of the mass 17 (Figure 11). Harmonic imaging has been shown to improve visualization of a lesion’s borders and acoustic shadowing, although this has not been entirely consistent with papillomas. Papillomas are usually oval in shape but can have a varied appearance. Color Doppler imaging is helpful in documenting blood flow to the area of interest, but the degree of vascularity is not a predictor of malignancy1,12 (Figure 12). Both benign and malignant papillomas tend to be soft and compressible, and excessive compression by the sonographer may obstruct the blood flow within the lesion, producing a false impression of absent blood flow. 5
Comparative gray-scale images of a peripheral papilloma (A) without and (B) with tissue harmonic imaging. Without harmonic imaging, there is significant through transmission enhancement deep to the lesion, and the tissues in that region are not as clearly resolved. With harmonic imaging, there is less through transmission artifact, the tissue within and deep to the lesion is seen more clearly, and the edges of the lesion are better defined.
Color Doppler image of the large, palpable papilloma seen in Figure 3 showing significant vascularity within the lesion; a finding such as this is not definitive in discriminating benign from malignant lesions.
For patients with nipple discharge, imaging begins at the nipple in a radial projection. When imaging patients with a palpable lump or a focused area of pain, imaging should begin at the directed area. It is important to ask the patient to palpate the area and scan in varying positions. Securing the area with the nonscanning hand (echo palpation) may be helpful. The sonographer must be mindful to look not only for ductal dilatation but also for multiple (peripheral) papillomas, which typically do not present with any ductal dilatation. In some patients, it may be difficult to determine the contents of a dilated duct. Using compression, also known as ballottement, can help to differentiate between inspissated (thickened and viscous) secretions and a papilloma. Inspissated secretions will disperse upon compression, while a true papilloma will retain its shape 2 (Figure 13). Internal vascularity identified by color Doppler imaging indicates a true papilloma versus inspissation (Figure 14). Many patients will have ductal ectasia, or simple dilatation of the duct, but the entire duct must be imaged to exclude a mass. In some cases, a standoff pad may be helpful in imaging super-ficial ducts.2,5 Imaging papillomas in orthogonal views (90°) is essential for size and location within the duct.

Gray-scale image of a dilated duct with internal echogenicity, which may represent either the thickened, viscous debris of inspissation or multiple small papillomas.
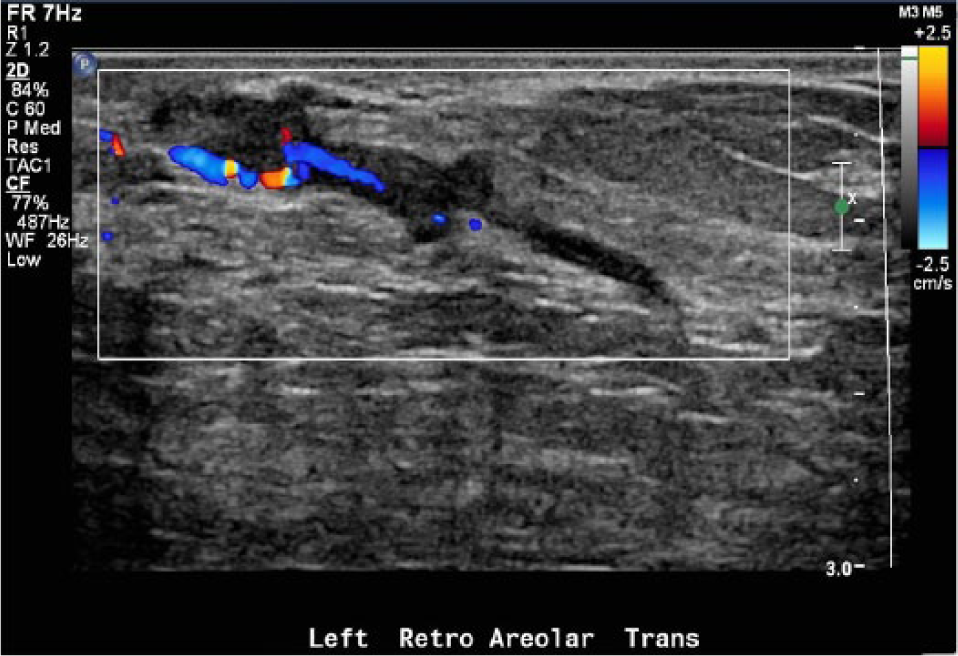
Color Doppler image of the dilated duct seen in Figure 13 using probe compression (ballottement); the gray-scale component of the image indicates the duct and echoes do not appear changed and the vascularity within the intraductal echoes indicate a diagnosis of papilloma.
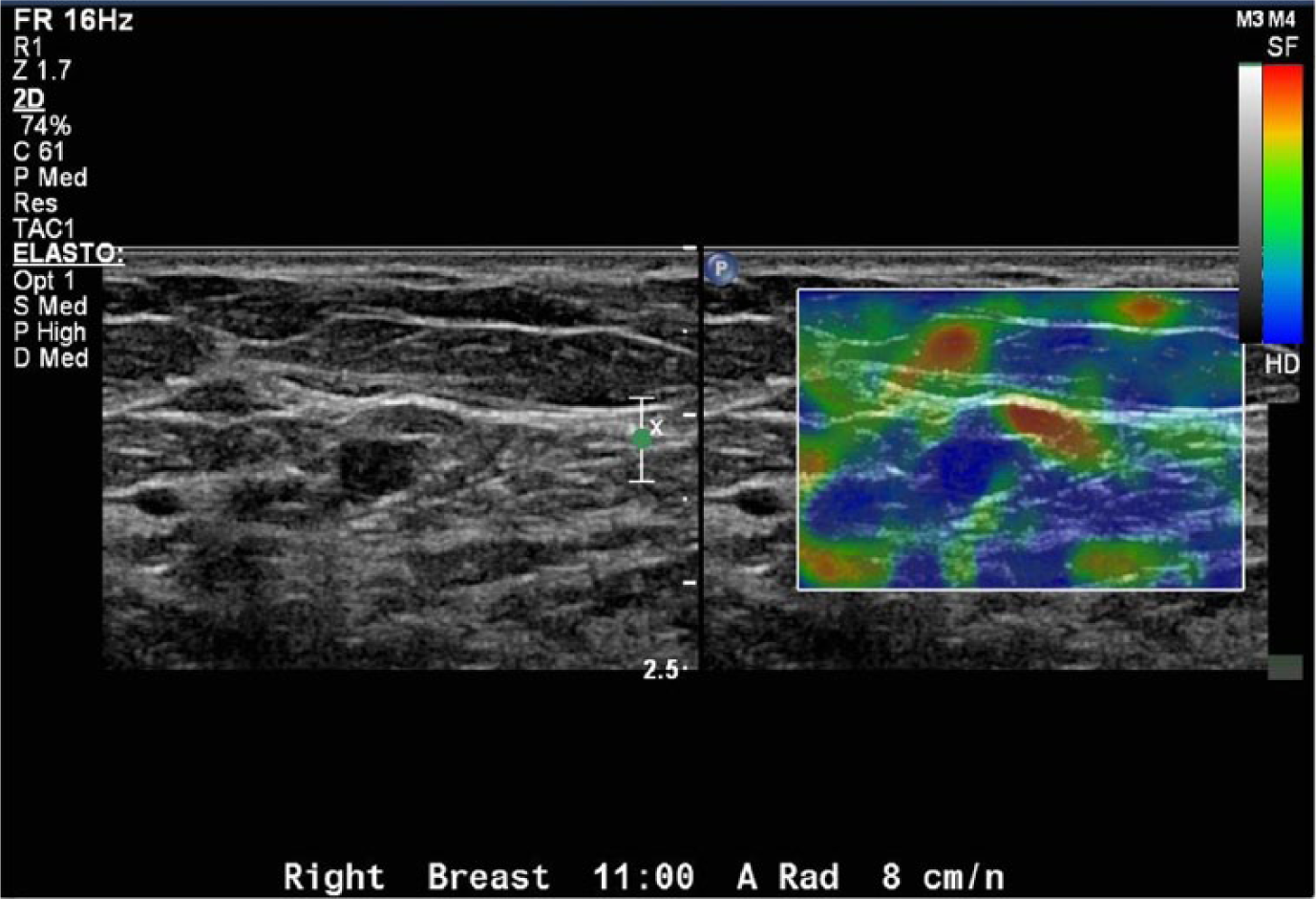
There have been recent studies evaluating the effectiveness of elastography as a determinant of the hardness or stiffness of a lesion for detection of papillomas18–21 (Figures 15 and 16). Compression elastography, also called strain elastography, is done by the sonographer using free hand tissue compression while imaging the mass. This form of elastography is highly dependent on technique and the degree of compression of the surrounding tissue and therefore can be inconsistent.18,19 Shear-wave elastography will show the stiffness of the mass as compared with the surrounding tissue using a color map; it has the significant advantage that no external compression is necessary, making the technique less operator dependent and more reproducible.20,21 Typically, benign masses have a soft appearance and also have a solid or mixed appearance indicated by the color map, while suspicious masses have a hard appearance as indicated by the color map. 21 The research on elastography for solid masses has been extensive; however, the studies on breast papillomas are still in their infancy and have not been conclusive.20,21
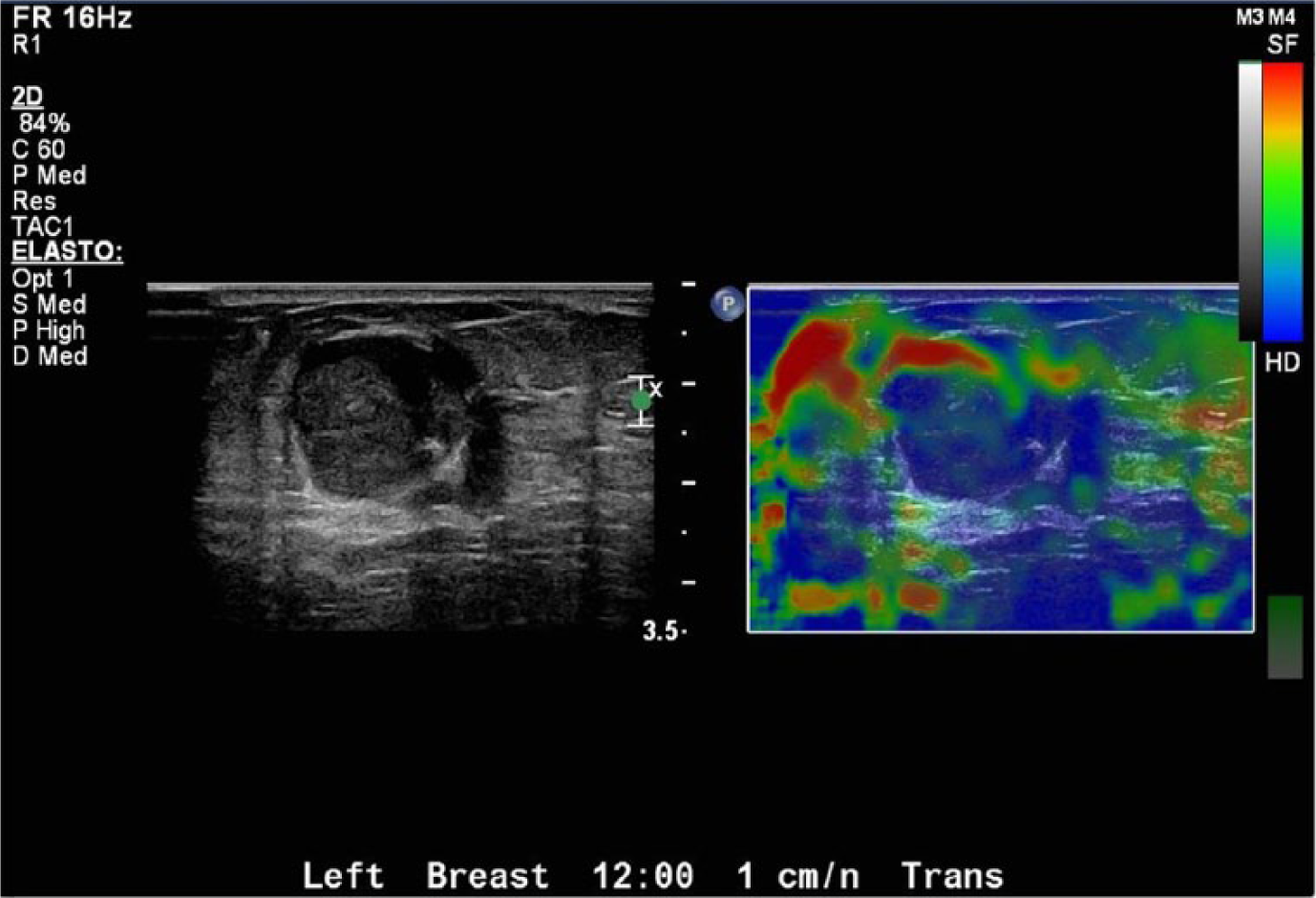
Elastography of a large breast papilloma showing a mix of both soft (red) and hard (blue) tissue characteristics within the lesion.
Elastography of a small breast lesion showing predominantly hard (blue) tissue characteristics, suspicious for (but not at this time conclusive evidence of) papillary carcinoma.
Conclusion
Intraductal breast papillomas, both solitary and multiple, are important to identify properly. Although there are multiple modalities that are able to image the breast, sonography has been shown to be the most effective in identifying these masses. Ultrasonographic imaging can distinguish the size, position, vascularity, and degree of ductal dilatation associated with breast papillomas. The sonographer must combine the clinical symptoms with any mammographic findings to correctly identify the area of interest. Use of all resources such as stand-off pads, color Doppler imaging, tissue harmonic imaging, ballottement, and echo palpation is necessary to localize and clearly demonstrate breast papillomas. Shear-wave elastography also shows early promise for lesion detection and classification. These findings will help the radiologist or breast surgeon form a diagnosis and recommendation for treatment. When a biopsy is indicated, an ultrasound-guided core biopsy is the least invasive choice for the patient, and the real-time guidance ensures proper sampling. Although papillomas are included in multiple research studies of solid breast masses, there are very few studies dedicated solely to characterizing intraductal breast papillomas, and it is hoped that more research will lead to better treatment of papillomas.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.