
Abstract
Ovarian torsion is the complete or partial rotation of the ovary upon its vascular pedicle with subsequent vascular compromise; it is one of a few gynecologic surgical emergencies requiring prompt diagnosis and treatment. The commonly accepted diagnostic sonographic finding in ovarian torsion is the absence of ovarian parenchymal blood flow using color or power Doppler imaging. However, since not all cases of ovarian torsion cause complete vascular obstruction, the presence of ovarian blood flow cannot eliminate this diagnosis in symptomatic patients with other positive sonographic findings. The case presented demonstrates the potential for a missed diagnosis of ovarian torsion when relying predominantly on Doppler findings.
Ovarian torsion is the complete or partial rotation of the ovary upon its vascular pedicle with subsequent arterial inflow, venous outflow, and lymphatic obstruction. When complete disruption of arterial flow occurs, acute pain and the potential for organ loss create a gynecologic emergency that requires rapid intervention to prevent ischemic ovarian necrosis and death. The commonly accepted pathognomonic sonographic finding in ovarian torsion is complete absence of ovarian parenchymal blood flow using color, power, and/or spectral Doppler evaluation. However, since not all cases of ovarian torsion result in the complete disruption of perfusion and since collateralized flow via terminal uterine artery branches may maintain ovarian viability, the presence of flow within an ovary cannot eliminate a differential diagnosis of ovarian torsion in a patient with suggestive symptoms and other positive B-mode sonographic findings. The case reported here demonstrates this potential pitfall in relying predominantly on Doppler findings to diagnose ovarian torsion.
Case Report
A 23-year-old gravida 0, para 0 patient presented to the emergency department with acute right lower quadrant pain. A pregnancy test was performed, and the result was negative. Medical history included an episode of nephrolithiasis. A computed tomographic examination was ordered, the results of which were negative for kidney stones and appendicitis but positive for a right ovarian mass. The patient was sent for pelvic sonography, which showed a normal uterus and left ovary and a large, diffusely heterogeneous, prominently vascularized right ovary measuring 4.6 × 4.0 × 2.8 cm. She was released from the emergency department with instructions to follow-up with her gynecologist.
Approximately 7 weeks later after consultation with her gynecologist, the patient underwent follow-up pelvic sonography, which again reported a normal uterus and left ovary. The right ovary, which remained heterogeneously enlarged and prominently vascularized, had approximately quadrupled in size to 6.5 × 4.3 × 5.1 cm. Sonographic findings were correlated with serum tumor markers, which were all within normal limits. A recommendation was made for another sonographic follow-up examination in 2 months before surgical intervention was to be considered.
The third pelvic sonogram, performed approximately 2 months later, demonstrated a uterus and left ovary within normal limits and, again, enlargement and diffuse heterogeneity of the right ovary, not significantly changed from the previous examination, measuring 5.7 × 3.9 × 5.3 cm (Figure 1A). Vascularity within the ovary again appeared prominent but normal (Figure 1B). As the patient was asymptomatic at this time and doing well and the tumor markers remained within normal limits, the gynecologist chose to follow the right ovary with yet another ultrasound in 3 months. On that visit, the ovarian mass had increased marginally in size to 6.5 × 3.0 × 5.5 cm, but of more concern was the appearance of a focal, solid, hypoechoic mass within the ovary measuring approximately 3.1 × 2.8 × 4.0 cm (Figure 2A). Persistent, prominent, but normal intraparenchymal blood flow was noted with color Doppler imaging (Figure 2B). The patient was sent for a gynecologic oncology consult, and laparoscopic evaluation was recommended despite the repeatedly normal tumor markers. At surgery, the right ovary was found to be torsed, twisted 3 times on the vascular pedicle; however, arterial and venous flow were not completely disrupted. After detorsing, the ovary was determined to be viable and began to decrease in size. The patient had an uneventful recovery and, 8 months later, returned for a follow-up postoperative pelvic sonogram, which showed a right ovary of normal size and appearance (Figure 3).
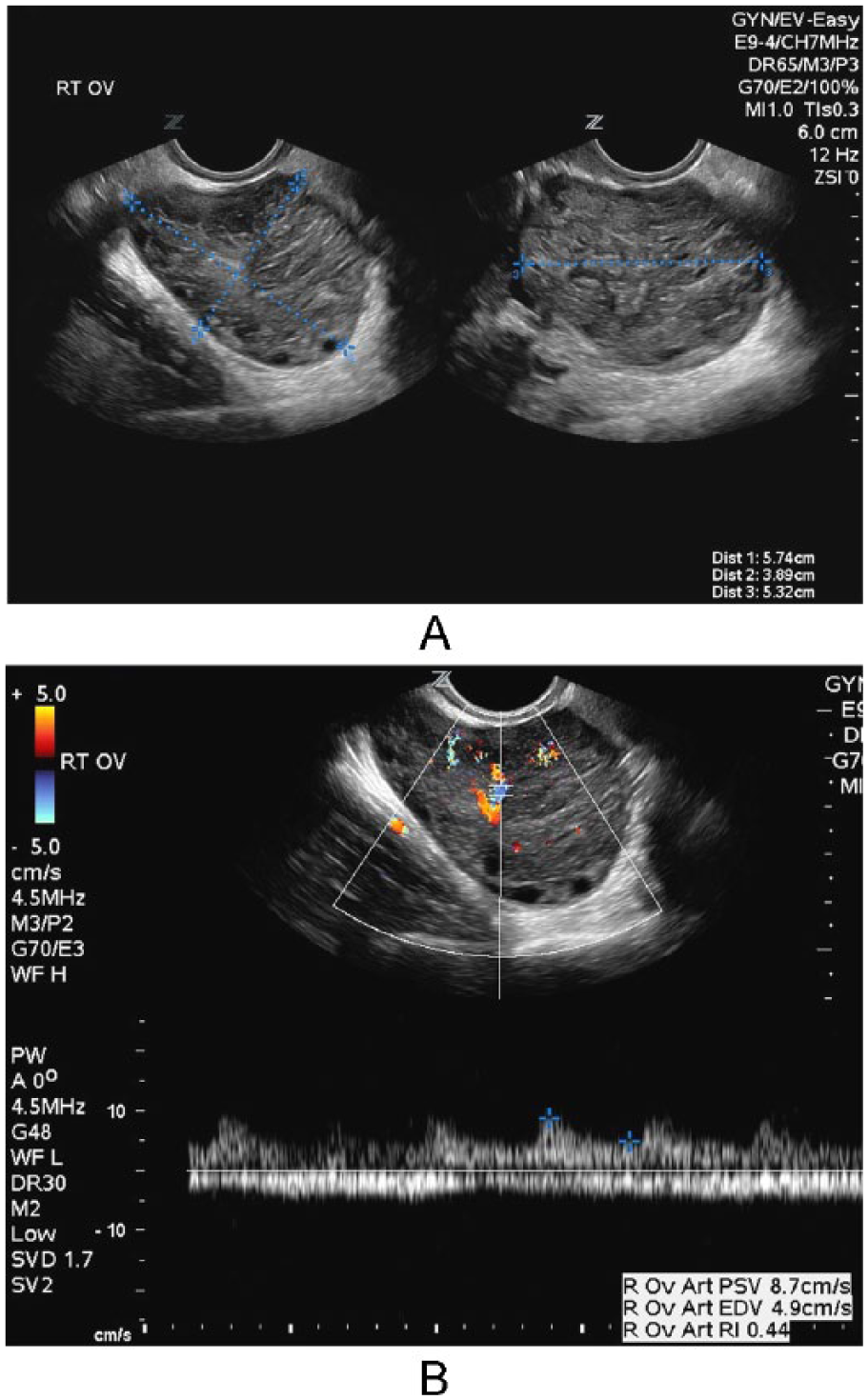
A, Longitudinal (left) and transverse (right) gray-scale endovaginal images (taken approximately 4 months following the initial computed tomographic examination) through the right adnexa, demonstrating an enlarged, diffusely heterogeneous right ovary. B, Color and spectral Doppler endovaginal image of the enlarged right ovary (taken approximately 4 months following the initial computed tomographic examination) demonstrating typical venous and low-resistance arterial flow patterns within the ovarian parenchyma. There is prominent but normal intraparenchymal vascularity.
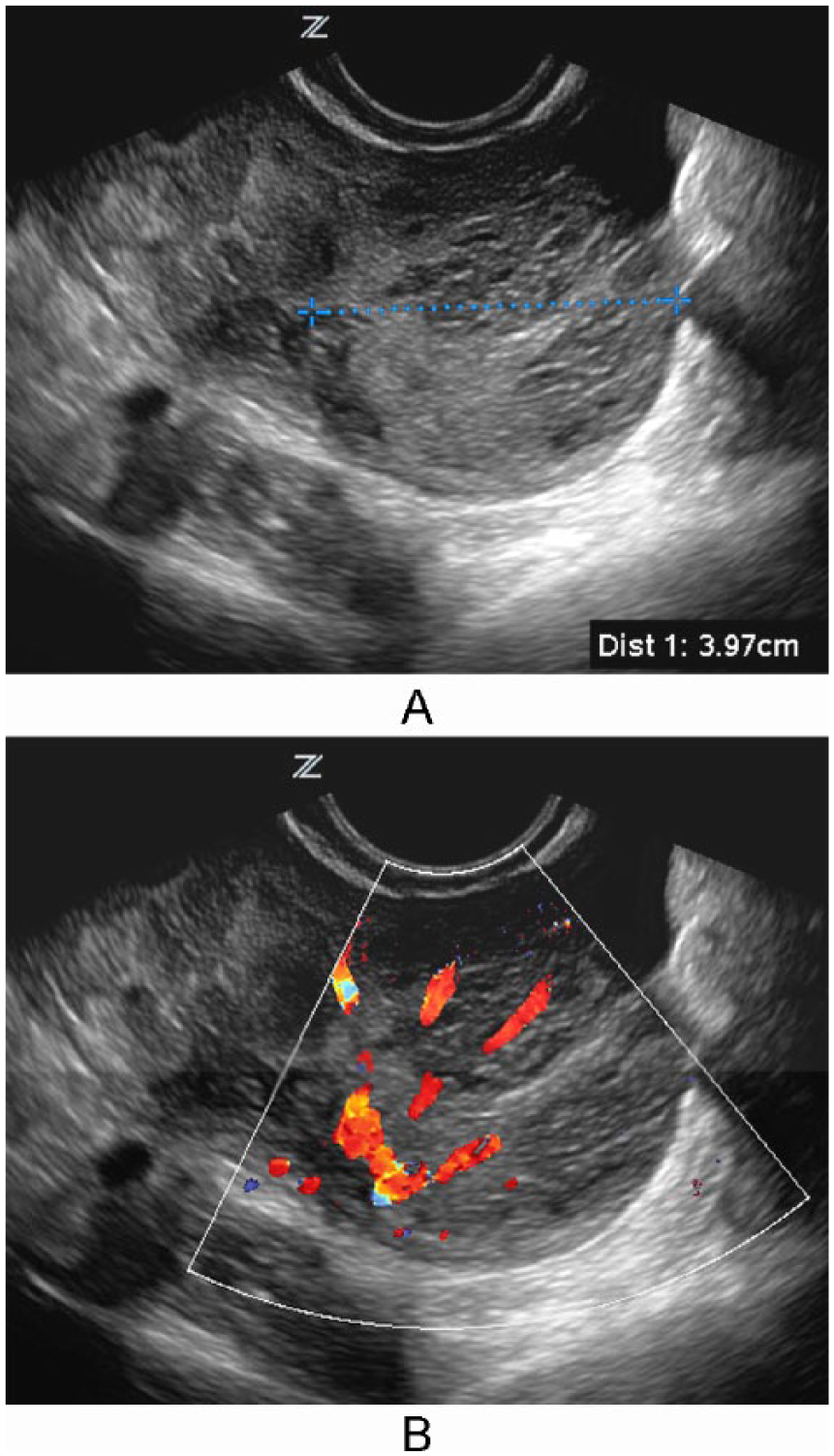
A, Endovaginal gray-scale image of the enlarged ovary (taken approximately 7 months following the initial computed tomographic examination) with a 4-cm focal mass noted within (cursors). B, Endovaginal color Doppler image of the enlarged ovary (taken approximately 7 months following the initial computed tomographic examination) showing persistent, prominent, but normal intraparenchymal vascularity.
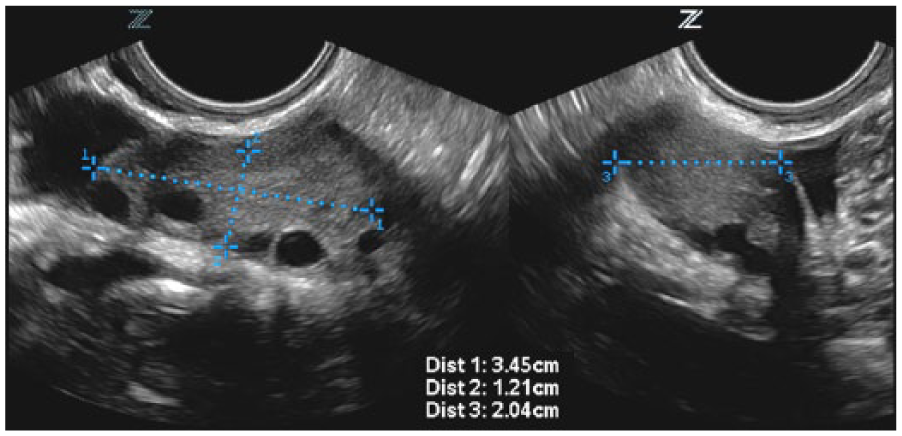
Longitudinal (left) and transverse (right) endovaginal gray-scale images obtained 8 months postoperatively demonstrating a normal right ovary.
Discussion
Ovarian torsion is one of a few gynecologic surgical emergencies. It has a bimodal age distribution, being more common in young (15 to 30 years) and postmenopausal women. 1 Typical clinical findings include acute pelvic pain accompanied by nausea and vomiting and tenderness on abdominal and adnexal palpation. Hypermobility of the ovary—particularly in association with pregnancy and adnexal masses such as mature cystic teratomas and paraovarian cysts—increase the risk of the ovary twisting on its vascular pedicle. 2 Strangulation of the arterial inflow produces the acute symptoms experienced by affected patients and creates the potential for ischemic organ loss. Venous and lymphatic obstruction result in edematous enlargement of the ovary and the seepage of fluid, which typically collects in the posterior cul de sac.
Sonography has become the primary imaging modality for evaluation of patients with suspected ovarian torsion. Typical and well-established B-mode sonographic findings include unilateral ovarian enlargement with cystic lesions, peripherally displaced ovarian follicles, uterine deviation toward the side of torsion, and free fluid in the posterior cul de sac. 3 The identification of a focal, solid mass within a torsed ovary, as demonstrated in this case, is suggestive of a chronic ischemic process but is seen only in approximately 5% of cases.4,5
Doppler findings associated with ovarian torsion vary with the degree of perfusional disruption present in a particular case. If arterial inflow is completely compromised, no flow will be observed in the ovarian parenchyma with color or power Doppler imaging modalities. Complete absence of flow in a patient with acute pelvic symptoms is a strong indication that the ovary may not be viable, and immediate intervention is usually warranted. 6 More commonly, some arterial flow to the ovary persists, either through the residual lumen of an incompletely obstructed vessel or via collateral branches arising from the uterine artery. In such cases and as presented in this report, color and power Doppler will demonstrate intraparenchymal flow, although it may appear diminished when compared to the contralateral ovary.
Conclusion
Sonographic imaging has long been the modality of choice in evaluating patients with suspected ovarian torsion. While the commonly accepted pathognomonic finding in a torsed ovary is absent blood flow using Doppler imaging modalities, as demonstrated in this case, the identification of intraparenchymal ovarian flow does not rule out a diagnosis of ovarian torsion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.