
Abstract
Cultural awareness is an emerging issue in the field of sonography. A cross-sectional study of cultural awareness was conducted in the northeastern United States through a professional echocardiography society. Of the 101 sonographer members, 67 (66%) participated in the survey, which addressed the following questions: What is the level of cultural awareness of the cardiac sonography membership of a suburban northeastern United States professional echocardiography society, and how does this relate to the number of years that the respective sonographers have been practicing in the field of echocardiography? Results of the study showed no significant relationship between cultural awareness and the total number of years of scanning experience, suggesting that cardiac sonographers did not gain cultural awareness because of the transcultural experiences they encountered.
Health care in the United States is going through an evolution, with increasing emphasis on providing culturally competent health care. Achieving cultural competency is a 2-step process: obtaining cultural information, which translates into developing cultural awareness, and applying the cultural knowledge. 1 In the field of cultural training, the terms cultural awareness and cultural competency are often used interchangeably, although cultural awareness is a subset of cultural competency. According to Betancourt et al, cultural competence in health care describes the ability of systems to provide care to patients with diverse values, beliefs, and behaviors, including tailoring delivery to meet patients’ social, cultural, and linguistic needs. 2
In 2003 at the request of the US Congress, the Institute of Medicine’s Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care conducted a study for assessing differences in the kinds and quality of American health care. 3 The Institute of Medicine study developed 5 key findings indicating unequal treatment in health care. Two of these findings directly related to services provided by echocardiographers. According to Scott et al, the first finding was that “racial and ethnic disparities in health care exist even when insurance status, income, age, and severity of conditions are comparable. Death rates from cancer, heart disease, and diabetes are significantly higher in racial and ethnic minorities than in whites.” 3 The exact etiology of this ethnic disparity can be determined only by prudent evaluation of every component of health care, including the field of echocardiography.
A transthoracic echocardiogram is a common diagnostic tool for the diagnosis or monitoring of heart disease. 4 Garroutte et al 5 showed that “small differences in patient perceptual measures can be quite meaningful in their relationship to health outcomes and should be taken seriously.” Cardiac sonographers with low levels of cultural competency could contribute to the etiology of the racial or ethnic disparity within the scope of echocardiography. A transcultural interaction could result in miscommunication between the patient and the sonographer. An apprehensive patient may be less forthcoming with pertinent medical information, which could negatively influence the echocardiogram examination.
Low levels of cultural competency could also be responsible for the second finding within this Institute of Medicine study: “Bias, stereotyping, prejudice, and clinical uncertainty on the part of health care providers may contribute to racial and ethnic disparities in health care.” 3 Bias, prejudice, and clinical uncertainty have been shown to result in detrimental health care in a nursing cultural competency study. 6 Therefore, the ability to identify health care bias or prejudice through an established tool such as the Cultural Self-efficacy Scale presents an opportunity to modify these behaviors. 7 Kardong-Edgren’s study showed that cultural competency can be increased with cultural training classes, with those that incorporate firsthand interaction with diverse cultural groups being the most effective. 7
Cultural awareness has recently been added to the standards for approved study in the field of diagnostic cardiac sonography. In the standards for both the Joint Review Committee on Education in Cardiovascular Technology (revised 2010) 8 and the Joint Review Committee on Education in Diagnostic Medical Sonography (revised 2011), 9 members of the Commission on Accreditation of Allied Health Education Programs state that approved programs “must identify and respond to changes in the needs and/or expectations of its communities of interest.” 9 As diversity is being embraced in the United States, the needs and expectations of the communities of interest are quickly expanding. Consequently, this is creating a challenge for sonographers to develop cultural awareness since the needs and expectations of the communities of interest vary, making cultural training unique to regional needs and expectations.
A review of the literature showed that numerous other institutions of medical training, such as medical schools, nursing programs, and physical therapy programs, have studied the significance of cultural awareness and cultural competency. These medical fields have incorporated curriculum changes that provide enhanced cultural training, making those health care professionals more prepared to serve the increasingly diverse American population. There is evidence of legislative support for competency education for physicians, nurses, and other health professionals. The Liaison Committee on Medical Education mandated that medical schools provide training in cultural and belief systems, as they affect health care. 10 The committee has made the fundamental assumption that basic principles of culturally competent health care will enable the physician to recognize situations in which a patient’s culture may be a factor in determining treatment.
Materials and Methods
The purpose of this study was to assess the current level of cultural awareness of practicing cardiac sonographers. This level will provide a cultural awareness baseline of practicing echocardiographers that will produce a starting point for the field of echocardiography to keep pace with other health care fields. The study investigated the following research questions: What is the level of cultural awareness of the cardiac sonographer membership of a suburban northeastern US professional echocardiography society, and how does this relate to the number of years that the respective sonographers have been practicing in the field of echocardiography?
Research Design and Rationale
The study was a cross-sectional study design, which used a questionnaire to provide quantitative data. The design was selected because the current levels of cultural awareness in the field of echocardiography have not been measured. The quantitative design provided an unambiguous benchmark of the existing levels of cultural awareness in the field of echocardiography. The interpretation of the quantitative data indicated the participants’ current levels of cultural awareness. Low levels of cultural awareness were identified in some of the participants; future patients may benefit from if cultural awareness training were provided to these sonographers. New benchmarks can be used to evaluate the effectiveness of future cultural awareness training.
Participants
Members of a professional echocardiography society in the northeastern United States were the participants in the study. The society membership represented a 100-mile radius from a major metropolitan city. The region encompassed parts of 3 states and a variety of settings, ranging from metropolitan to rural. The society is composed of cardiologists, anesthesiologists, cardiac sonographers, and cardiac ultrasound students. Only the 101 cardiac sonographer members of the society were invited to participate because the cultural awareness of practicing sonographers was the variable to be measured in the study. The society members were invited to participate in the study during a presentation at one of the biannual membership meetings, and an e-mail invitation was sent to all sonographer members. The e-mail contained a link to the survey and a password that enabled them to access the questionnaire. The e-mail invitation contained the participation letter and indicated that by clicking on the link, they were giving their consent to participate. A link to the survey was also posted on the society webpage. After the initial e-mail was sent, reminder invitations to participate in the study were sent at 14-day intervals for the remainder of time that the survey was available.
Survey
The tool adapted for this study was the Cultural Awareness Assessment Tool (see Appendix A). Electronic permission to adapt and use it was granted by the F. A. Davis Company. It was identified by Flowers as an effective self-assessment tool to determine a person’s cultural awareness. 11 Catalano cautioned that learning about another person’s culture does not guarantee cultural awareness; one must first understand one’s own cultural background and explore one’s own prejudiced and biased views of others. 12 The tool was designed to assess the cultural awareness of nurses but was easily adapted to assess cardiac sonographers. The questions in the tool assessed bias toward patients of another culture. The tool can be used to assess awareness of many cultural differences other than obvious ethnic differences, including alternative lifestyles, race, age, and gender. The tool also assessed the health care practitioner’s perception of the dynamic that occurs during a transcultural interaction. The adapted data collection tool was tested for reliability and validity. A focus group of 6 practicing cardiac sonographers analyzed the instrument for reliability and validity and provided their recommendations as needed.
Reliability
Reliability analysis of the Cultural Awareness Assessment Tool was computed, and a Cronbach’s alpha of .734 was obtained, indicating that the 17 items for this scale measured a similar construct: cultural awareness. An alpha of .700 or better is considered acceptable in social science research. 13
Results
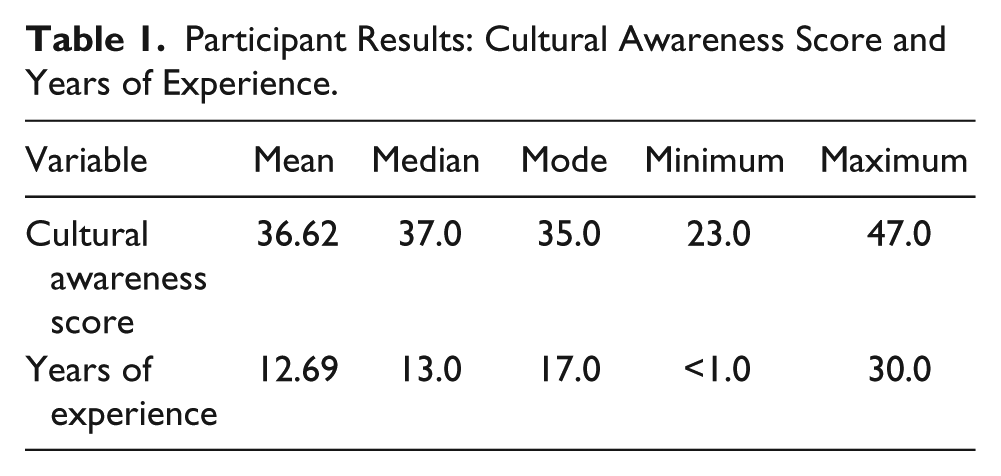
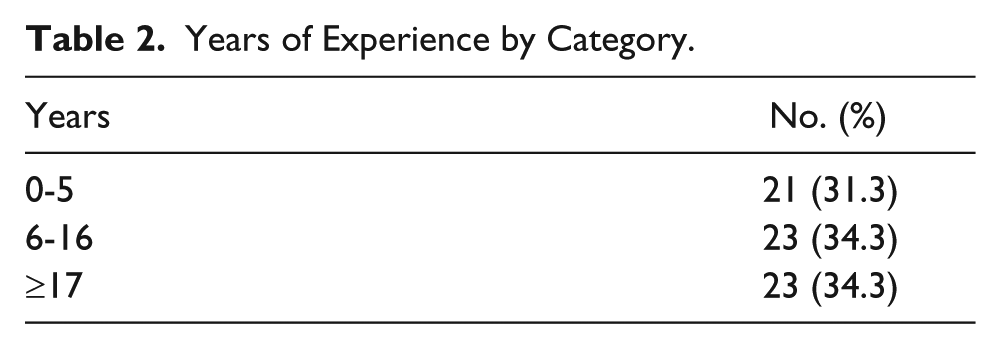
It was assumed that the number of random transcultural patient interactions would increase with the number of years that a sonographer had practiced. The null hypothesis (H0) was the following: The cultural awareness scores of the practicing cardiac sonographers were unaffected by the years of experience. The research (H1) hypothesis was that cultural awareness scores would increase with the years of experience. The mean cultural awareness score for the sample group was 36.62 out of a possible 54.00 points, and the mean experience for the sample group was 12.69 years (Table 1). The independent variable, years of experience, was recoded into 3 categories: 0-5 years of experience, 6-16 years, and 17 or more years (Table 2). The percentage of participants in each of the 3 categories was, respectively, 31.3%, 34.3%, and 34.3%.
Participant Results: Cultural Awareness Score and Years of Experience.
Years of Experience by Category.
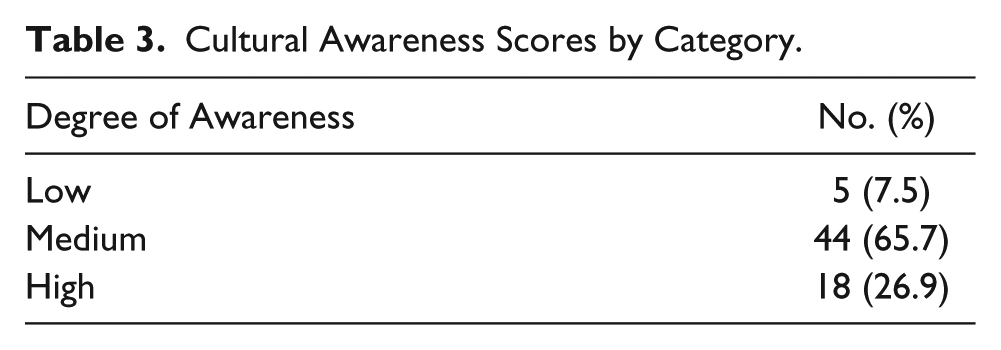
The cultural awareness scores of the participants were coded into 3 categories—low degree (17-29 points), medium degree (30-39 points), and high degree (40-51 points) of cultural awareness—based on the scale’s scoring protocol. The percentages of participants in each of the 3 cultural awareness score categories were as follows (Table 3): low degree, 7.5% (n = 5); medium degree, 65.7% (n = 44); and high degree, 26.9% (n = 18).
Cultural Awareness Scores by Category.
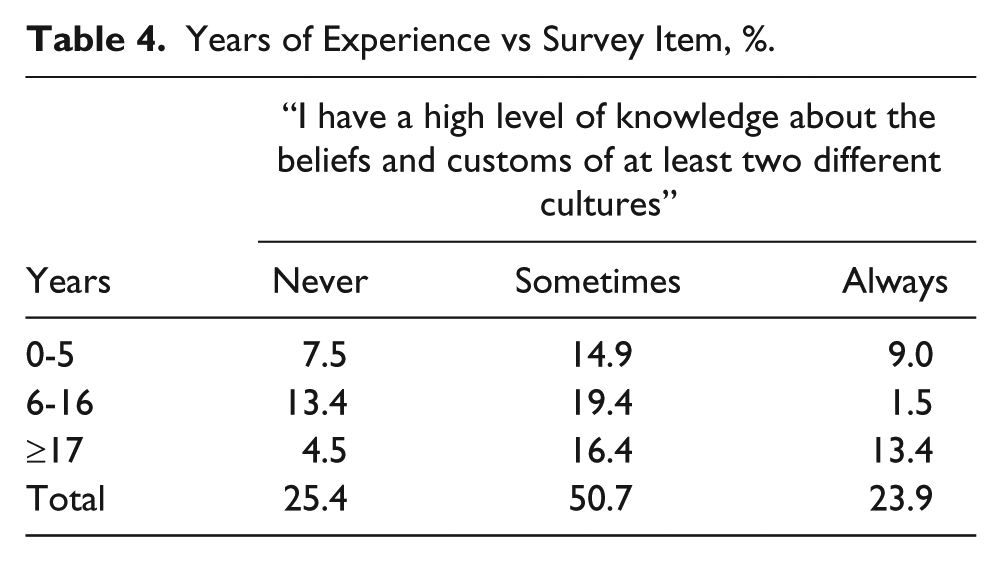
Only one item—“I have a high level of knowledge about the beliefs and customs of at least two different cultures”—was significant across the experience categories (χ2 = 8.735, P < .05). Post hoc analysis based on the Mann Whitney U test found that those respondents with 17 or more years of experience were more likely to respond sometimes or always to this statement compared to those respondents with between 6 and 16 years of experience (Z = −2.941, P < .01). There was a trend toward significance with respondents who had performed echocardiograms for 5 or fewer years being more likely to respond positively to this statement compared to those respondents with 6 to 16 years of experience (Z = −1.841, P < .10; see Table 4).
Years of Experience vs Survey Item, %.
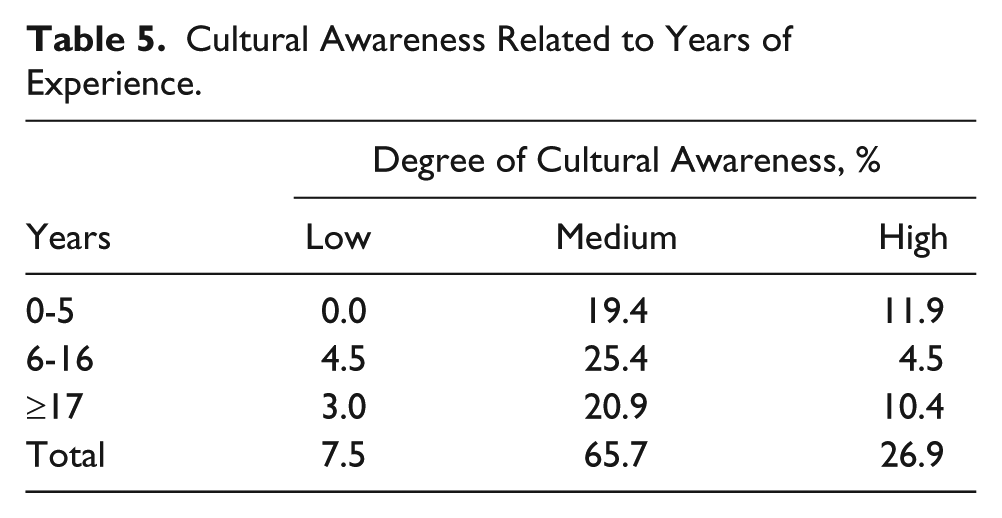
For all respondents, there was no significant relationship between the cultural awareness score and total number of years of experience (r = −.033, P = .793). When data were categorized into groups, there was a trend toward significance for categories of low, medium, and high degrees of cultural awareness and years of experience (χ2 = 5.069, P < .10; see Table 5). Post hoc analysis based on the Mann Whitney U test found that those respondents with 5 or fewer years of performing echocardiograms were more likely to have scored in the high degree of cultural awareness compared to those respondents with 6 to 16 years of experience (Z = −2.301, P < .05; see Table 5).
Cultural Awareness Related to Years of Experience.
Discussion
There was no significant relationship between cultural awareness and the total number of years of experience, suggesting that cardiac sonographers did not gain cultural awareness because of transcultural experiences encountered. Consequently, during subsequent examinations on transcultural patients, cardiac sonographers likely had the same level of cultural awareness and were unprepared to provide more culturally sensitive care to them. Exposure to transcultural patients for cardiac sonograms through a sonographer’s professional career represents an opportunity to become more familiar with the cultures of others. Greater cultural understanding generated from each transcultural interaction adds to the sonographer’s cultural repertoire if one is cognizant of the opportunity. Otherwise, the sonographer’s level of cultural awareness will remain the same, and future transcultural echocardiography examinations will have no greater cultural sensitivity to address an increasingly diverse patient population.
Respondents’ cultural awareness scores indicated that 26.9% had a high degree of cultural awareness. The remaining scores represent an opportunity to improve cultural aspects of health care by providing additional training to the 65.7% of respondents who had a medium degree of awareness and the 7.5% who had a low degree. There was a trend toward significance with respondents who had performed echocardiograms for 5 or fewer years being more likely to have scored in the high degree of cultural awareness compared to those respondents with 6 to 16 years. The Kruskal-Wallis test was conducted to determine if there were significant differences between years of experience and the respondents’ ratings; for all but 1 of the 17 items on the Cultural Awareness Assessment Tool, there were no differences in respondents’ ratings of never, sometimes, and always based on the categories of years of experience in performing echocardiograms. Only one item—“I have a high level of knowledge about the beliefs and customs of at least two different cultures” (see Appendix A)—was significant across the experience categories. Respondents reporting 17 or more years of experience were more likely to respond sometimes or always to this statement compared to those respondents reporting between 6 and 16 years of experience. This may be due to the greater probability of their having had transcultural experiences during the extended time span of their cardiac sonography career. There was a trend toward significance with respondents who had performed echocardiograms for 5 or fewer years being more likely to respond positively to this statement compared to those respondents with 6 to 16 years of experience. This may have been the result of casual exposure to greater diversity among classmates.
The results of this research strongly suggest that there is no correlation between one’s cultural awareness score and one’s years of experience as a sonographer performing echocardiography examinations. The lack of a significant relationship between the cardiac sonographers’ cultural awareness scores and their total years of experience suggests that they did not gain cultural awareness as a result of their transcultural experiences encountered. As the diversity increases among our communities of interests, it reduces our ability to address this challenge by simply painting cultural training with a broad brush, since the needs and expectations vary so greatly. However, our ability to recognize changes in needs and expectations in our local communities of interest represents an opportunity to improve our contribution to patient care by valuing these new needs and expectations. As we embrace the value of the new needs and expectations, an ethos of greater cultural awareness will acclimate sonographers to the value of diversity.
Footnotes
Appendix A:
Appendix B:
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.