
Abstract
Twin-to-twin transfusion syndrome (TTTS) is a known complication of 10% to 15% of monochorionic/diamniotic twin gestations. It is also known that the “recipient” twin in these pregnancies is at higher risk for cardiac abnormalities. Early identification of TTTS and recognition of changes in fetal cardiac function can reduce fetal morbidity and mortality. This case describes intrauterine myocardial infarction developing in the recipient twin of a monochorionic/diamniotic twin gestation complicated by TTTS.
Keywords
Monochorionic twin gestations are complicated by twin-to-twin transfusion syndrome (TTTS) in approximately 10% to 15% of cases. Perinatal mortality of either fetus can be as high as 70% to 80% if left untreated.1,2 TTTS evolves when an anastomosis occurs between communicating vessels at the level of the placenta, resulting in a disproportionate shift of blood volume from one twin to another, for which the fetuses cannot compensate. Consequently, the volume-depleted “donor” twin develops oliguria and oligohydramnios. The volume-overloaded “recipient” twin develops polyuria, resulting in polyhydramnios.
The Quintero staging system can be used to assess the severity of TTTS based on the following sonographic findings: amniotic fluid volume, fetal bladder size, Doppler interrogation of the umbilical arteries and ductus venosus, and the presence of hydrops (Table 1). 3 In addition, changes in cardiac structure and function not assessed in Quintero staging occur in the recipient twin early in the evolution of TTTS, as described by the Cincinnati modification of the Quintero staging system (Table 2). 4 Ventricular systolic dysfunction, cardiac chamber enlargement, ventricular hypertrophy, and atrioventricular valve regurgitation have been demonstrated in the recipient twin of affected pregnancies. 5
Quintero Staging System for Twin-Twin Transfusion Syndrome
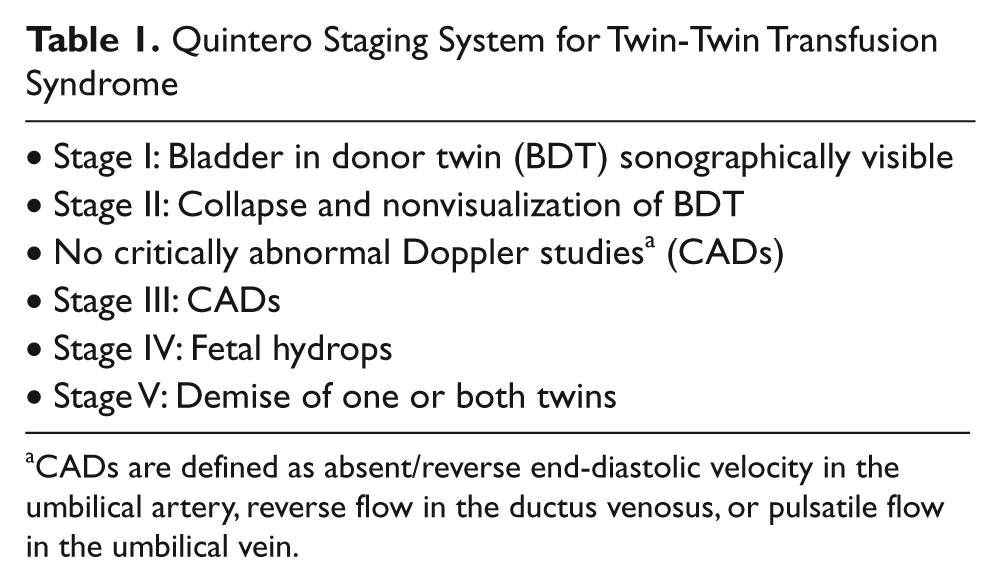
CADs are defined as absent/reverse end-diastolic velocity in the umbilical artery, reverse flow in the ductus venosus, or pulsatile flow in the umbilical vein.
Cincinnati Modification of the Quintero Staging System for Twin-Twin Transfusion Syndrome
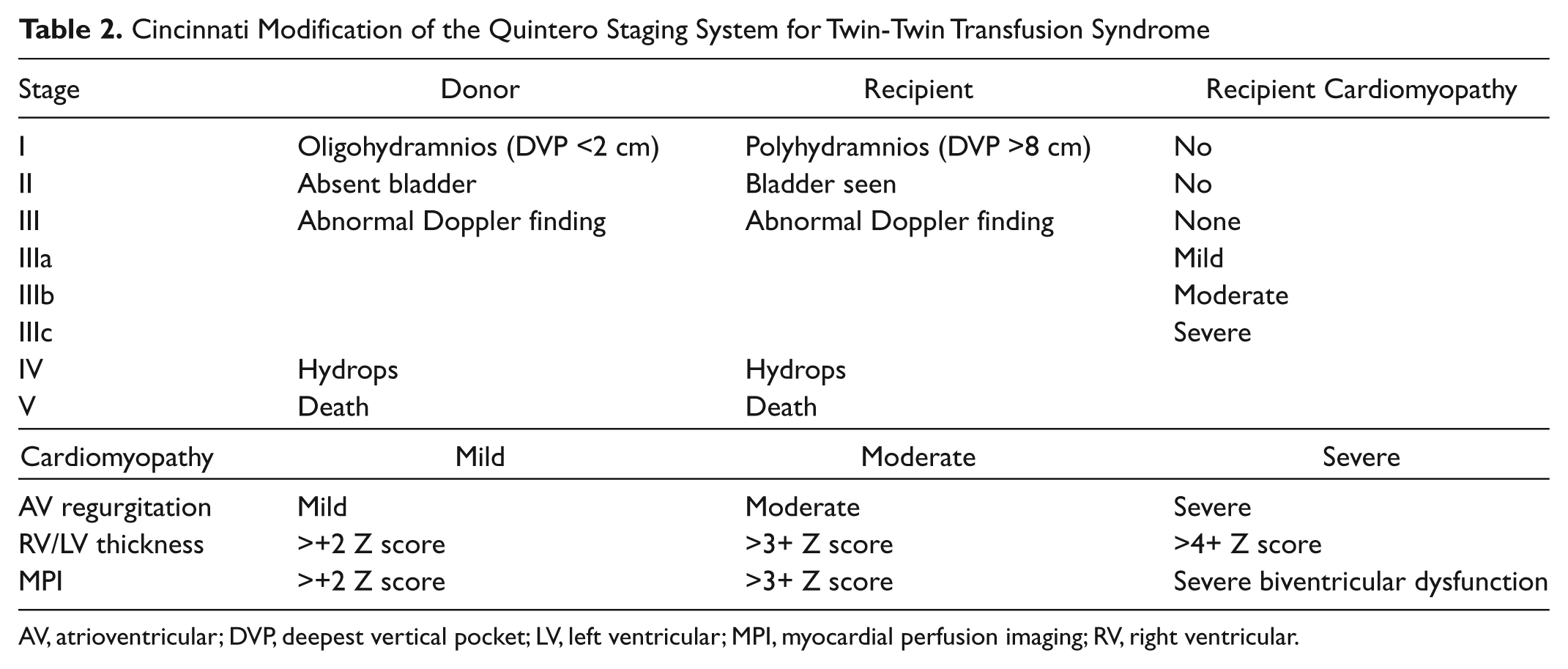
AV, atrioventricular; DVP, deepest vertical pocket; LV, left ventricular; MPI, myocardial perfusion imaging; RV, right ventricular.
Over the past 10 years, the treatment of severe TTTS has shifted from repetitive amnioreduction to selective laser photocoagulation of communicating vessels (SLPCV). SLPCV has been shown to improve the course and outcome of severe TTTS (Quintero stage II or above) in previable fetuses between 16 and 26 weeks’ gestation. 6
Case Report
A G5/P3/A1 patient in her late 20s was referred for fetal echocardiography secondary to a diagnosis of monochorionic/diamniotic twin gestation and TTTS. Her medical history was noncontributory. Sonographic examination demonstrated TTTS, stage IV atypical recipient (hydropic recipient twin with visible donor bladder). Twin A (recipient) demonstrated polyhydramnios, hydrops, and poor cardiac contractility, with primarily left ventricular (LV) dysfunction. Twin A demonstrated an abnormal Doppler pattern with reversal of flow in the ductus venosus, an elevated Tei Index (a Doppler-derived measure of myocardial performance), and a pulsatile umbilical vein. All of these features were highly suggestive of cardiac compromise. Twin B (donor) demonstrated oligohydramnios, normal fetal Doppler patterns, and good cardiac contractility. The patient was subsequently referred for SLPCV and therapeutic amnioreduction at 20 weeks’ gestation.
A preoperative sonogram was performed prior to the laser procedure and demonstrated stage IV atypical recipient TTTS, with similar sonographic findings outlined above. Three weeks following SLPCV, there had been adequate interval fetal growth in both twins; however, the estimated fetal weights remained discordant. Twin A had a normal amount of amniotic fluid. The previously imaged ascites and skin edema had resolved, and there was a mild apical pericardial effusion. However, the severe LV dysfunction remained.
At 30 weeks’ gestation, a complete fetal echocardiograph examination was performed in our department using a Toshiba istyle Aplio MX (Toshiba Medical Systems Europe, Zoetermeer, the Netherlands) with a 3.5-MHz curvilinear probe. The fetal echocardiogram on twin A demonstrated mildly decreased right ventricular (RV) systolic function, severe LV dysfunction with endocardial fibroelastosis involving the septum and posterior wall, mild LV enlargement, and a mildly hypoplastic aortic arch with retrograde flow (Figure 1, Video Clip 1). The ductus venosus Doppler pattern demonstrated prominent a-wave reversal, an indicator of cardiovascular deterioration (Figure 2). Given the patient’s history, the twins were monitored weekly with serial sonograms, biophysical profiles, and umbilical artery Doppler surveillance until delivery.

(Video Clip 1) Four-chamber view of the fetal heart demonstrating left ventricular enlargement, endocardial fibroelastosis, and pericardial effusion (PE). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.
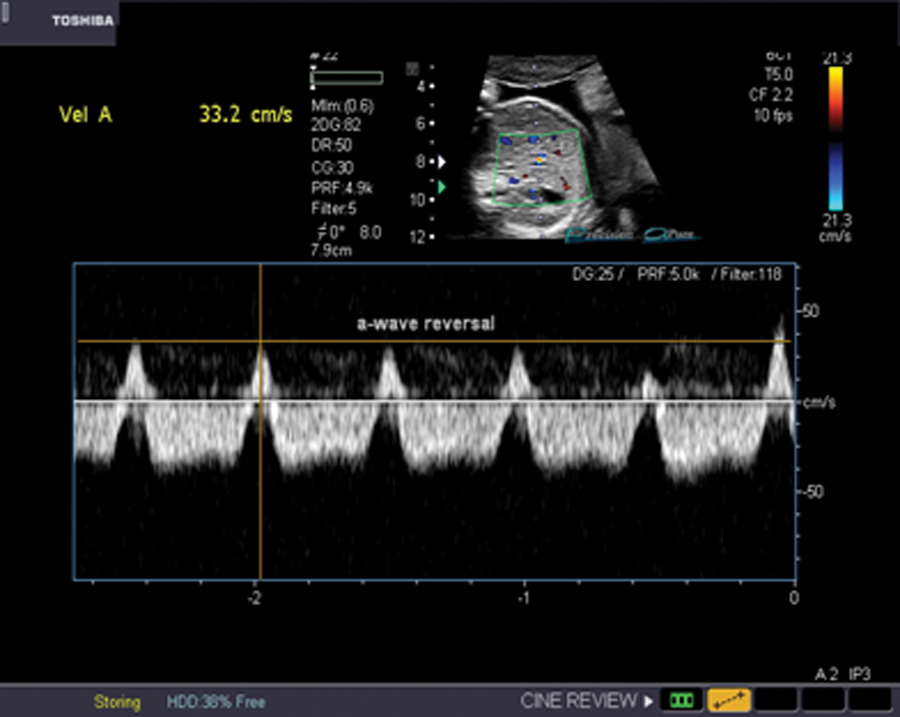
Abnormal Doppler pattern (a-wave reversal) of the ductus venosus indicating evolving fetal heart failure at 30 weeks’ gestation.
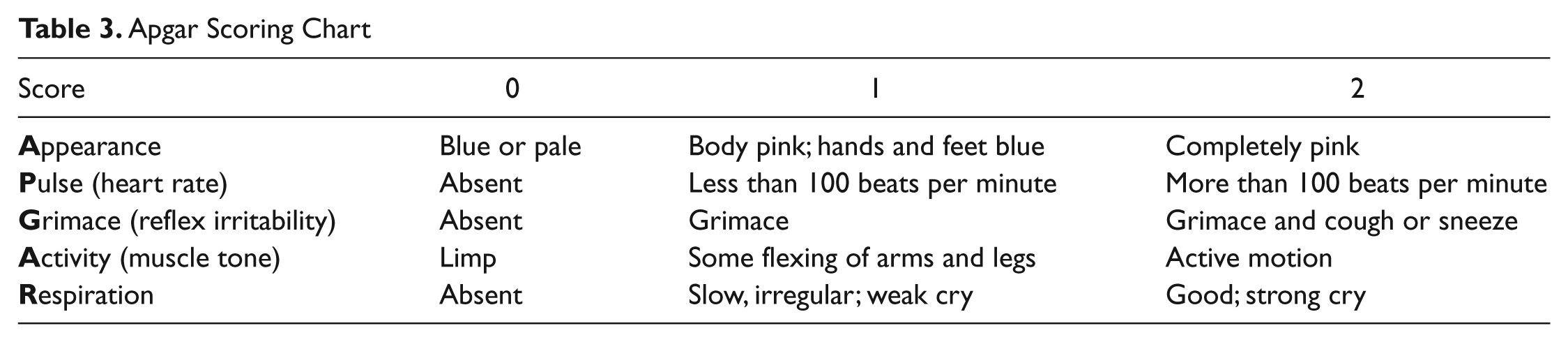
The twins were delivered by cesarean section at 36 weeks’ gestation. Twin B, the donor twin, had Apgar scores (Table 3) of 8 at one minute and 9 at five minutes and weighed 2.9 kg. Following a normal cardiac examination, the baby was discharged home with mother at four days of age. Twin A, the recipient twin, had Apgar scores of 8 at one minute and 9 at five minutes and weighed 1.87 kg. An echocardiogram demonstrated severely decreased LV function with endocardial fibroelastosis, mildly hypoplastic aortic arch without coarctation, mildly decreased RV function, a small atrial septal defect with left-to-right shunting, and a large patent ductus arteriosus with bidirectional shunting. Prostaglandin therapy (PGE1 analogs) was initiated to maintain patency of the ductus; however, the PGE was discontinued after an echocardiogram confirmed there was no evidence of ductal-dependent circulation. Umbilical venous and umbilical arterial lines were placed, and transfer to the local children’s hospital for further management was arranged.
Apgar Scoring Chart
Twin A was admitted to the cardiac intensive care unit at the local children’s hospital. Given her history of heart failure (low cardiac output syndrome), she was started on a milrinone infusion. Transthoracic echocardiography performed on admission confirmed all of the above findings. Transcranial sonogram was normal.
Over the course of the hospitalization, twin A demonstrated persistent severe LV dysfunction with mild LV dilation and moderate left atrial dilation (Figure 3, Video Clip 2). She was maintained on milrinone and carvedilol, a beta-blocker. Single-ventricle palliation and orthotopic heart transplantation were discussed. However, during cardiac catheterization for persistent tachypnea and worsening RV function, the baby was noted to have increased pulmonary vascular resistance (PVR) for which sildenafil was initiated. Cardiac transplantation was withheld until the PVR decreased. At one month of age, twin A continues to demonstrate severe LV dysfunction and has a guarded clinical course, which may eventually require cardiac transplantation.
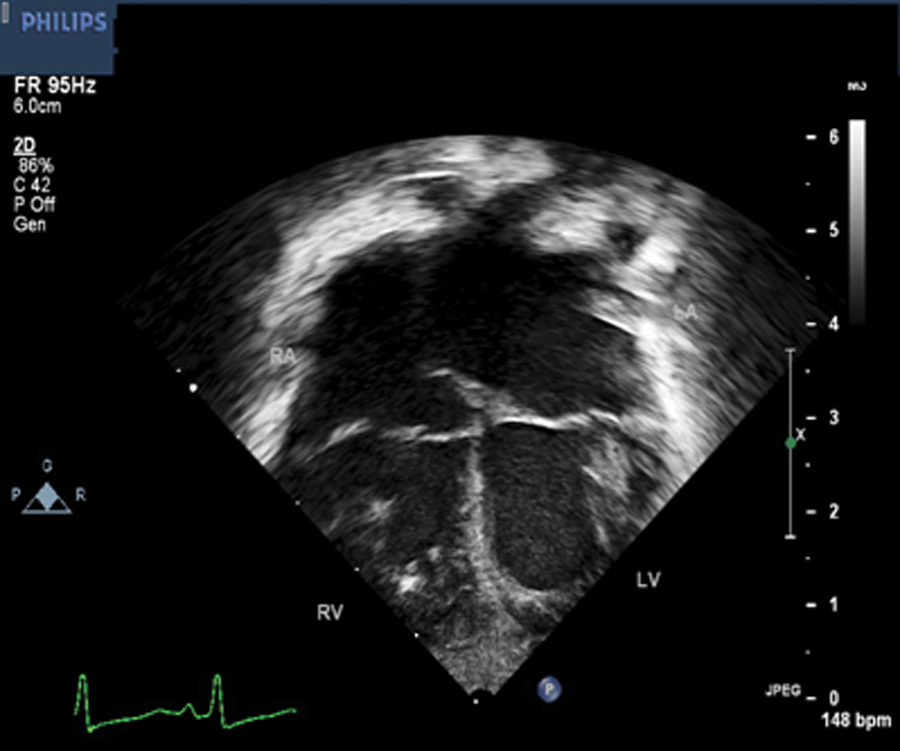
(Video Clip 2) Apical four-chamber view at four weeks of age. Note the presence of left ventricular endocardial fibroelastosis. LV, left ventricle; RV, right ventricle.
Discussion
TTTS is a known complication affecting 10% to 15% of monochorionic/diamniotic twin gestations. If left untreated, it carries a 70% to 80% risk of perinatal mortality.1,2 Treatment for severe TTTS has shifted from repetitive amnioreduction to SLPCV over the past 10 years, improving the course and outcome of the syndrome. 6
The Quintero staging system can be helpful in determining the presence and degree of TTTS (Table 1). 3 During sonographic examinations, a skilled sonographer should assess amniotic fluid volumes, bladder sizes, and for the presence of hydrops. Umbilical vessel and ductus venosus waveforms should be obtained and assessed for absence or reversal of flow. Close observation is required for signs of ventricular dysfunction with or without evidence of endocardial fibroelastosis, as progressive ventricular dysfunction can lead to dilation of the involved chamber.
In 2007, Michelfelder et al 5 described that ventricular hypertrophy, RV and/or LV dysfunction, and atrioventricular (AV) valve regurgitation were prevalent in recipient twins at all Quintero stages. Cardiomegaly and severe systolic RV and/or LV systolic dysfunction appeared with increasing frequency in higher Quintero stages.
This case study demonstrates the appearance, treatment, and outcome of the recipient twin in a monochorionic/diamniotic twin gestation complicated by twin-to-twin transfusion syndrome and likely intrauterine myocardial infarction. A search of the literature yielded one similar case; however, the pregnancy was terminated. 7
We hypothesize that twin A suffered intrauterine myocardial infarction and subsequent severe LV dysfunction with evolving ventricular remodeling, including endocardial fibroelastosis and ventricular dilation, as a result of TTTS. Both global and segmental LV wall motion abnormalities could be identified during fetal echocardiography.
Conclusion
The recipient twin (twin A) of this monochorionic/diamniotic twin gestation affected by TTTS was found to have early signs of myocardial infarction. The progressive, severe LV dysfunction led to diffuse thickening of the ventricular endocardium, endocardial fibroelastosis, and eventual dilation of the chamber.
Noninvasive, detailed sonographic examinations have proven to be excellent tools when performed by skilled sonographers. The sonographers’ awareness of the signs and symptoms of intrauterine conditions and subtle changes exhibited by fetuses can facilitate early diagnosis, intervention, and treatment, thereby reducing the morbidity and mortality of some fetuses.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.